
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-199
AI-Reconstructed Ultra-High-Resolution CCTA and Intravascular Lithotripsy-Assisted PCI for Severe Concentric and Eccentric Calcified Plaques
By Hirofumi Ohashi, Koshiro Sakai, Masanobu Fujimoto, Akihiro Suzuki, Hirohiko Ando, Carlos Collet, Tetsuya Amano
Presenter
Hirofumi Ohashi
Authors
Hirofumi Ohashi1, Koshiro Sakai2, Masanobu Fujimoto1, Akihiro Suzuki1, Hirohiko Ando1, Carlos Collet3, Tetsuya Amano1
Affiliation
Aichi Medical University, Japan1, Showa University, Japan2, OLV Hospital, Belgium3,
View Study Report
TCTAP C-199
Coronary - Imaging & Physiology - Non-Invasive Imaging (CTA, MRI, Echo, etc)
AI-Reconstructed Ultra-High-Resolution CCTA and Intravascular Lithotripsy-Assisted PCI for Severe Concentric and Eccentric Calcified Plaques
Hirofumi Ohashi1, Koshiro Sakai2, Masanobu Fujimoto1, Akihiro Suzuki1, Hirohiko Ando1, Carlos Collet3, Tetsuya Amano1
Aichi Medical University, Japan1, Showa University, Japan2, OLV Hospital, Belgium3,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
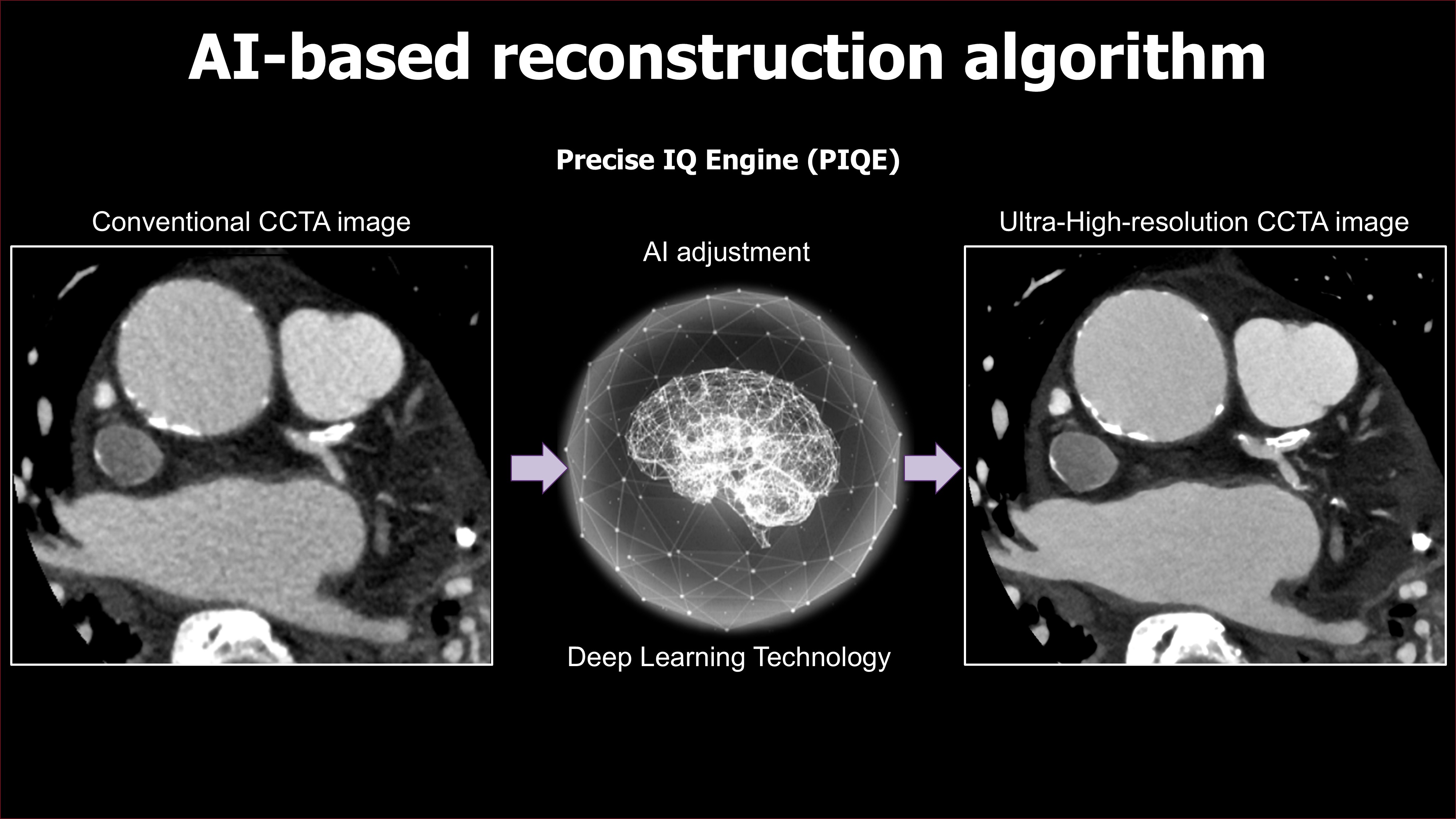
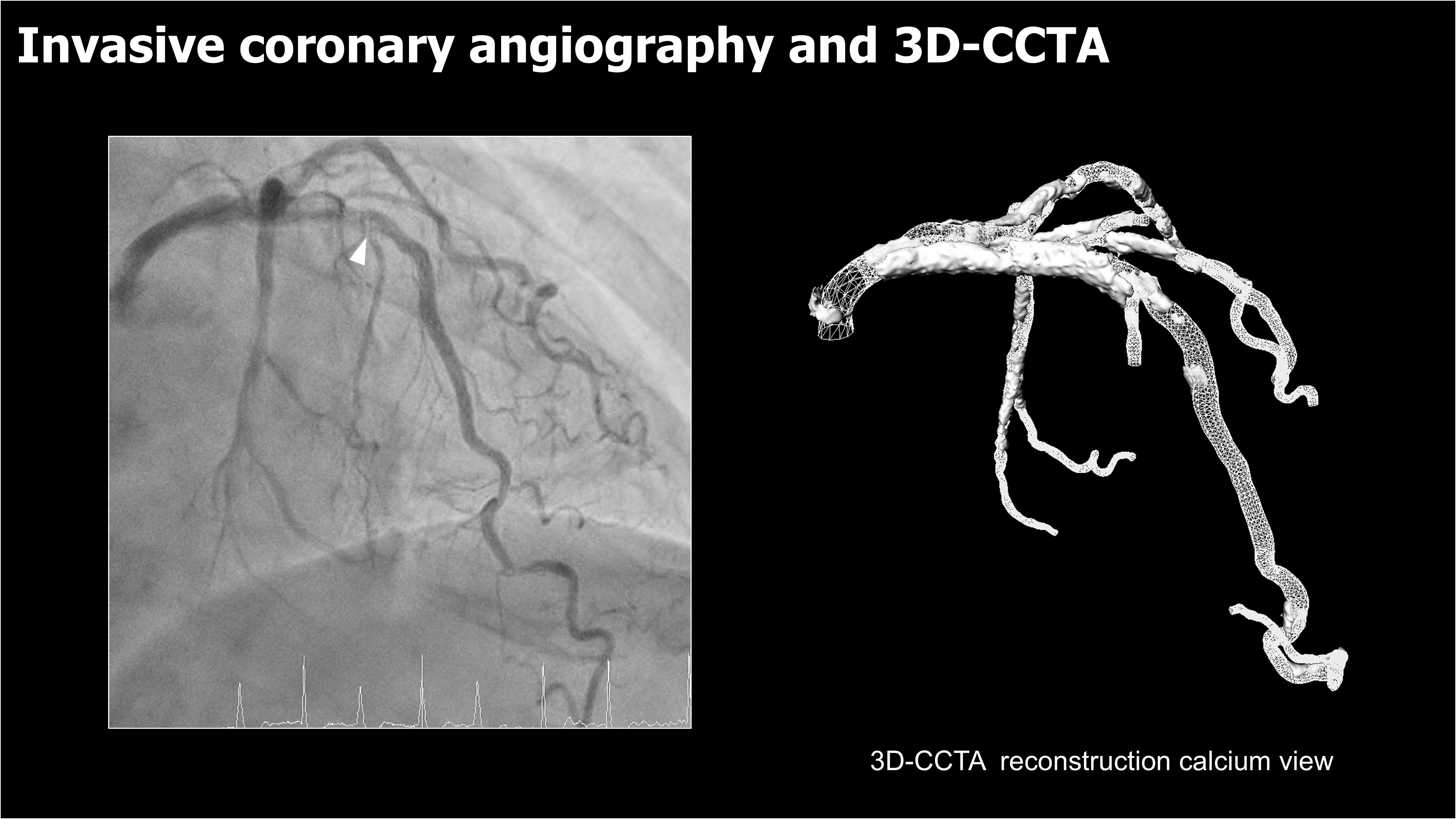
A 73-year-old female with severe aortic stenosis (AS), hypertension,and atrial fibrillation underwent a coronary CT angiography (CCTA) due to stable angina, which is CCS class II. Coronary CT angiography (CCTA) was performed using an AI-based reconstruction algorithm (Aquilion ONE®, CanonMedical Systems), providing ultra-high-resolution images.
