
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-063
Orbital Atherectomy in Short and Heavily Calcified Chronic Total Occlusion Right Coronary Artery
By Hana Soraya, Arwin Saleh Mangkuanom, Nanda Iryuza, Amir Aziz Alkatiri, Doni Firman
Presenter
Hana Soraya
Authors
Hana Soraya1, Arwin Saleh Mangkuanom1, Nanda Iryuza1, Amir Aziz Alkatiri1, Doni Firman1
Affiliation
National Cardiovascular Center, Indonesia1,
View Study Report
TCTAP C-063
Coronary - Complex PCI - Calcified Lesion
Orbital Atherectomy in Short and Heavily Calcified Chronic Total Occlusion Right Coronary Artery
Hana Soraya1, Arwin Saleh Mangkuanom1, Nanda Iryuza1, Amir Aziz Alkatiri1, Doni Firman1
National Cardiovascular Center, Indonesia1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A male, 82 years old came in with recurrent syncope induced by moderate exertion.He denied any chest pain or dyspnea. There was no dyspnea on effort. Physical examination findings were within normal limits.
Relevant Test Results Prior to Catheterization
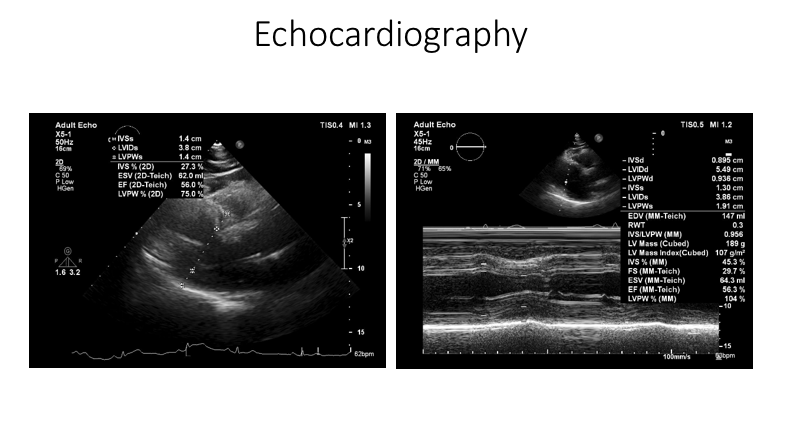
ECG result showed normal sinus rhythm, and echocardiography showed normal LVEF. CT Coronary Angiogram showed CAD 2VD with total occlusion of RCA and patent stent at the LAD.
Relevant Catheterization Findings
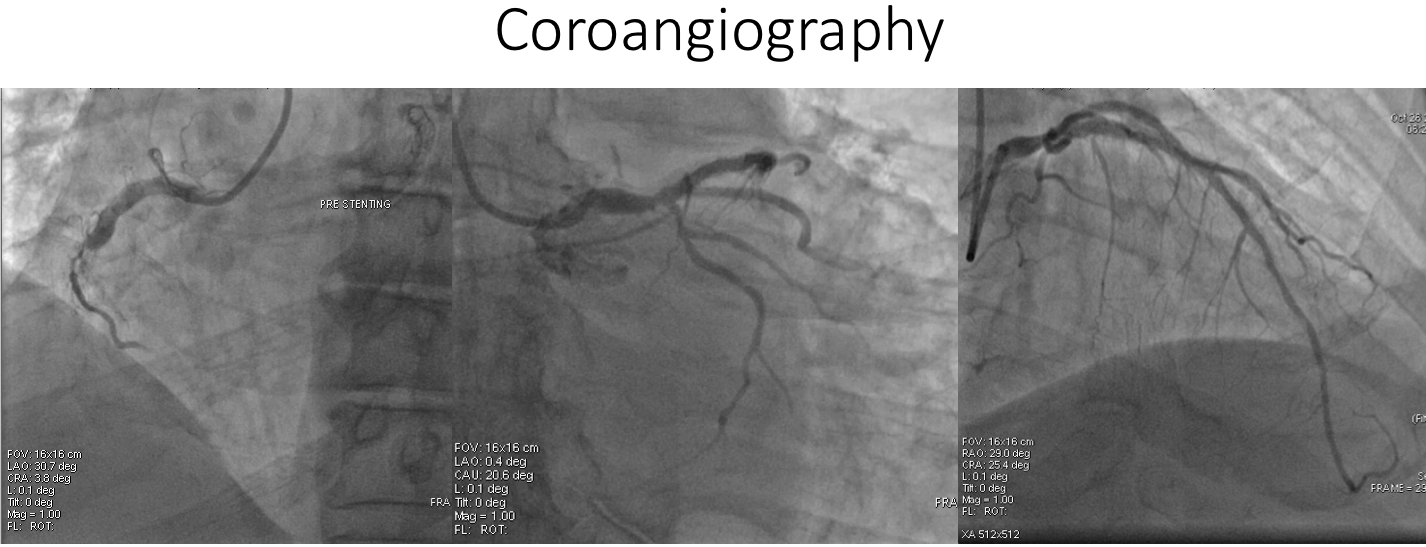
Subsequent angiography confirms the diagnosis. Heavy calcified with total occlusion at the mid part of the RCA. He was then readmitted for PCI to RCA.
