
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-129
When Facing a Balloon Uncrossable Lesion and Rotablator Burr Entrapment in Left Anterior Descending Coronary Artery
By Thirawat Jewpakanon
Presenter
Thirawat Jewpakanon
Authors
Thirawat Jewpakanon1
Affiliation
Vachira Phuket Hospital, Thailand1,
View Study Report
TCTAP C-129
Coronary - Complication Management
When Facing a Balloon Uncrossable Lesion and Rotablator Burr Entrapment in Left Anterior Descending Coronary Artery
Thirawat Jewpakanon1
Vachira Phuket Hospital, Thailand1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A 65-year-old male presented with intermittent cardiac chest pain and dyspnea on exertion for past six months. He had a history of acute inferior wall STEMI and underwent primary percutaneous coronary intervention (PCI) with an everolimus-eluting stent placed in the proximal to mid right coronary artery (RCA) one year ago. He also had ischemic cardiomyopathy with triple vessel disease, hypertension, hyperlipidemia, and was on current guideline-directed medical therapy for ICM.
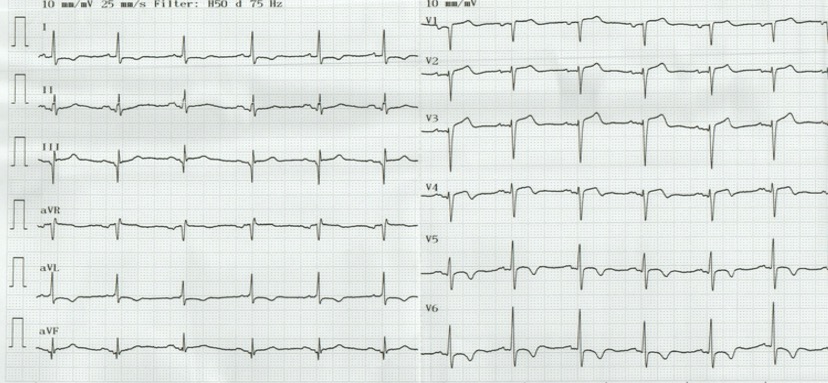
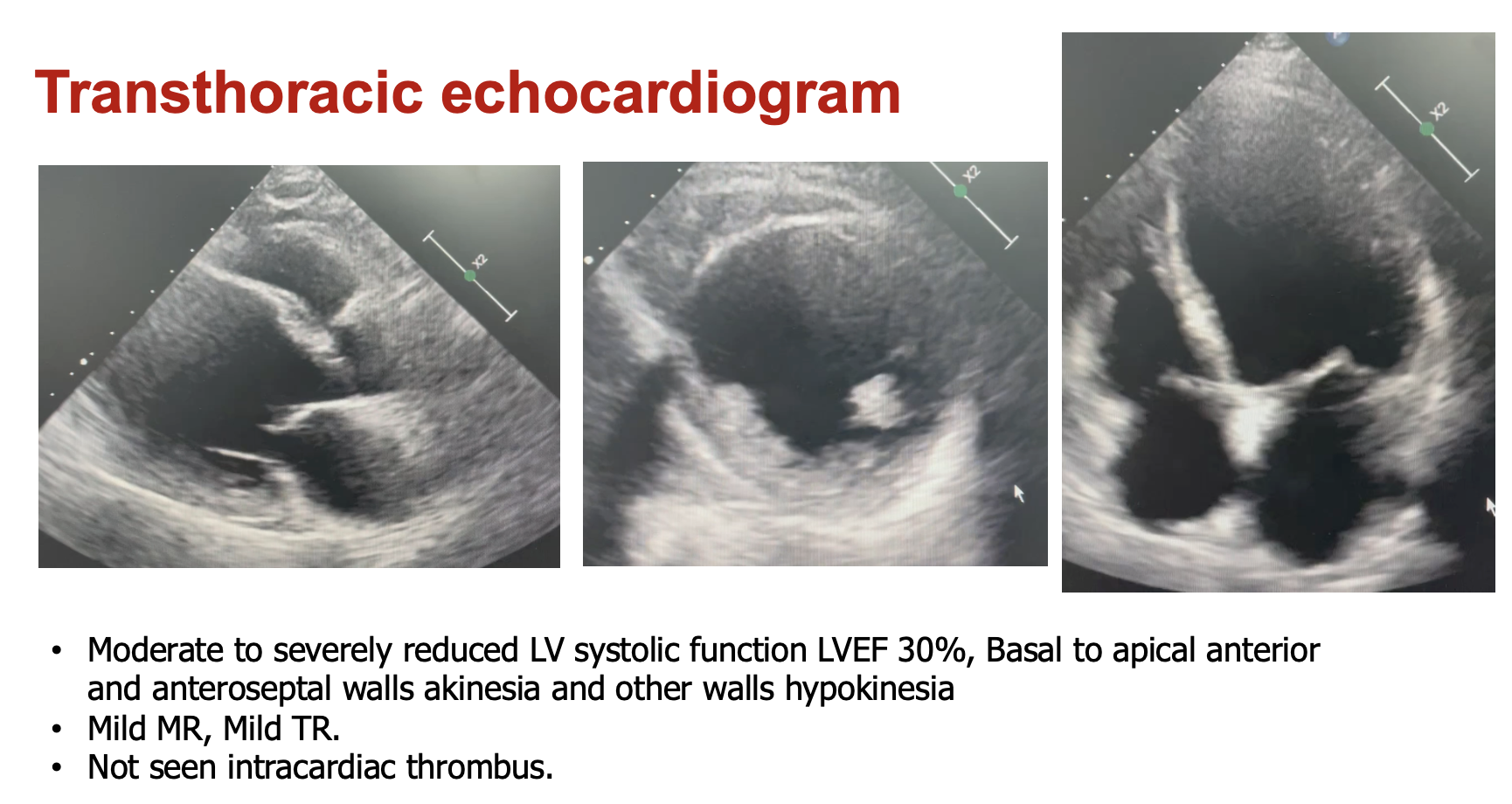
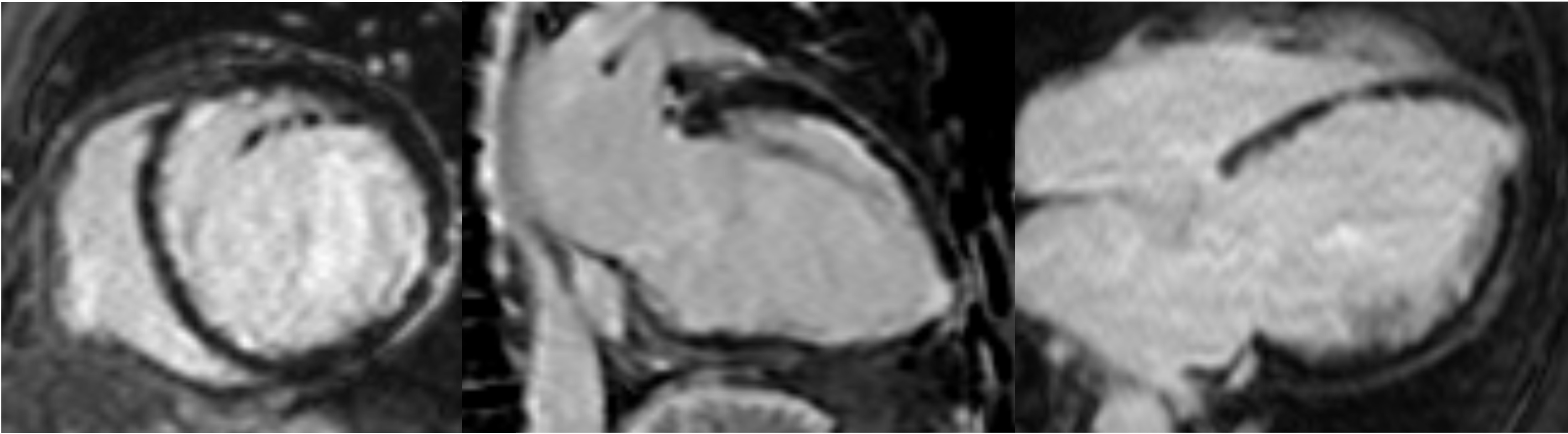
Relevant Test Results Prior to Catheterization
A 12-lead ECG showed normal sinus rhythm with poor R-wave progression and T-wave inversion in leads V4-V6. Echocardiography revealed severely reduced left ventricular systolic function with an ejection fraction of 30%, basal-to-apical anterior wall thinning, severe hypokinesia, and mild hypokinesia in other walls. Cardiac magnetic resonance imaging (CMR) demonstrated that all myocardial tissue was viable. Laboratory findings were within normal limits.