Relevant Test Results Prior to Catheterization
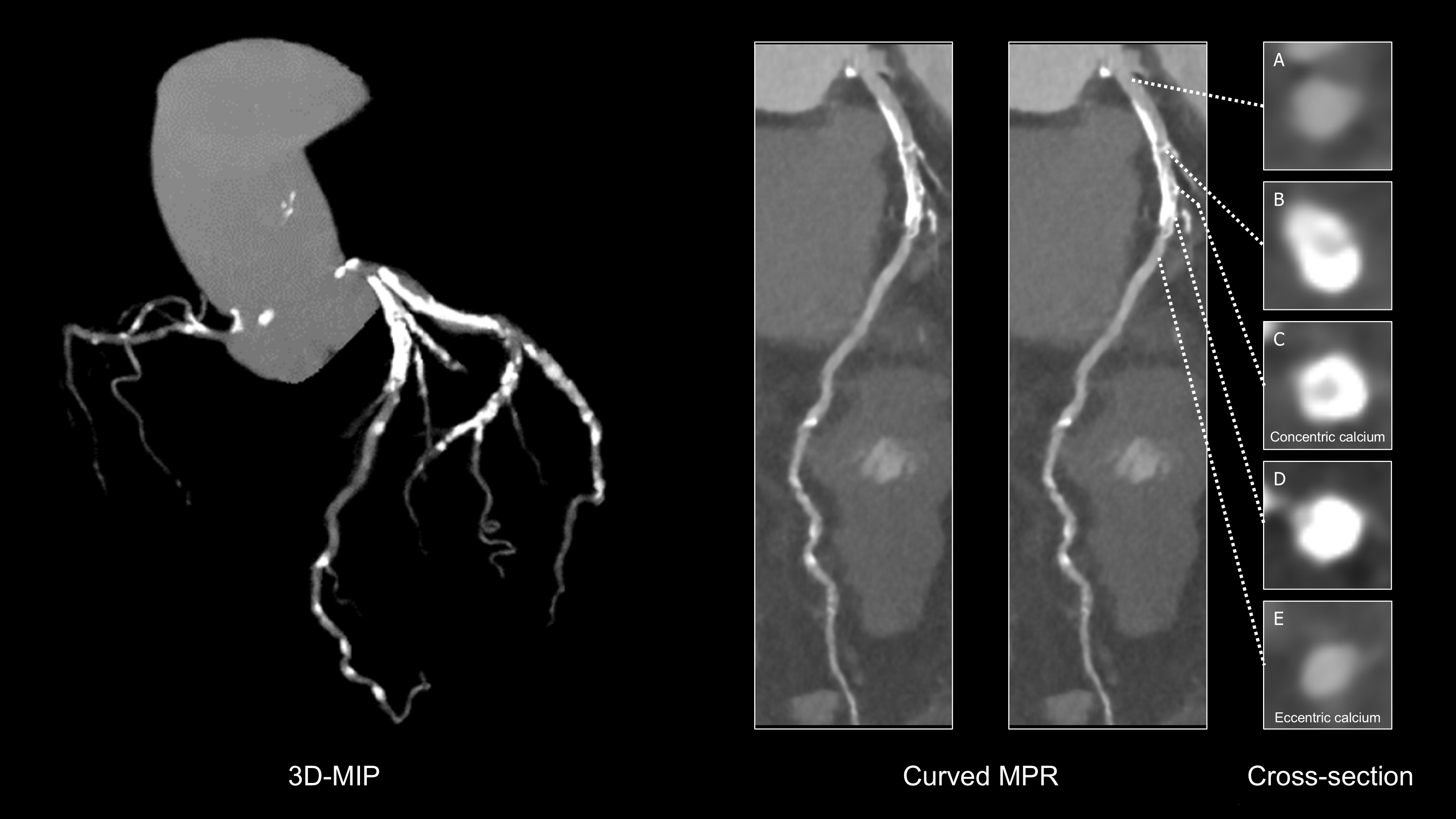
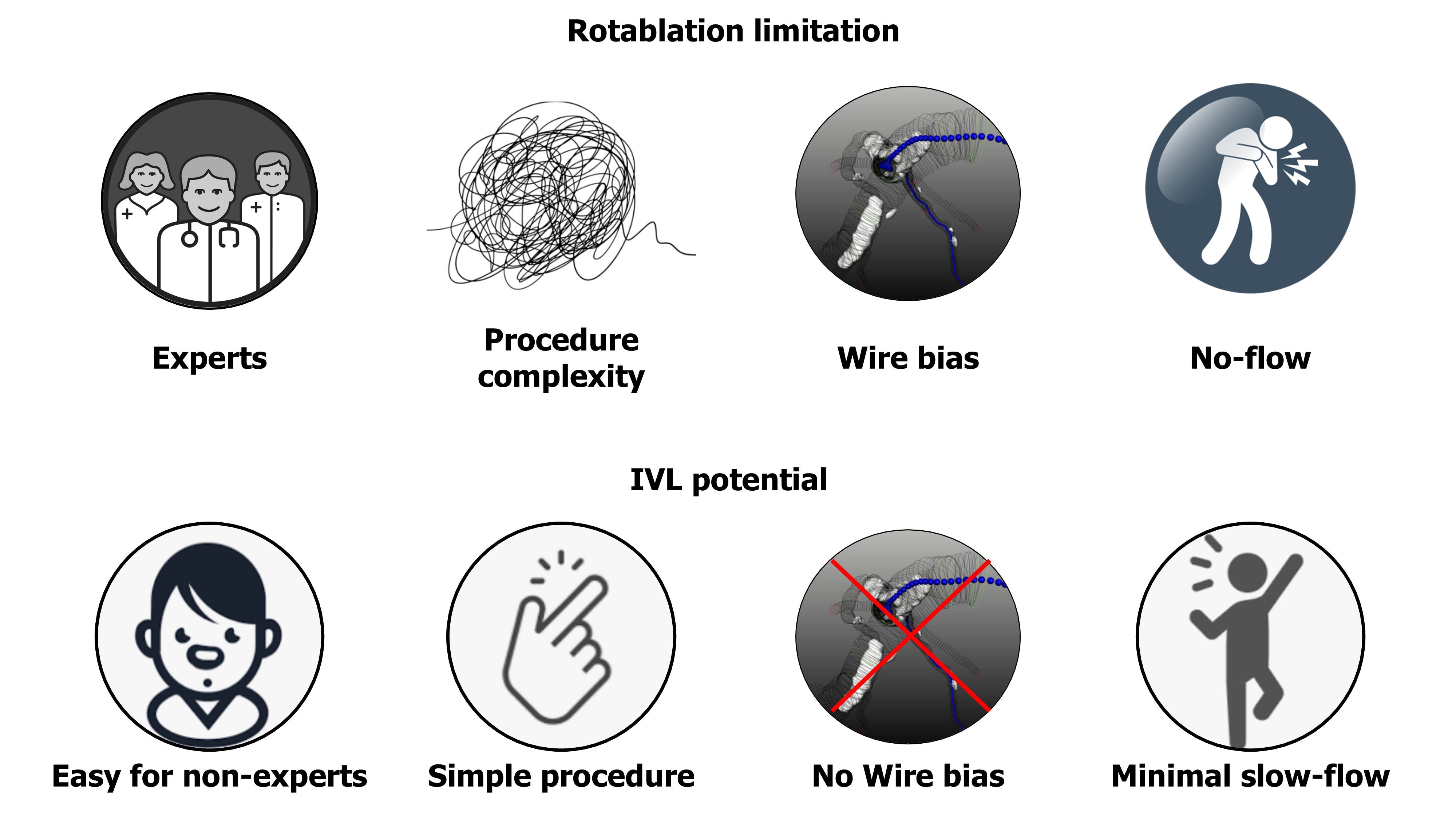
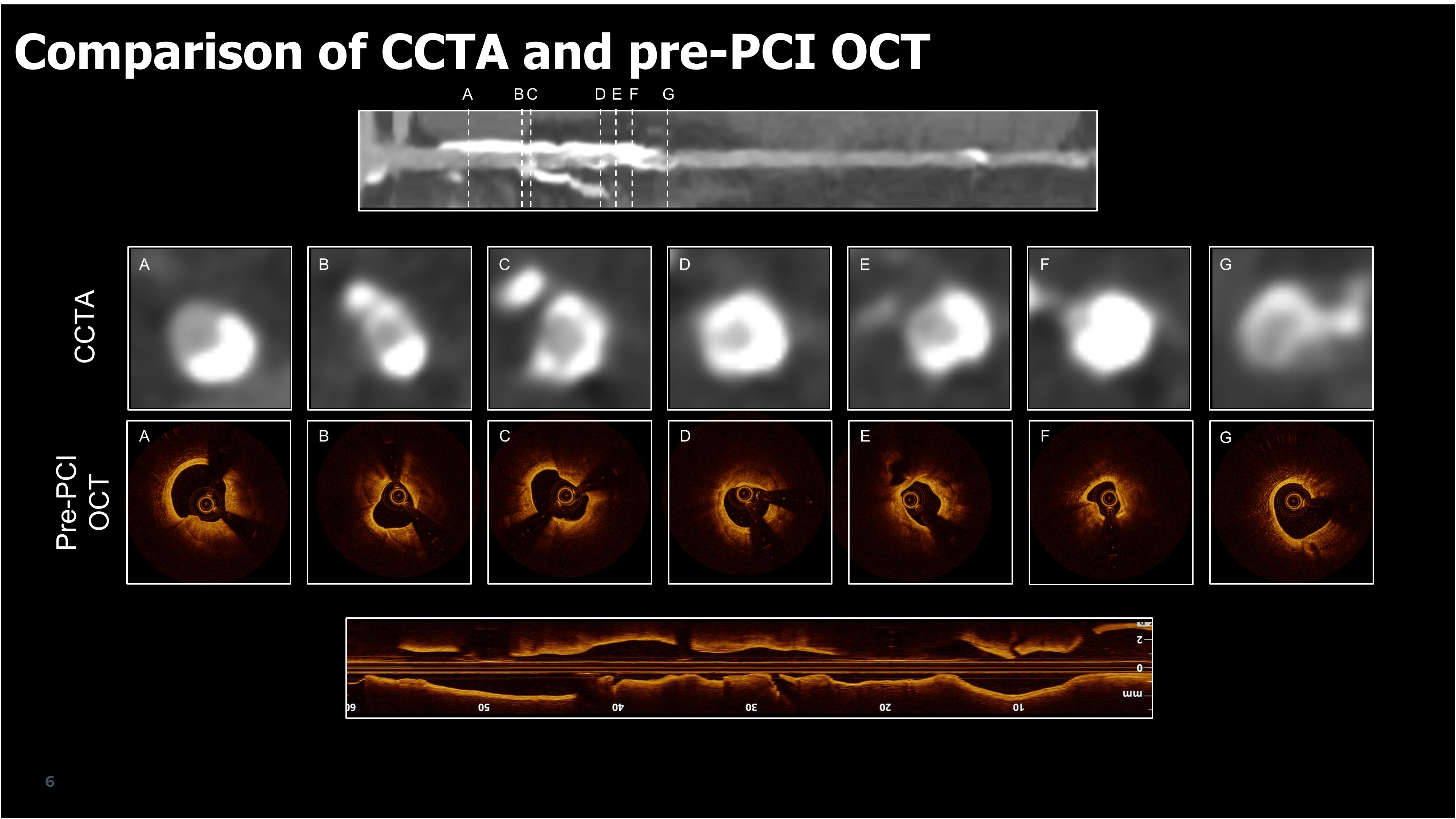
