
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-200
How to Overcome Radial Artery Spasm When PCI? Old Technique but Not Outdated
By Tung Ngo, Quan Manh Nguyen
Presenter
Tung Ngo
Authors
Tung Ngo1, Quan Manh Nguyen1
Affiliation
Vietnam National Heart Institute, Vietnam1,
View Study Report
TCTAP C-200
Coronary - Vascular Access and Closure
How to Overcome Radial Artery Spasm When PCI? Old Technique but Not Outdated
Tung Ngo1, Quan Manh Nguyen1
Vietnam National Heart Institute, Vietnam1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A male patient with a history of hypertension and long-term smoking, without a history of diabetes or dyslipidemia, was admitted due to intermittent left-sided chest pain, shortness of breath, sweating, and a feeling of dizziness that began 12 hours before hospitalization. Physical examination revealed no significant findings, and vital signs at admission were stable: heart rate of 56 beats per minute and blood pressure of 150/90 mmHg. The patient was diagnosed with acute myocardial infarction.
Relevant Test Results Prior to Catheterization
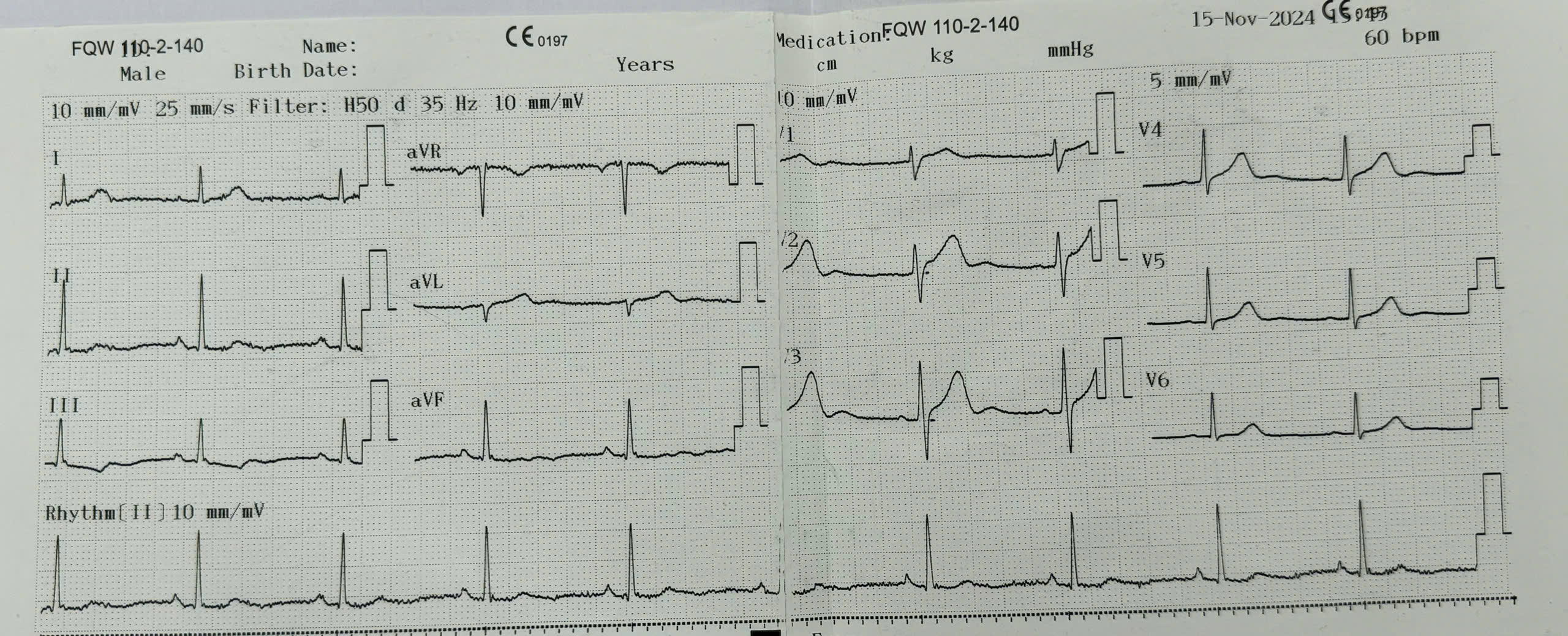
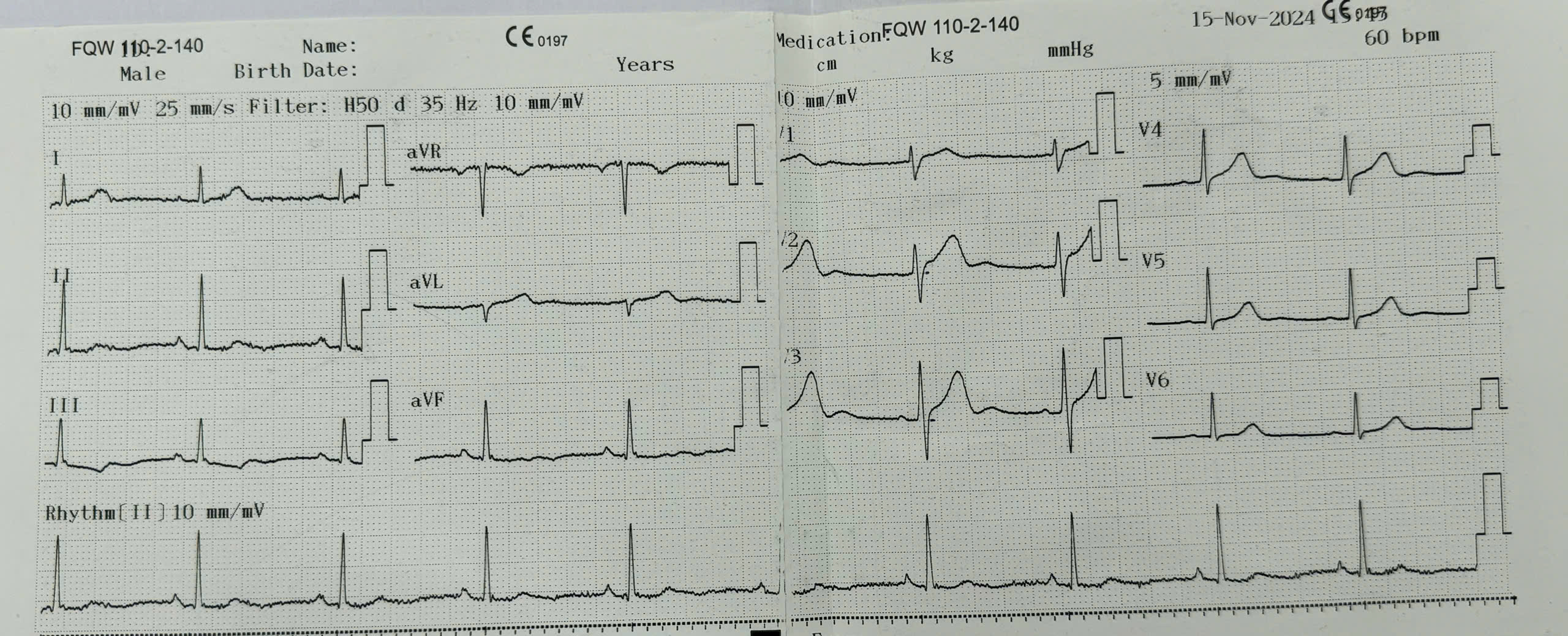
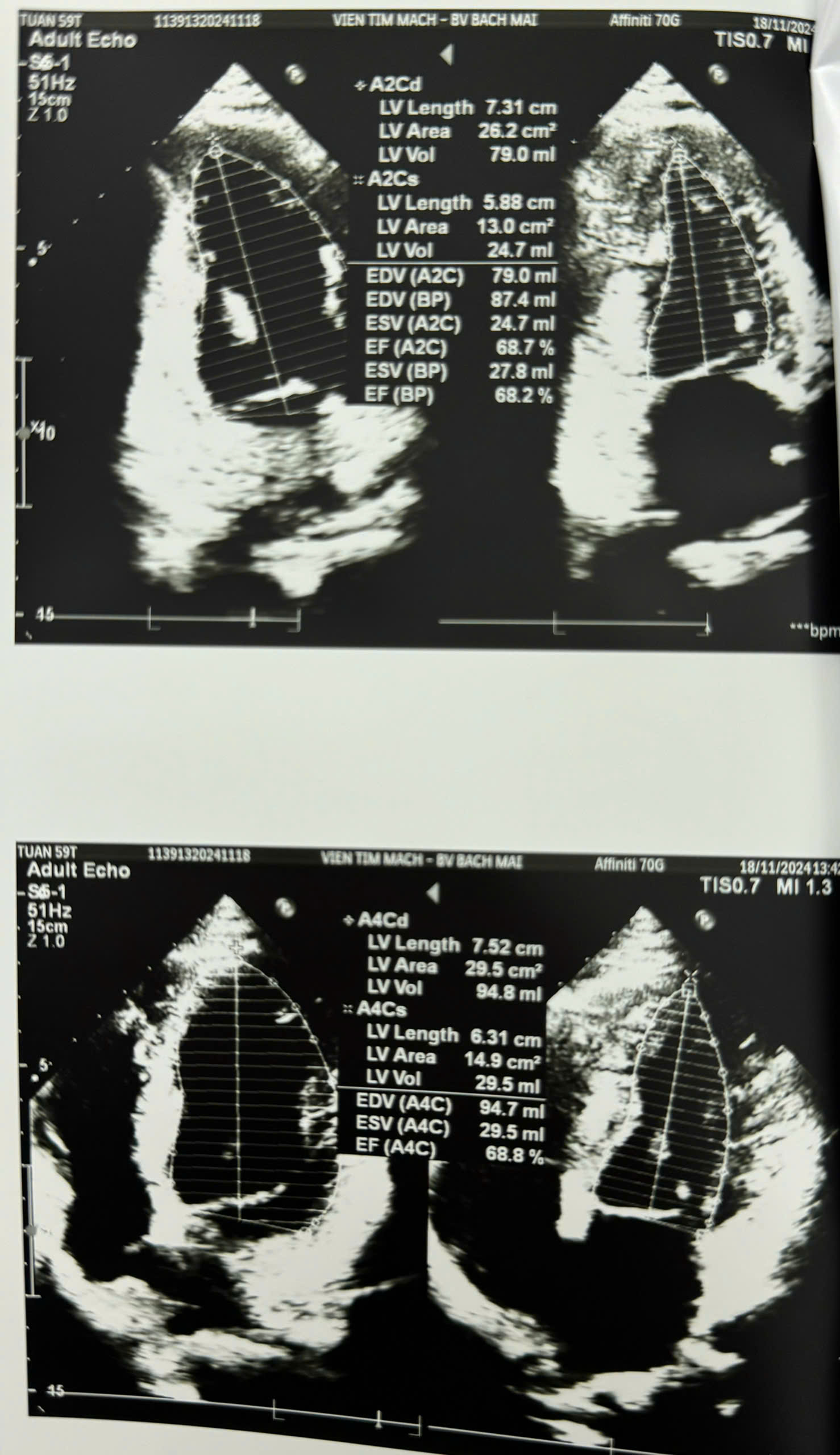
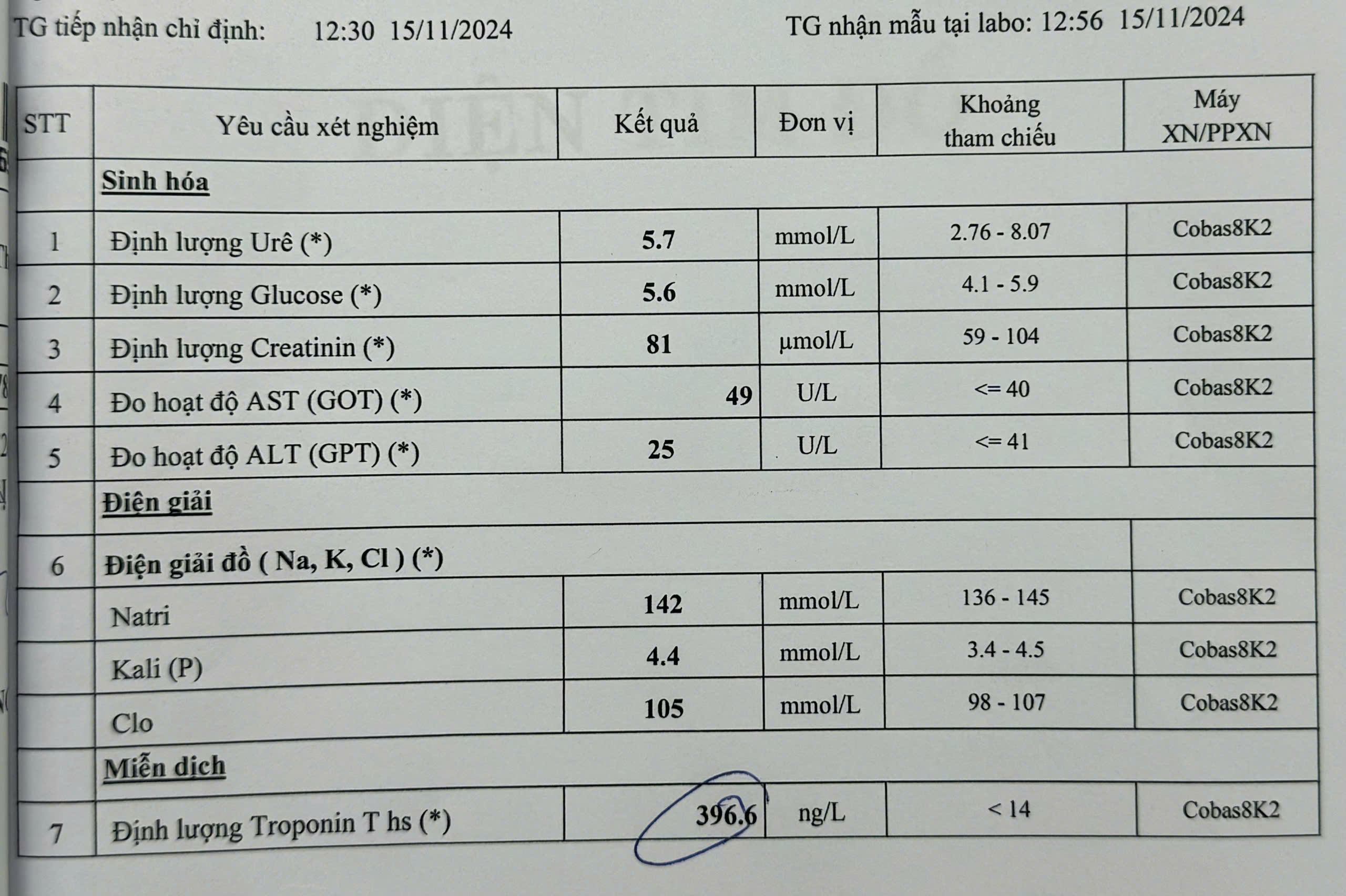