Relevant Catheterization Findings
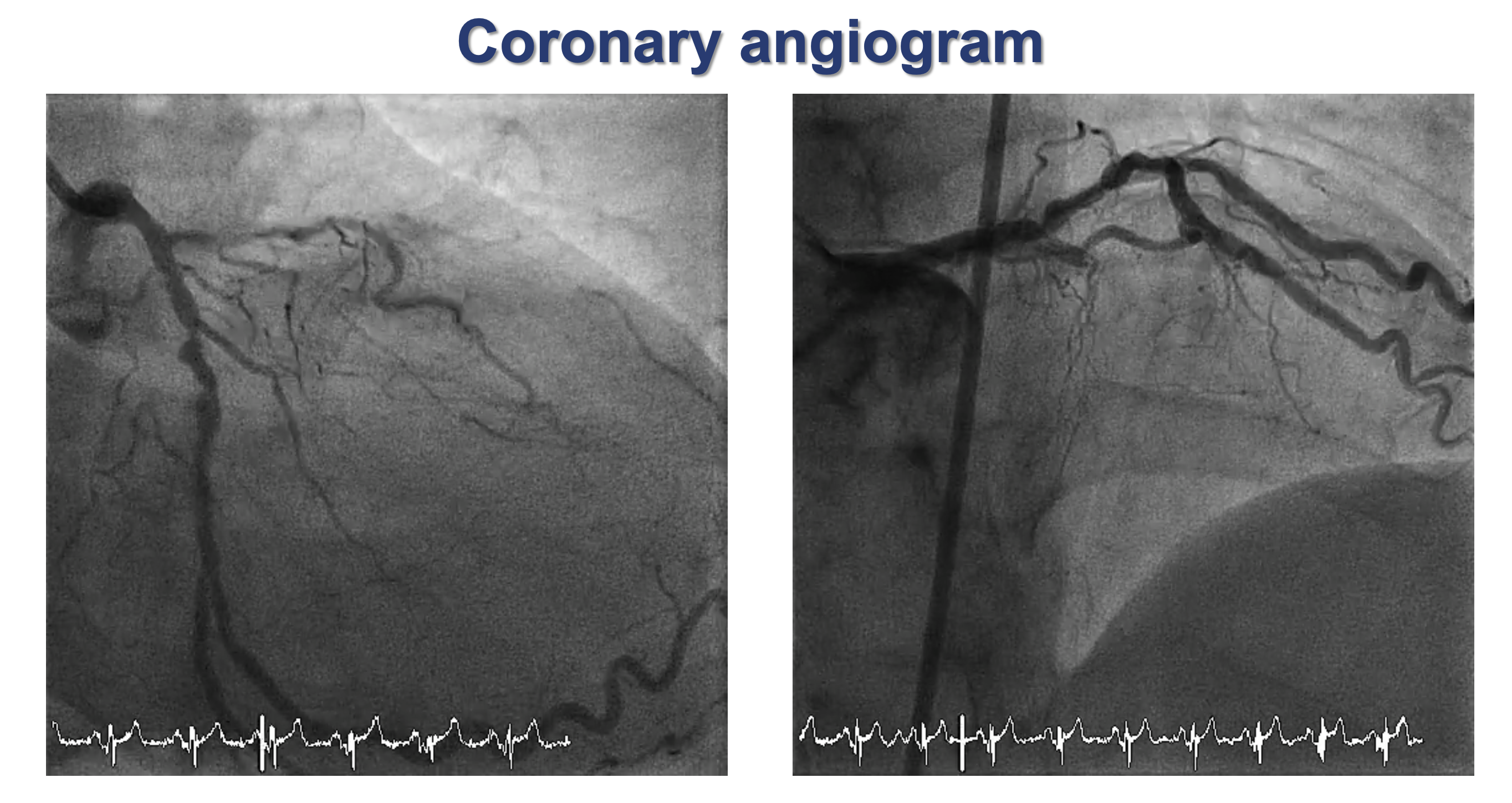
The coronary angiogram showed co-dominance and patent stent in the RCA, Chronic total occlusion (CTO) in the mid-left anterior descending coronary artery (LAD) and received collateral circulation from the left circumflex artery (LCx) and significant stenosis was noted in the proximal LCx. After a heart team conference, the patient absolutely refused coronary artery bypass grafting (CABG) and opted for complex PCI of the CTO in the mid-LAD as the mode of revascularization.