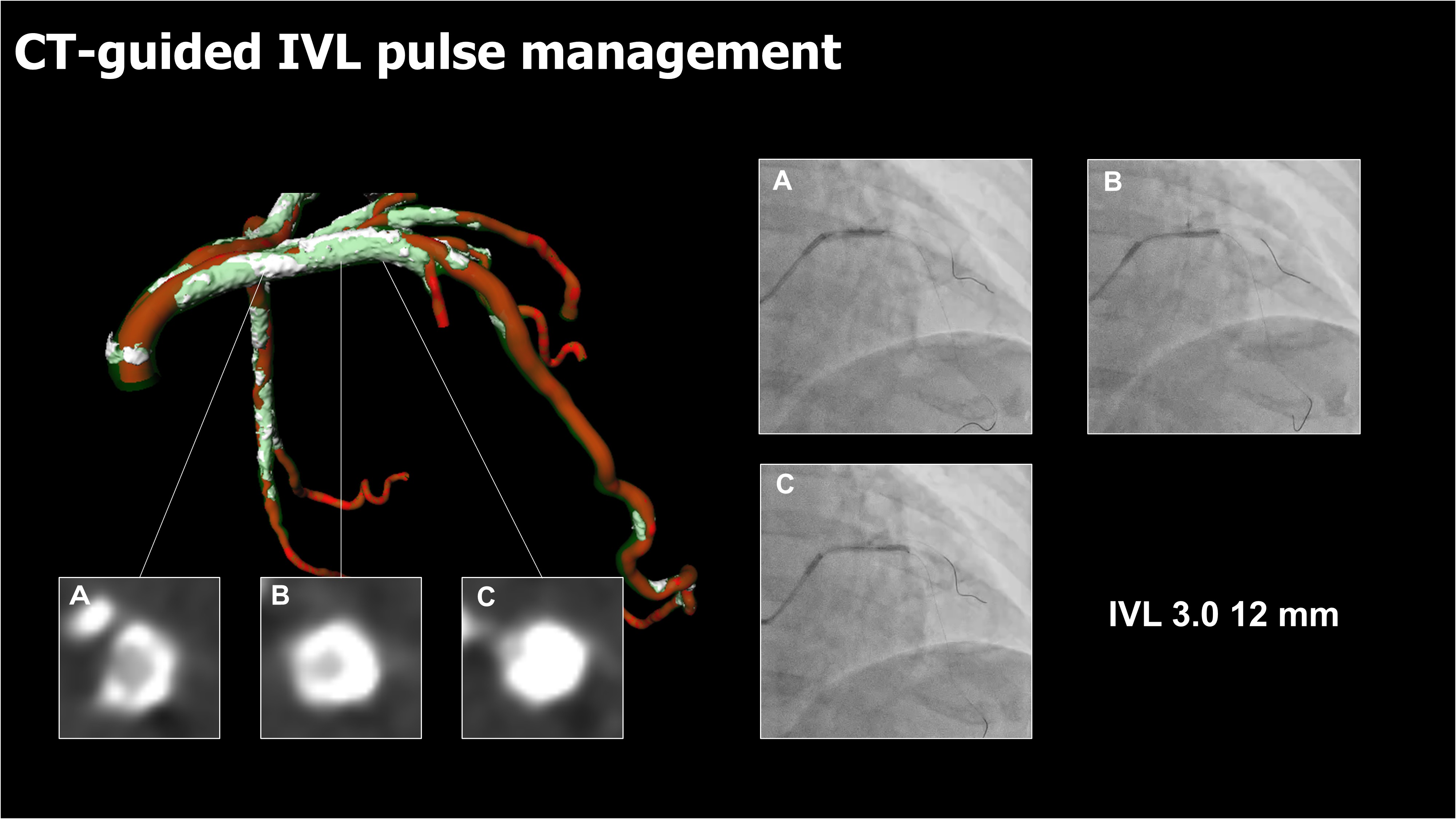
CCTA revealed two significantly different typesof calcifications with severe stenosis in the left anterior descending (LAD). Onehad concentric calcification in the mid-LAD, while the other exhibitedeccentric calcified plaque near the bifurcation with a diagonal branch (Dg). We planned to modify bothconcentric and eccentric calcium using IVL. The decision was considered to avoid the risk ofslow flow, particularly given the patient's severe AS.
