
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-053
Unexpected Complication During Left Main Stenting: Double Barrel Sign
By Chin Wee Lee, Koay Koon Wee, Mohamed Jahangir, Ng Kai Choon, Sabapathy Diagarajan
Presenter
Chin Wee Lee
Authors
Chin Wee Lee1, Koay Koon Wee1, Mohamed Jahangir1, Ng Kai Choon1, Sabapathy Diagarajan1
Affiliation
Hospital Pulau Pinang, Malaysia1,
View Study Report
TCTAP C-053
Coronary - Complex PCI - Bifurcation
Unexpected Complication During Left Main Stenting: Double Barrel Sign
Chin Wee Lee1, Koay Koon Wee1, Mohamed Jahangir1, Ng Kai Choon1, Sabapathy Diagarajan1
Hospital Pulau Pinang, Malaysia1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
Mr I , a 81 years old gentleman with underlying Ischemic Heart Disease, diabetes mellitus, hypertension, dyslipidemia, gout and pangastritis . Patient complained of reduced effort tolerance and chest pain on exertion.
Relevant Test Results Prior to Catheterization
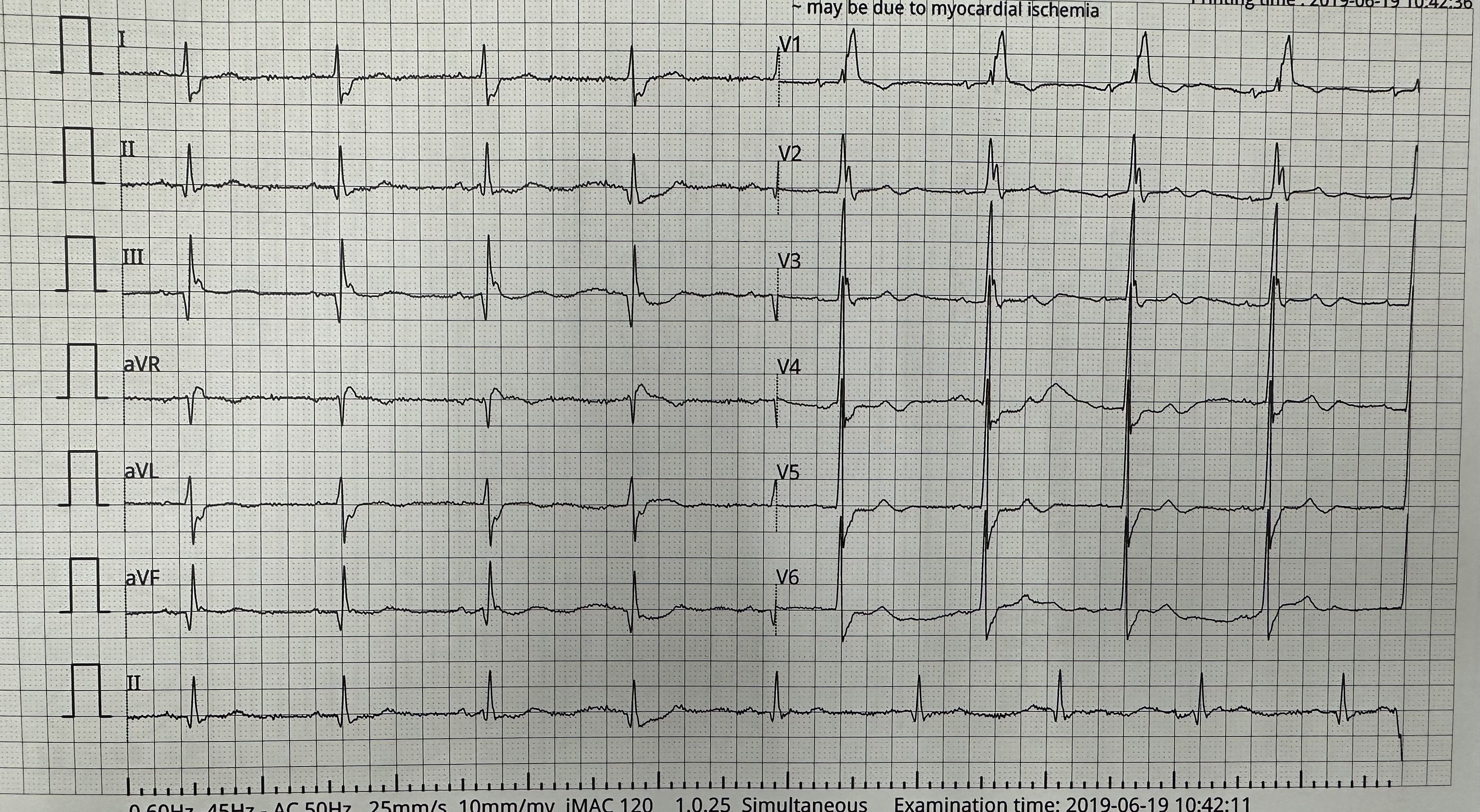
ECG showed sinus rhythm with right bundle branch block , Qwave over inferior lead ( lead 2,3 and AVF). Echocardiography showed left ventricular ejection fraction of 35%, global hypokinesia and dilated left ventricular and atrial chamber.
