
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-098
Simple Approach to Complex CTO Lesson
By Mir Nesaruddin Ahmed, Prof. Fazila Tun-Nessa Malik, Md Shamim Chowdhury, Md Kalim Uddin, Prof. Nazir Ahmed
Presenter
Mir Nesaruddin Ahmed
Authors
Mir Nesaruddin Ahmed1, Prof. Fazila Tun-Nessa Malik1, Md Shamim Chowdhury1, Md Kalim Uddin1, Prof. Nazir Ahmed1
Affiliation
National Heart Foundation Hospital & Research Institute, Bangladesh1,
View Study Report
TCTAP C-098
Coronary - Complex PCI - CTO
Simple Approach to Complex CTO Lesson
Mir Nesaruddin Ahmed1, Prof. Fazila Tun-Nessa Malik1, Md Shamim Chowdhury1, Md Kalim Uddin1, Prof. Nazir Ahmed1
National Heart Foundation Hospital & Research Institute, Bangladesh1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
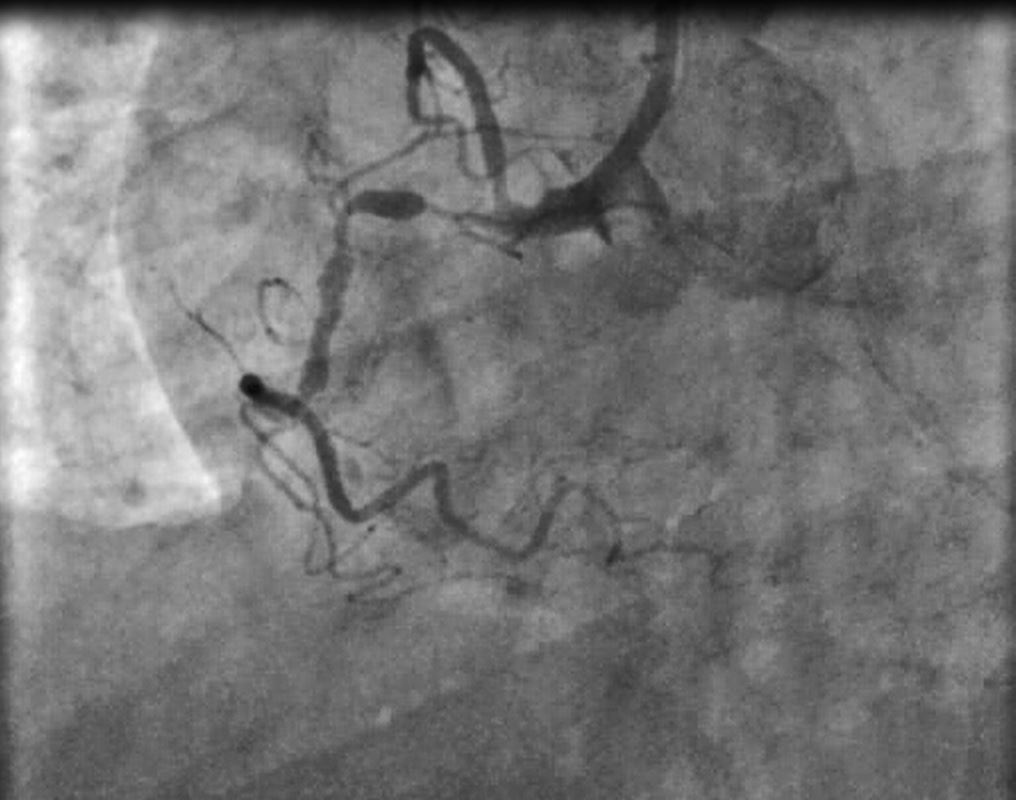
Mr. X 70yrs old hypertensive diabetic patient admitted with complains of exertional chest pain ( CCS class iii). His vitals were stable with NYHA Class II. He underwent Coronary angiogram which revealed Single vessel CAD ( 99% stenosis in proximal lesson followed by 100% occlusion from the mid segment of RCA with ipsi-lateral faint filling).