*Electrocardiogram (ECG): Sinus rhythm, intermediate axis, and inverted T waves in leads D2 and aVF.*Echocardiography: No apparent regional wall motion abnormalities, with preserved cardiac function.*Biochemical tests: High-sensitivity Troponin T markedly elevated.
Relevant Catheterization Findings
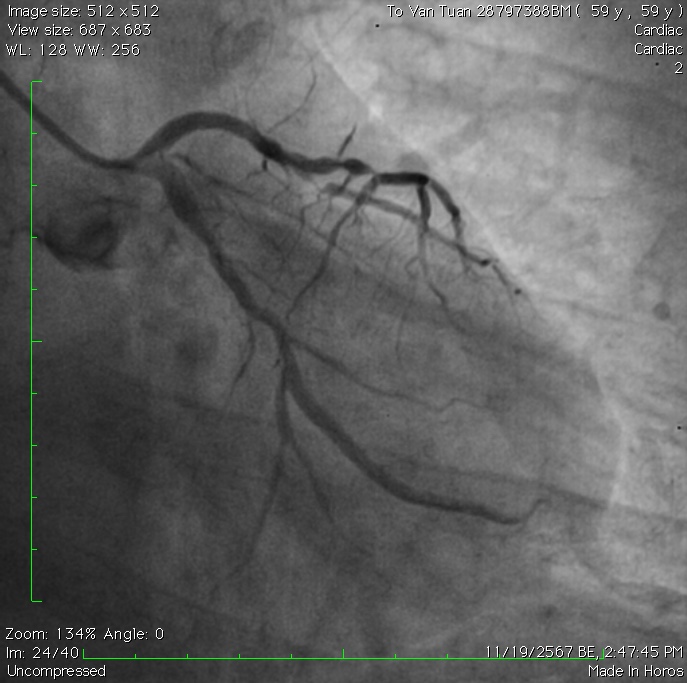
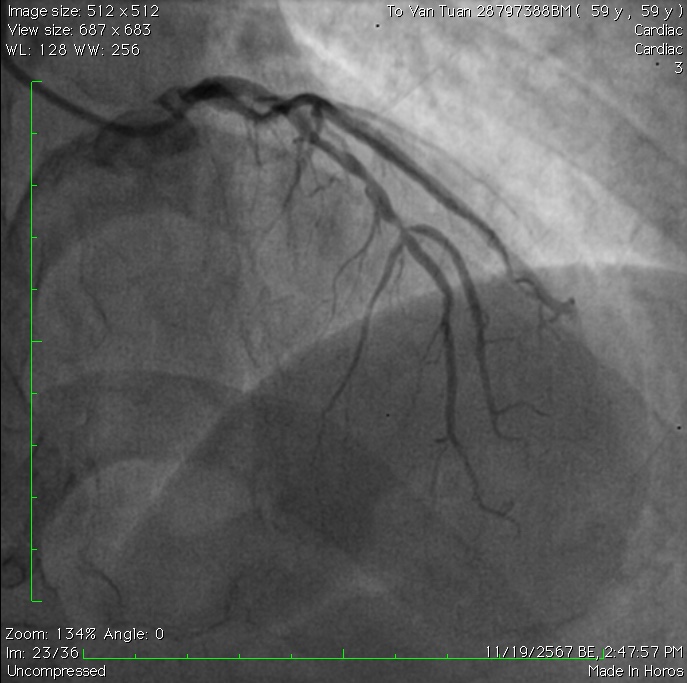
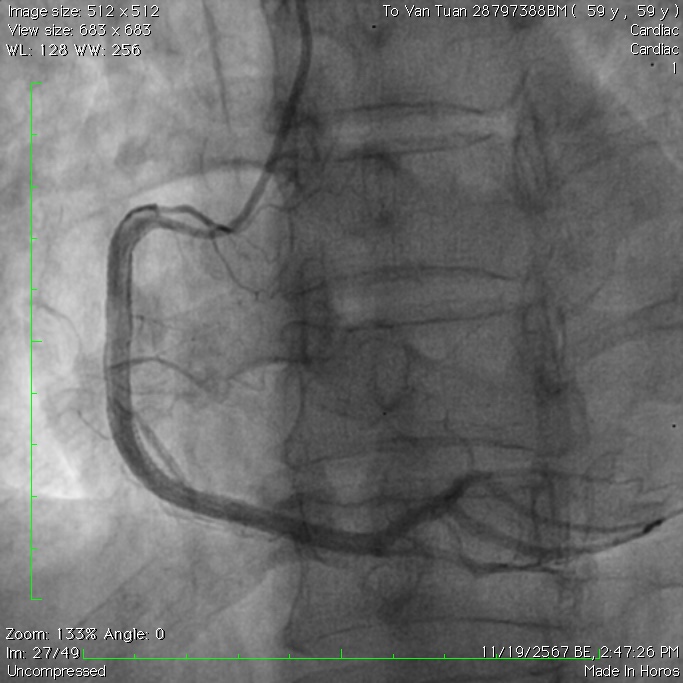
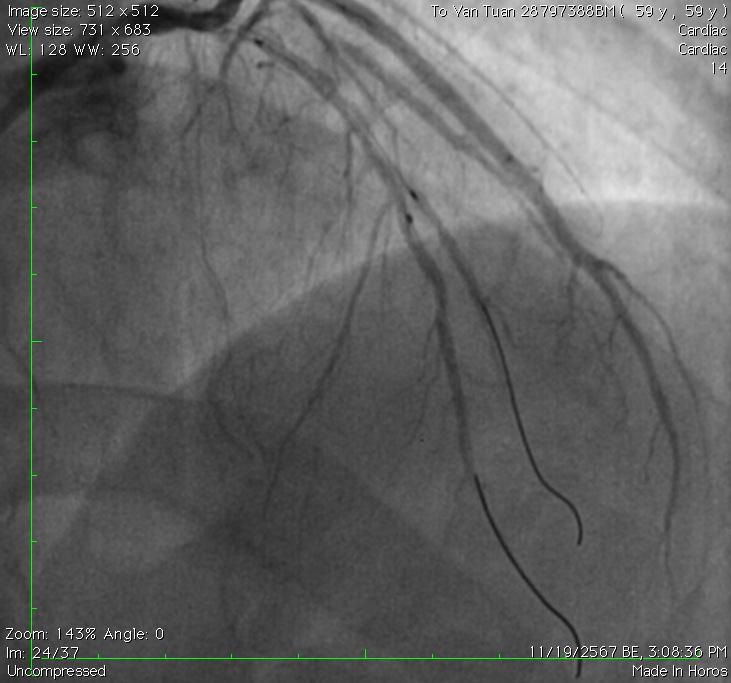
Coronary angiography results: Complete occlusion of the mid-right coronary artery (RCA) was treated with two drug-eluting stents (DES) during the initial intervention. In this follow-up angiography for LAD intervention, the RCA stents were patent. The LAD showed moderate stenosis (40-50%) from segment I to II and severe stenosis (95%) at segment II at the bifurcation with the second diagonal branch (D2). The left circumflex artery (LCX) had no significant stenosis.