Relevant Catheterization Findings
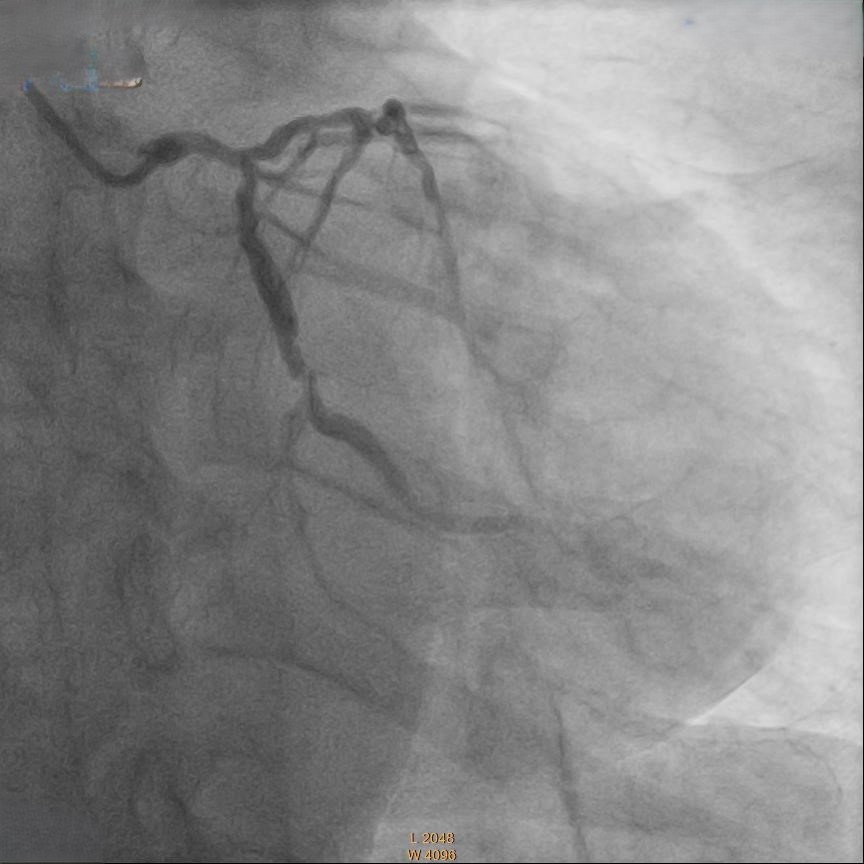
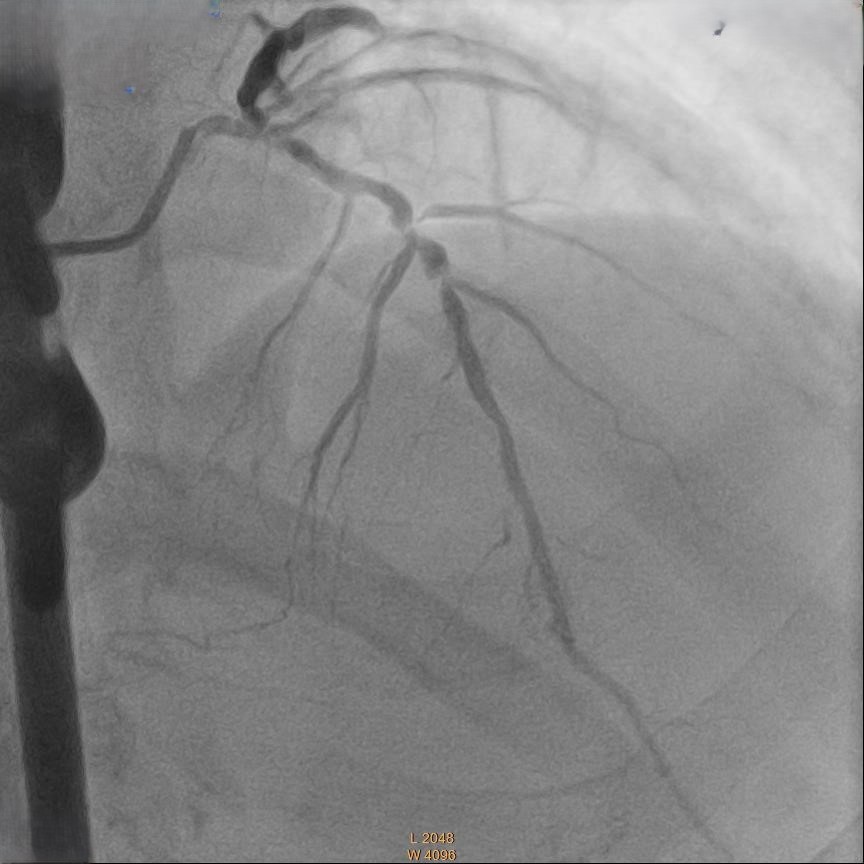
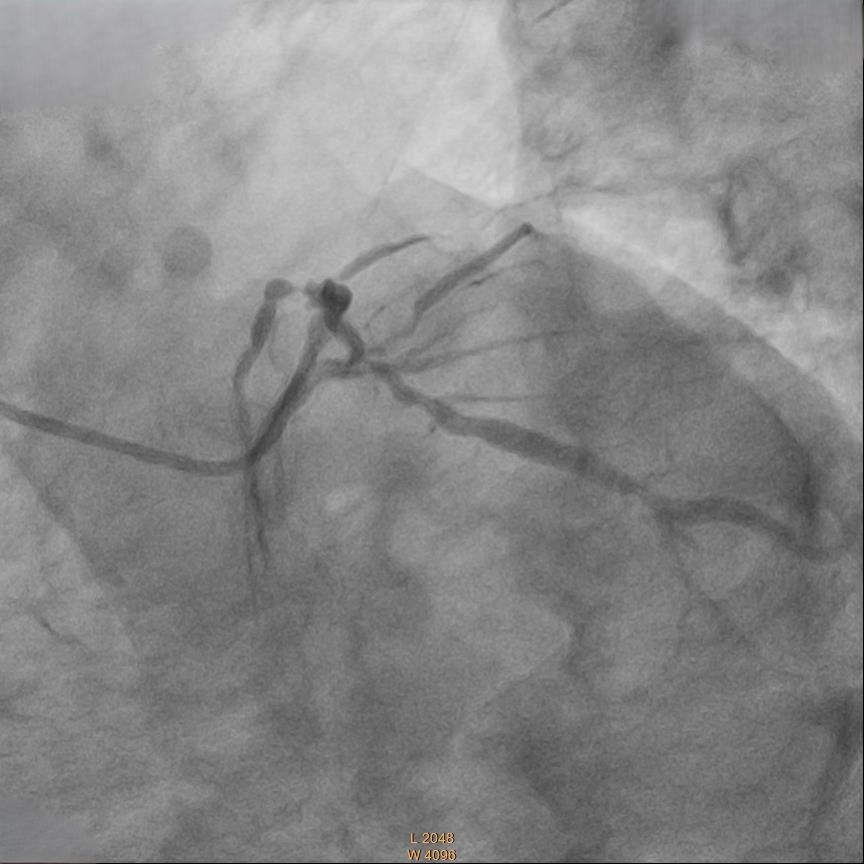
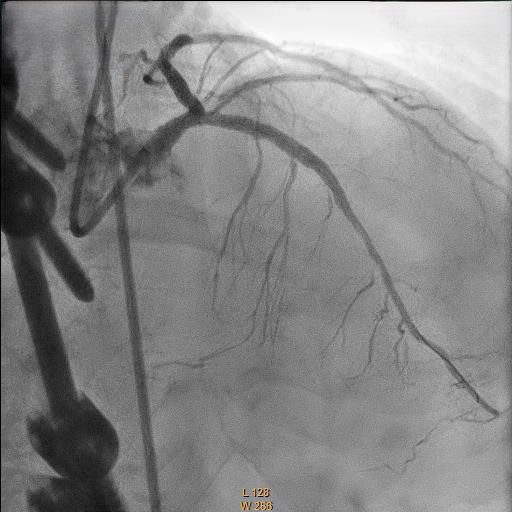
Coronary angiography showed 50% stenosis at Left Main (LM), proximal to mid Left Anterior Descending Artery (LAD) 70% stenosis, 80% stenosis at mid Left Circumflex Artery (LCX) and Chronic Total Occlusion at mid Right Coronary Artery (RCA) with collateral from LAD.