Interventional Management
Procedural Step
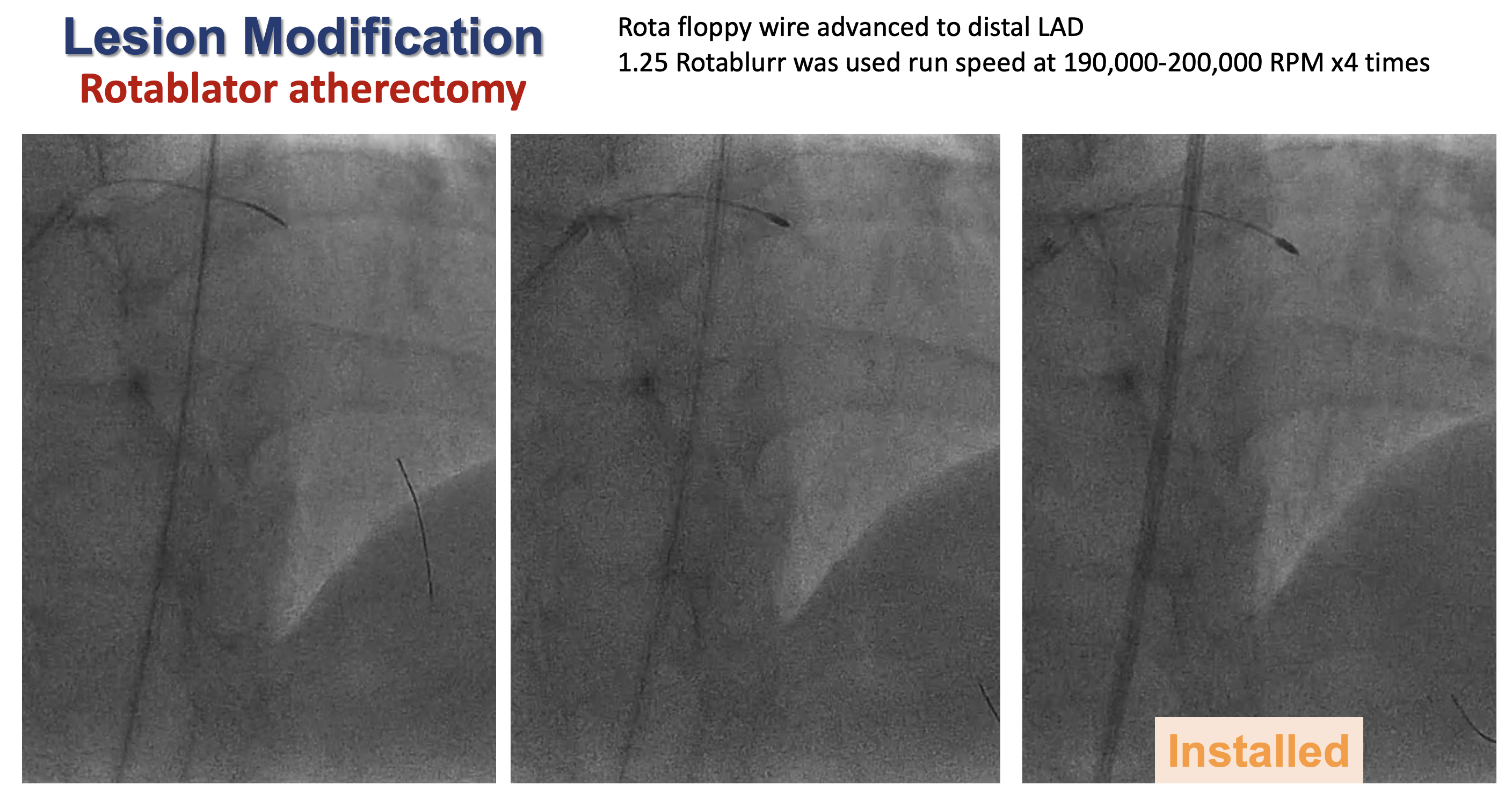
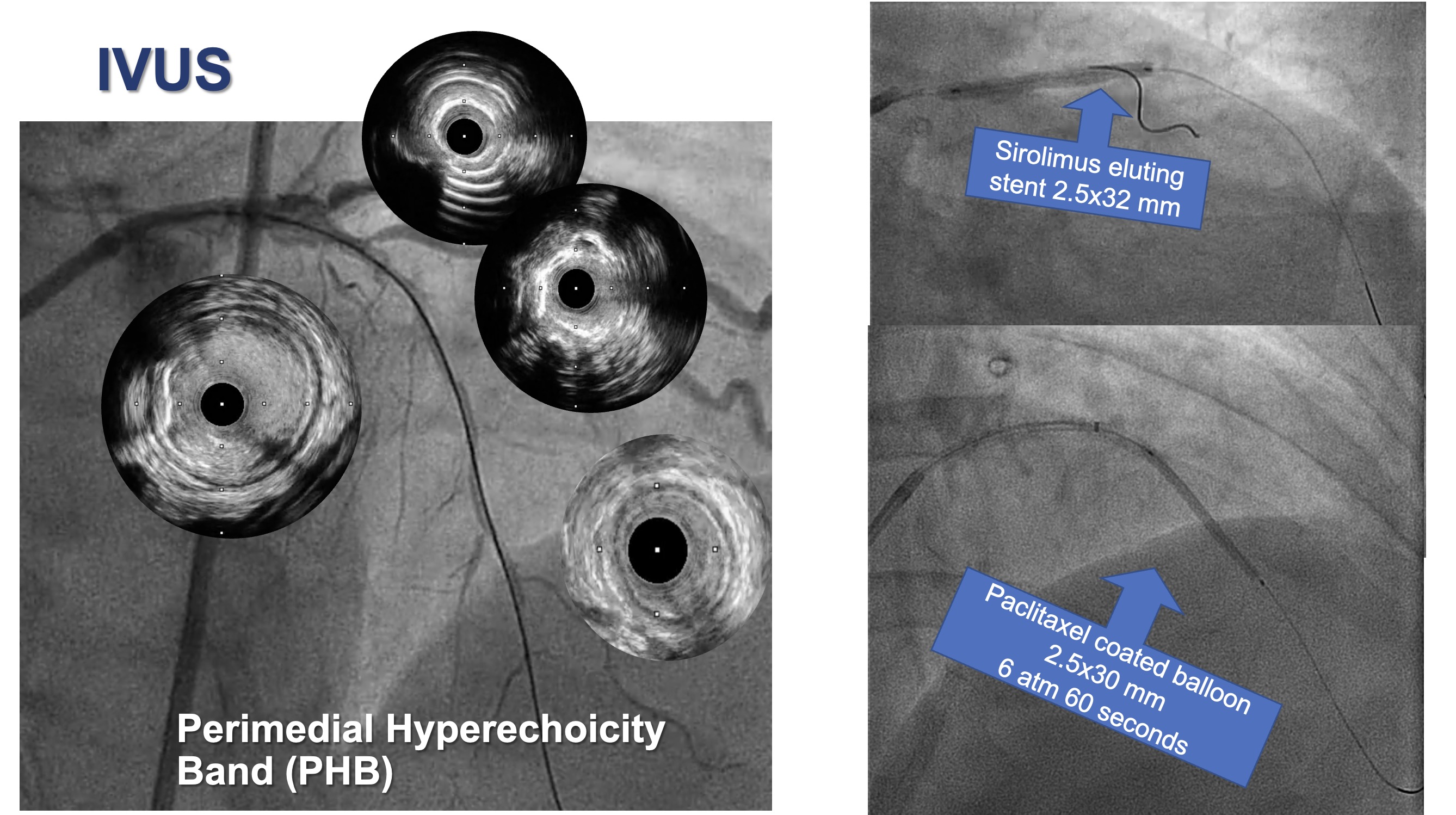
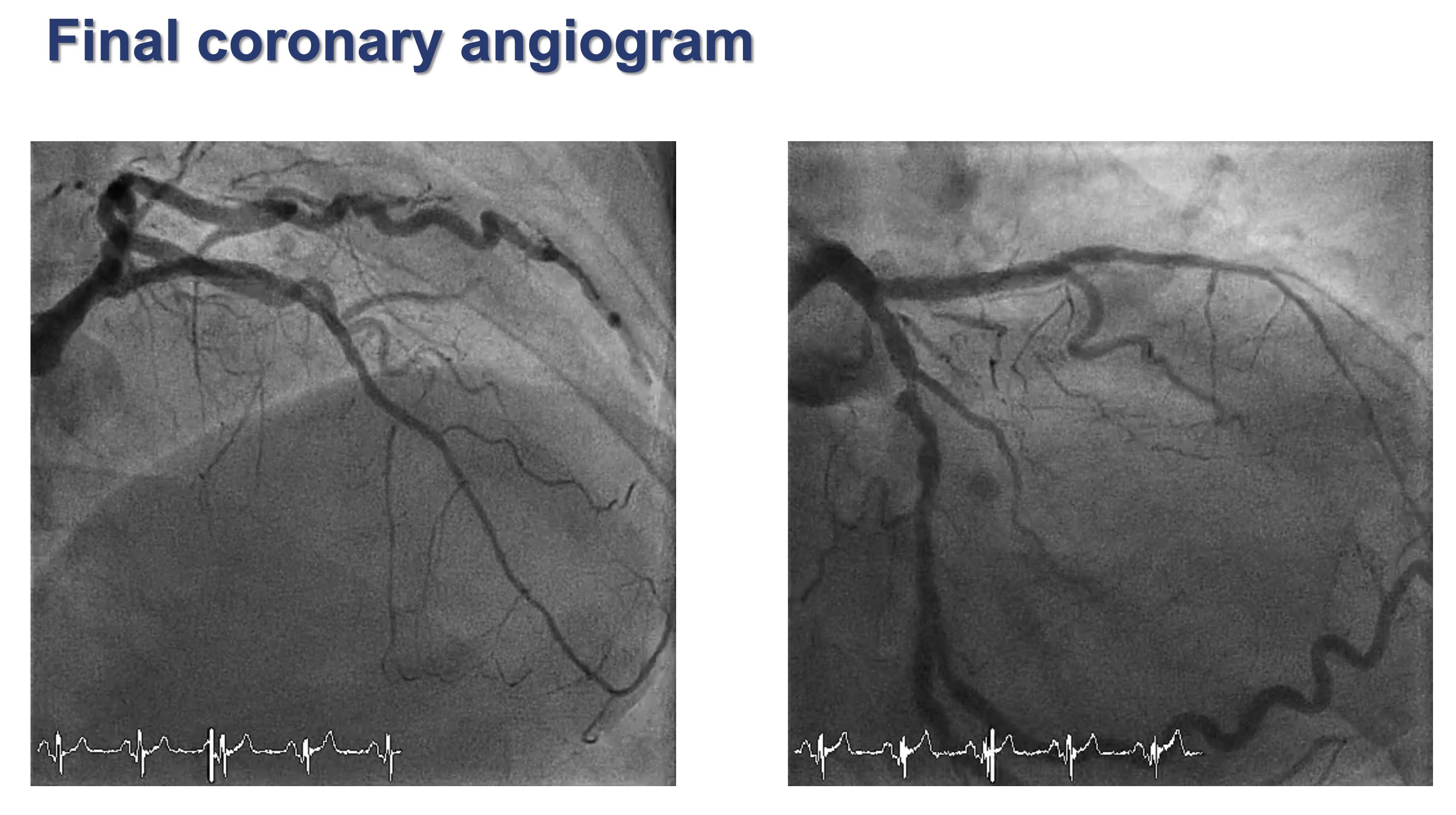
A 7-Fr system sheath with an EBU 3.5 guiding catheter was accessed via the right femoral artery without dual injection. The antegrade wire escalation technique with a microcatheter was used but initially failed with the Sion wire. The Fielder XT-A wire successfully crossed the CTO lesion, but the microcatheter and a small semi-compliant balloon could only advance to the proximal cap of the CTO lesion. Subsequently, Rotablator atherectomy was performed with bare the Rotawire Floppy advanced to the distal LAD. A Rotablator Burr 1.25 mm was used at a speed of 180,000–190,000 RPM for four passes. However, during