Relevant Catheterization Findings
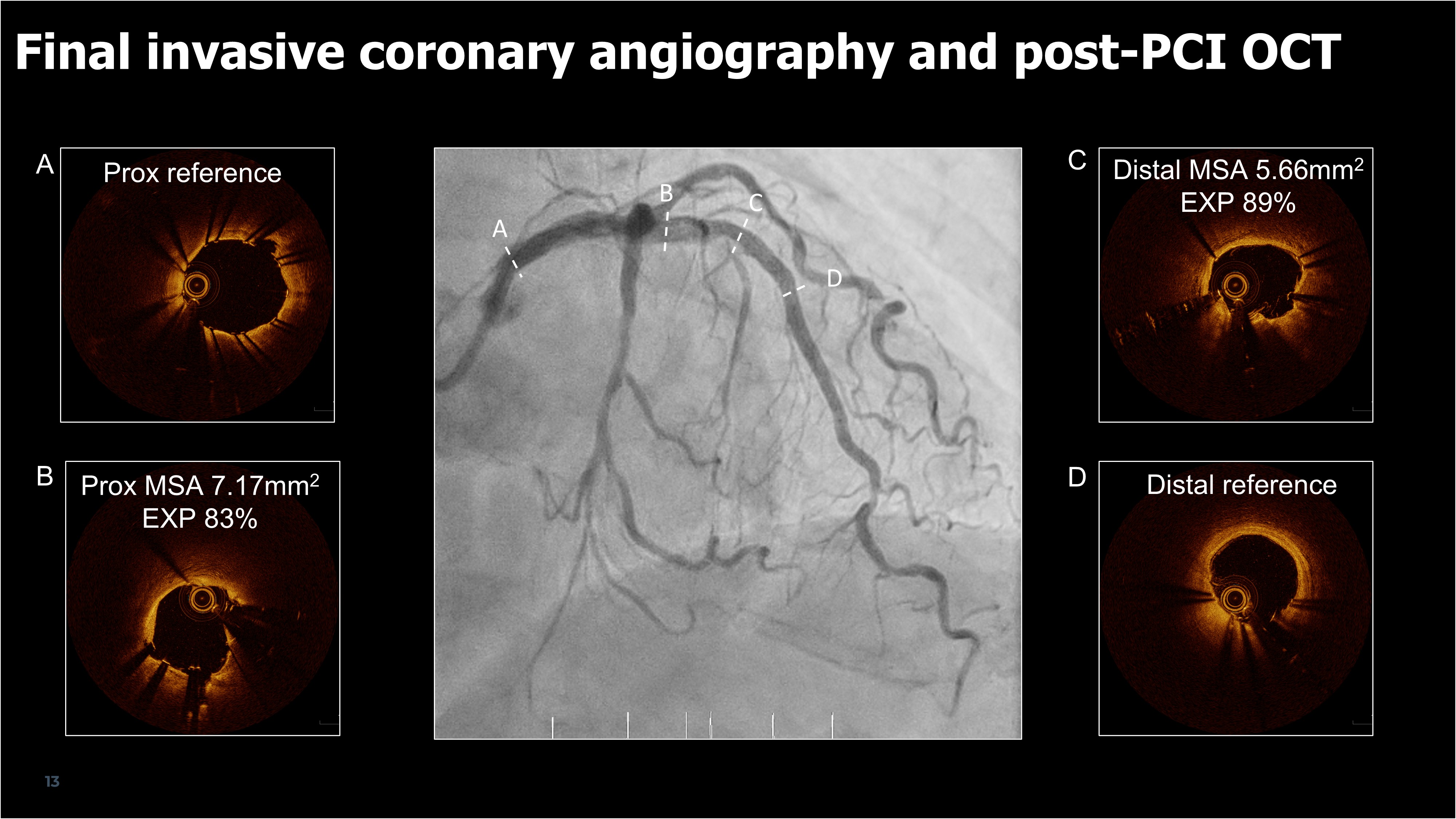
Invasive coronary angiography identifiedsignificant stenosis in the mid-LAD and at the LAD/Dg bifurcation, with afractional flow reserve (FFR) of 0.76. Optical coherence tomography (OCT)confirmed severe calcification like CCTA.