Relevant Test Results Prior to Catheterization
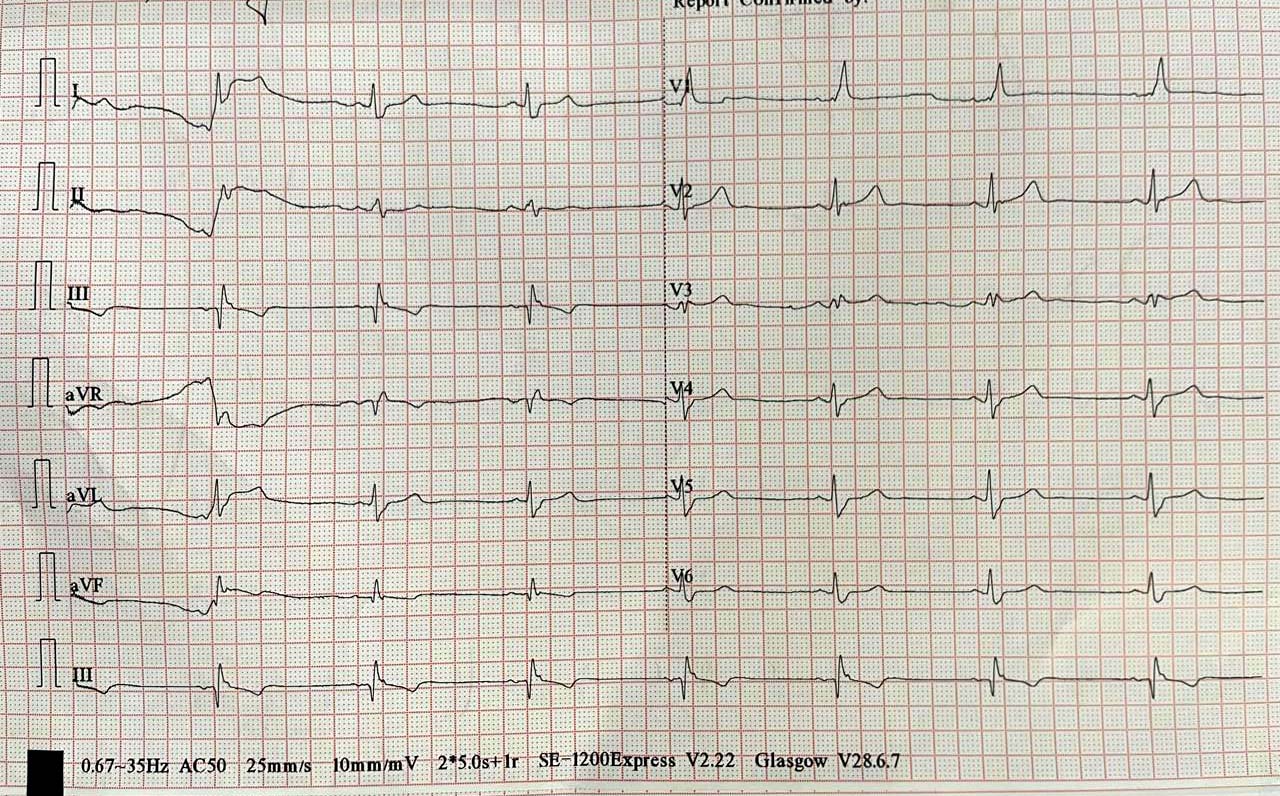
Lab reports: CBC: Hb-13.3 gm/dl;TC: 8000 / mm3; Blood group : B negative, S. creatinine: 1.5 mg/dlECG: Incomplete RBBB, Echo: IHD with LVEF : 40%, Dilated LA & LV; . Coronary Angiography Findings : His Left coronary artery revealed no significant disease; RCA (Dominant vessel) -CTO from mid Segment with blunt stump with highly tortuous vessel. Gensini score : Euro CTO score 3 & J CTO score 3.
Relevant Catheterization Findings
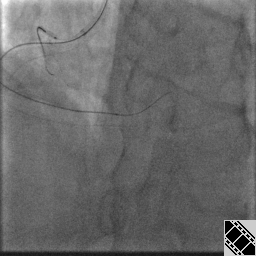
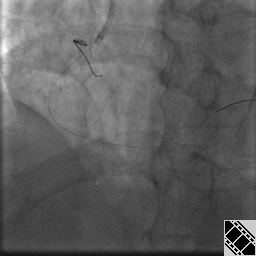
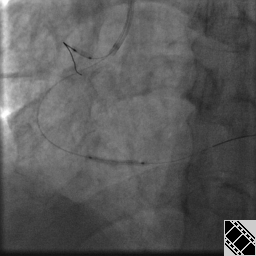
Anti grade wire escalation technique was used to cross the lesion with the support of anchor balloon technique. first micro catheter was taken with runthrough floppy wire. For lesion crossing pilot 50 hydrophilic followed by fielder XT wire were used. Wire crossing time was 34 min. After lesion preparation with NC balloon, Two sirolimous coated stents were implanted (2.5 X38 mm from mid portion to distal RCA and another 2.75 X 48 mm in the proximal portion). Procedure was uneventful.
Interventional Management
Procedural Step
We cross the RCA CTO lesion with ante-grade wire escalation technique with anchor balloon support.Hydrophilic wire (Pilot-50, Fielder XT ) Were used with the help of micro catheter. After proper lesion preparation with NC balloons ,just after the dilatation dissection was found from the mid portion of the RCA. Two Drug eluting stents (Sirolimous) were deployed at proximal & mid to distal portion of RCA. a 2.75 x 48 mm and another 2.5 X 38 mm was used. TIMI III flow was established and procedure was uneventful.
Case Summary
Here we present a case of chronic stable angina (CCS III), Whose angiogram revealed single vessel disease ( 99% lesion in Proximal portion & CTO from mid to distal RCA). This complex CTO case was managed successfully by ante-grade wire escalation technique with anchor balloon support & two DES were deployed to cover the lesion. Procedure was uneventful and the patient was discharged in stable condition.