Interventional Management
Procedural Step
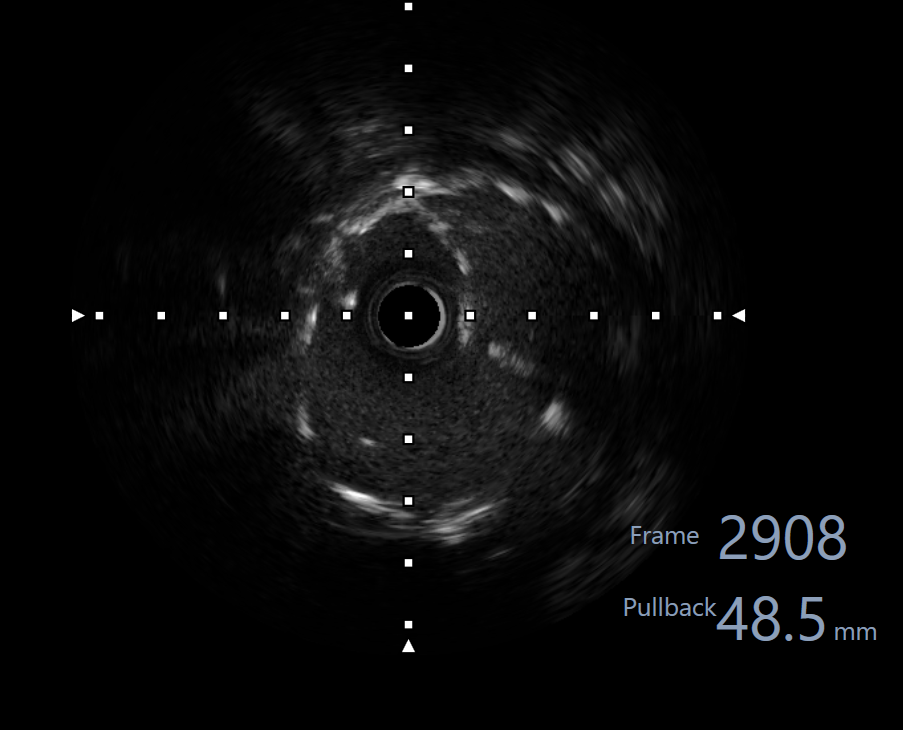
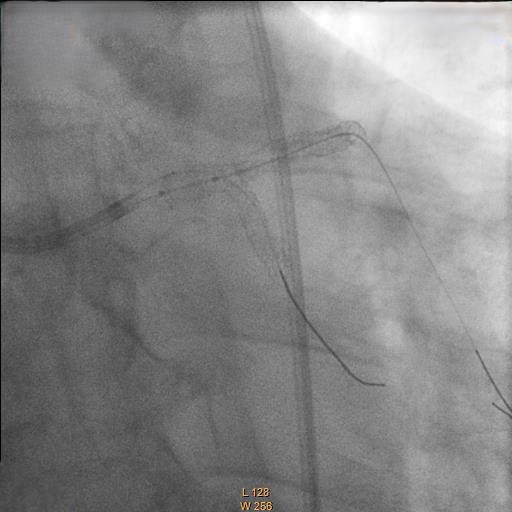
Right femoral artery punctured approach by 7Fr femoral sheath. Coronary guide catheter EBU 3.5 was used to engage left coronary artery. Percutaneous Coronary Intervention (PCI) to bifurcation Medina 1,1,1 using T and small protrusion (TAP) technique. LAD and LCX wired with workhorse wire . Mid LAD predilated with Semi-compliant (SC)2.5mm balloon and proximal LAD predilated with non-compliance (NC) 3.5mmballoon. Intravascular Ultrasound ( IVUS) was performed to measure the vessel size, lesion length and plaque morphology. Mid LAD stented with 3.5x23 mm drug eluting stent (DES). LM until proximal LAD stented with 4x33mm DES . Proximal optimization therapy (POT) at LM with NC balloon 5x8mm. Proximal LAD post dilated with NC balloon 4x20mm and mid LAD post dilated with NC balloon 3.5x15mm. LCX rewired with workhorse wire. Ostial LCX predilated with NC balloon 3.5x15mm and stented with 3.5x23mm DES subsequently post dilated with NC balloon 3.75x20mm. Final kissing balloon inflation was done at ostial LAD using NC balloon 4.0 and ostial LCX using NC balloon 3.75. Final IVUS noted double barrel sign at LM stent and confirmed with stent enhancement likely due to abluminal side branch wiring. Final POT to LM with NC balloon 5x8mm. Final IVUS showed good stent expansion and opposition with no dissection.
Case Summary
This case highlighted the importance of using IVUS in doing PCI. Importance of intravascular imaging in PCI was highlighted in recent 2024ESC guidelines and it’s class 1 evidence. Besides assessing the lesion length, diameter and plaque morphology, it can ensure good stent opposition and expansion. This is crucial to prevent complication during bifurcation stenting.