Interventional Management
Procedural Step
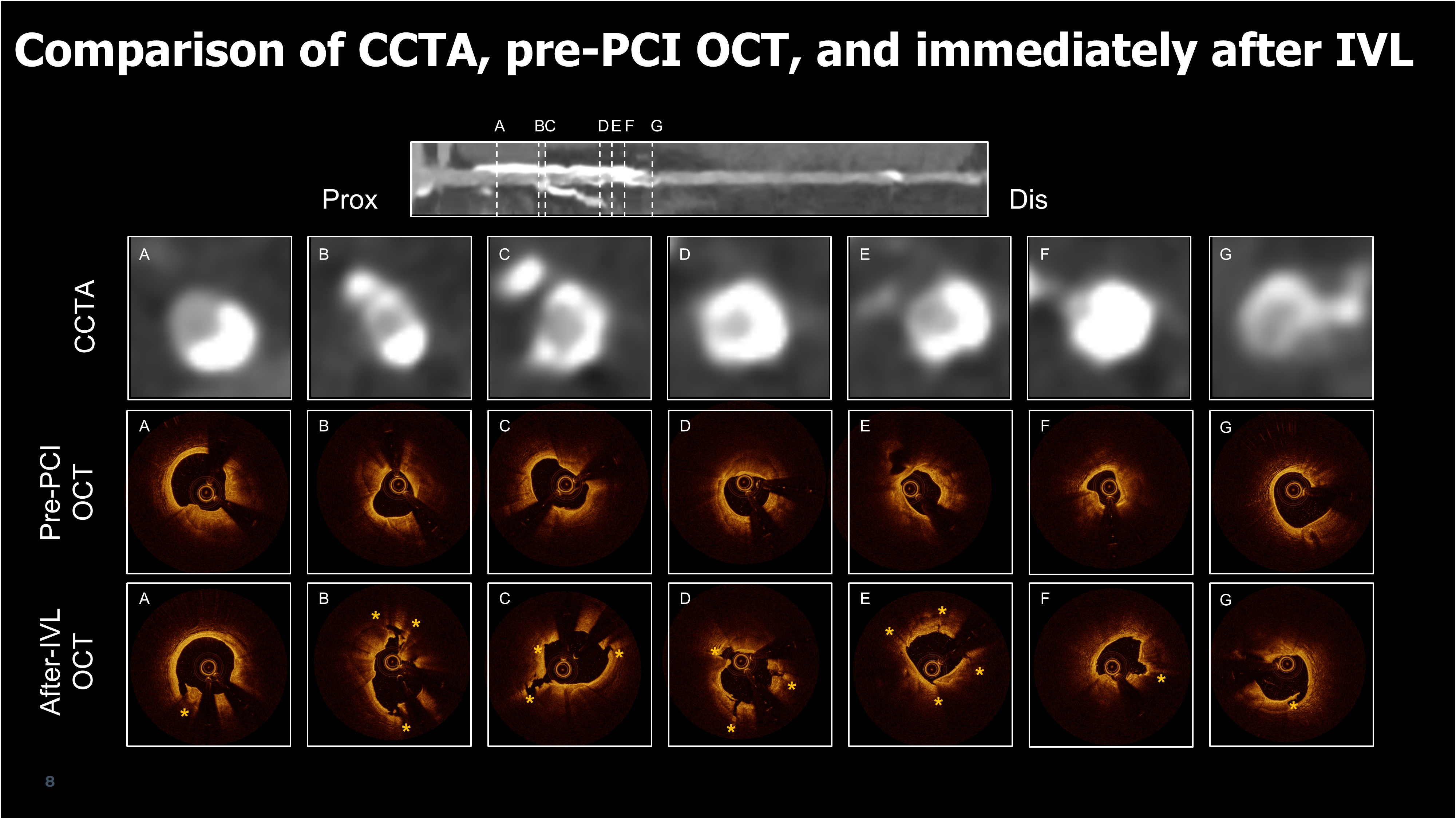
IVL was performed on both lesions, targeting the concentric and eccentric plaques. Post-IVL OCT revealed three fractures in the concentric plaque and one fracture in the eccentric plaque, leading to significant luminal gain. A drug-eluting stent (3.0x48mm) was deployed, followed by a 3.25 mm noncompliant balloon, with online CCTA guidance ensuring precise placement. Post-PCI OCT showed a minimum stent area of 7.2 mm² in the proximal concentric and 5.7 mm² in the distal eccentric calcified lesion.
Case Summary
This case demonstrates the utility of AI-enhanced ultra-high-resolution CCTA in identifying and guiding the treatment of complex calcified coronary lesions. IVL proved effective for both concentric and eccentric calcifications, resulting in favorable PCI outcomes.