the last pass, the Rotablator Burr became stuck at the mid-LAD lesion. Attempts to remove the Rotablator Burr by gently pulling back under Dynaglide mode failed. The Rotablator shaft and wire were then cut, and a guide extension catheter was inserted to provide additional support during the pullback. The entrapped Rotablator Burr was successfully removed. Post-removal angiography showed no high-grade dissection or vessel perforation. Intravascular ultrasound (IVUS) revealed fibrocalcific plaque along the LAD, with a reverberation artifact at the mid-LAD. Distal to the previous CTO showed a perimedial hyperechogenicity band (PHB). PCI was successfully performed with an Everolimus-eluting stent placed from the proximal to mid-LAD, and a paclitaxel-coated balloon was used distal to the stent due to the presence of PHB at the mid-LAD.
Case Summary
When complex PCI is performed with readiness to manage complications and apply appropriate interventions promptly. Although Rotablator burr entrapment is infrequent and often preventable, it can cause myocardial infarction. Aggressive pullback may lead to severe dissection or vessel perforation. Various techniques can be manage burr entrapment, including using a parallel second wire or balloon to release the stuck burr, cutting the Rotablator shaft and inserting a guide extension, or retrieving with a microsnare. Ultimately, prevention is better than cure. It is recommended gentle burr advancement without forceful contact and rotablation should neither start nor stop within target lesion.