Interventional Management
Procedural Step
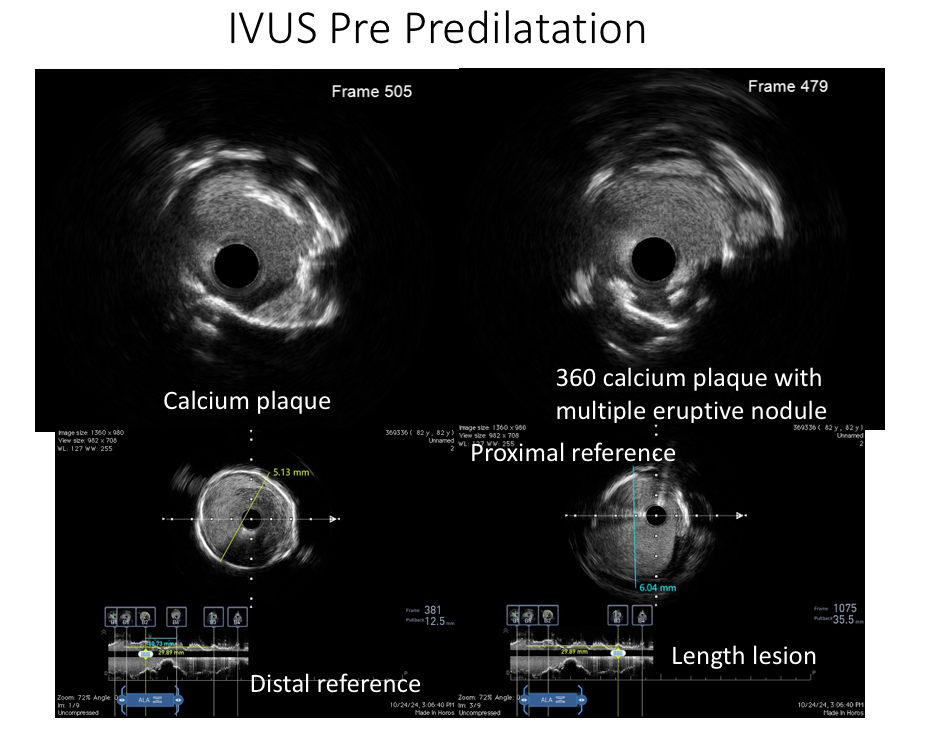
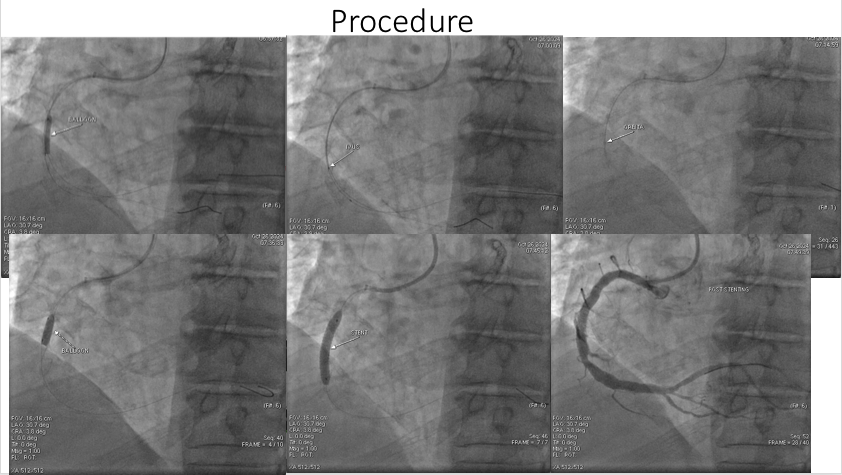
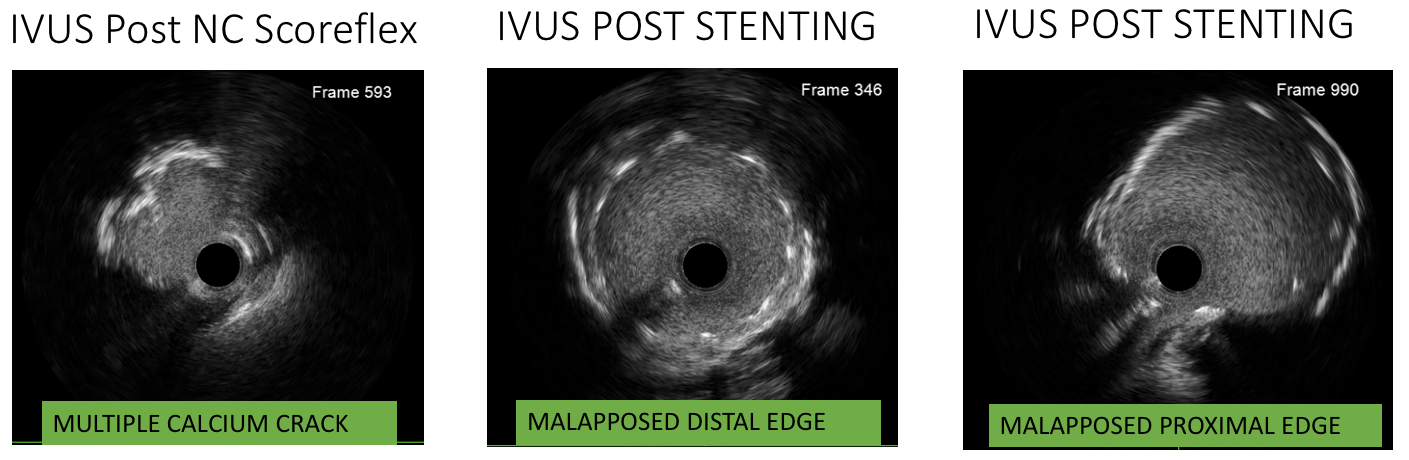
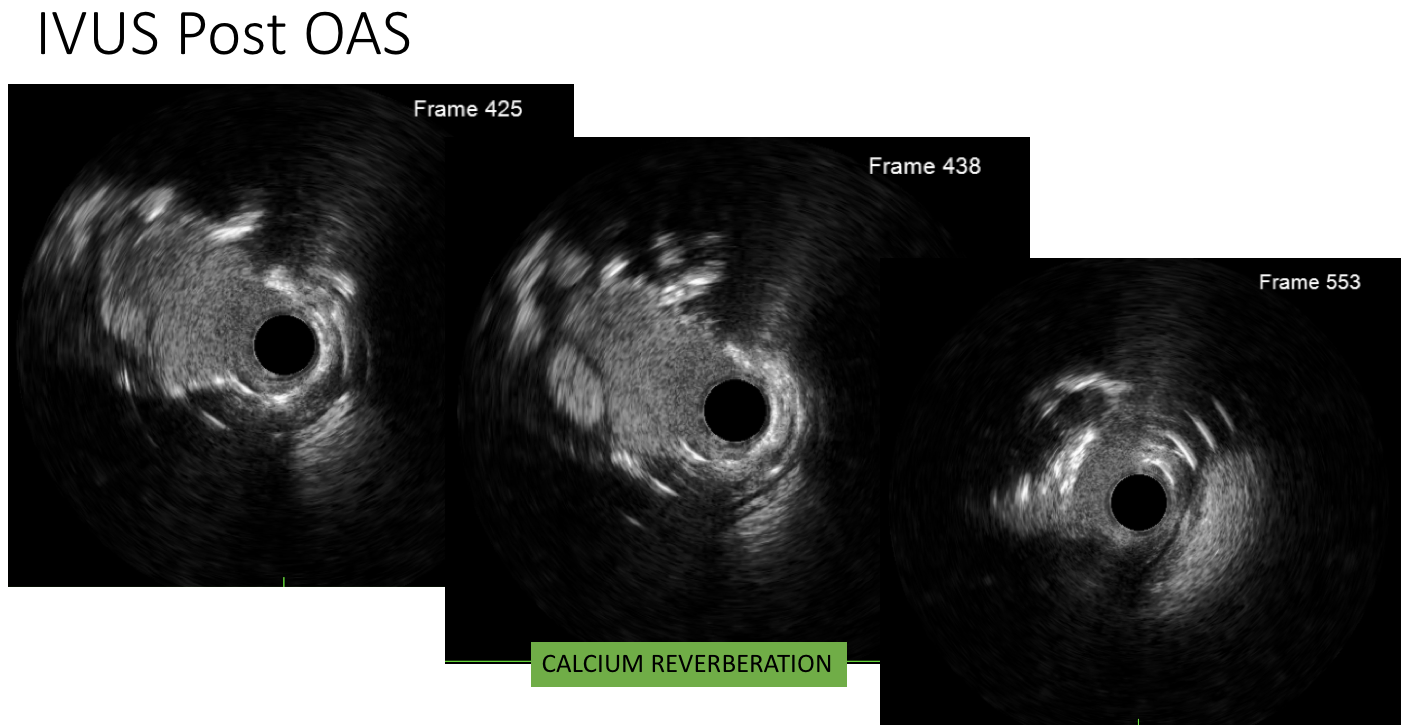
In this case,we opted for an atherectomy strategy for calcium modification.The procedure began via the radial artery using 6F sheaths and engaging the RCA with an IL 3.5 guiding catheter.Initially,the guiding catheter lacked sufficient support to cross the lesion. To address this,we introduced a Runthrough Floppy wire to the RV branch,along with a SC 2.0x15 mm balloon to facilitate microcatheter's penetration through the lesion.We then advanced the Asahi XTA wire through the lesion to the distal RCA and exchanged it for the Runthrough Floppy