Interventional Management
Procedural Step
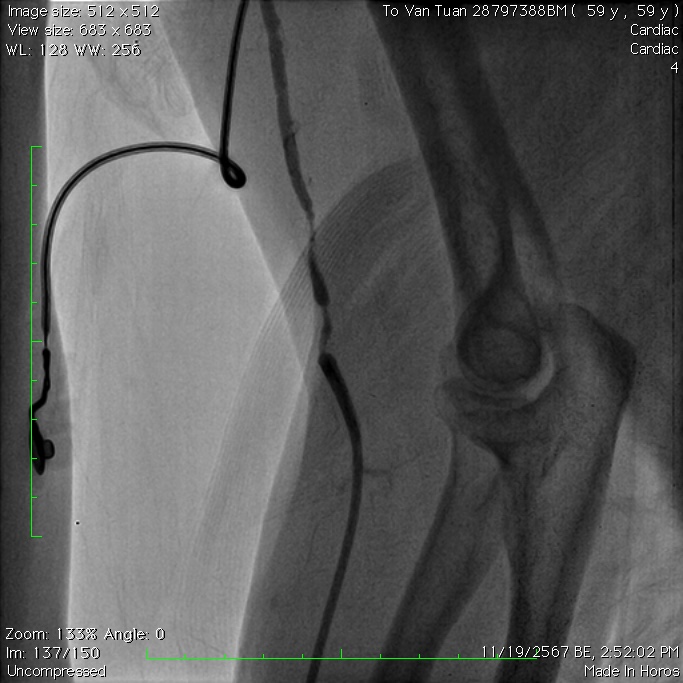
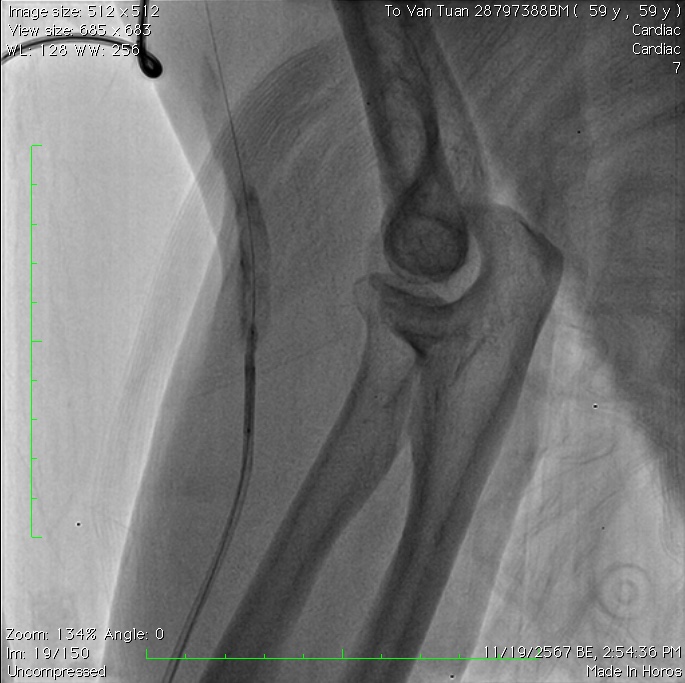
We initially planned to access the right radial artery for the intervention on the LAD segment II, but as it was inaccessible, we switched to the left radial artery. After reassessing the RCA stents and LAD lesions via angiography, we prepared to advance a 6F EBU guiding catheter through the left radial artery. However, radial artery spasms prevented further advancement of the guiding catheter. Intravenous Nitroglycerin and intramuscular Diazepam were administered, but left radial angiography still revealed significant spasm. We utilized a 2.0 x 20 mm balloon positioned halfway inside and halfway outside the guiding catheter tip and inflated it to 6 mmHg. This allowed the guiding catheter to advance smoothly. The intervention was performed via the left radial artery, addressing the LAD-D2 bifurcation using the jailing balloon technique and small balloon dilatation of the severe stenosis in the D1 branch.
Case Summary
The "tracking balloon" technique, though considered an older method, remains highly effective in overcoming challenging radial artery spasms during coronary interventions. By enabling the smooth advancement of guiding catheters in cases where pharmacological measures fail, this approach highlights the enduring value of time-tested techniques in modern interventional cardiology. This technique helps patients avoid complications associated with large arterial access, reduces hospital stay duration, and enhances patient comfort.