wire at the RV branch before transferring it to the posterior left (PL) branch.Multiple balloon predilations were performed using the SC 2.0x15 mm balloon, inflated to a maximum of 16 atm in the mid RCA,improving antegrade flow.We then escalated to a Scoreflex NC2.5x15 mm balloon,inflated to 18 atm in the mid RCA to crack the calcified plaque.IVUS was perfromed to analyze the lesion's characteristics, revealing circumferential calcium plaque with eruptive nodules. Calcium plaque seen at 2 to 4 o’clock was not favored by wire bias.Thus, we proceeded with an Orbital Atherectomy System using a Diamond Black 360 OAS for four runs at low speed followed by four runs at high speed.Postatherectomy IVUS evaluation showed reverberation. We prepared the lesion using Scoreflex. IVUS showed multiple calcium cracks. The RCA was stented using 3.0X24mm DES. Postdilation was done due to malapposition from IVUS. Final result was TIMI III Flow
Case Summary
Orbita atherectomy represents a significant advancement in the treatment of chronic total occlusion in PCI. Although the used of OA enhances the likelihood of stent deployment by modifying calcified plaque, it is still used sparingly due to its complexities and associated risks. In this case, OA has shown favourable results in preparing severely calcified lesion for stenting. Thus, when significant calcifications are present alongside multiple nodules and a tubular lesion with large vessels reference, orbital atherectomy emerges as the optimal solution.