
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-079
The Integral Role of IVUS in Complex PCI Optimization Using Dual Angiography and Modified Parallel Wire Technique
By Yulianto Yulianto, Arwin Saleh Mangkuanom, Doni Firman, Nanda Iryuza, Amir Aziz Alkatiri
Presenter
Yulianto Yulianto
Authors
Yulianto Yulianto1, Arwin Saleh Mangkuanom1, Doni Firman1, Nanda Iryuza1, Amir Aziz Alkatiri1
Affiliation
National Cardiovascular Center, Indonesia1,
View Study Report
TCTAP C-079
Coronary - Complex PCI - CTO
The Integral Role of IVUS in Complex PCI Optimization Using Dual Angiography and Modified Parallel Wire Technique
Yulianto Yulianto1, Arwin Saleh Mangkuanom1, Doni Firman1, Nanda Iryuza1, Amir Aziz Alkatiri1
National Cardiovascular Center, Indonesia1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A 56-year-old male presents with chest pain as the main complaint. He has a previous history of hypertension.He was referred to Harapan Kita Hospital due to the failure of a CTO PCI procedure at the previous hospital. The patient is currently on the following medications: minoxidil 80 mg once daily, clopidogrel 75 mg once daily, simvastatin 20 mg once daily, bisoprolol 5 mg once daily, candesartan 16 mg once daily, and isosorbide dinitrate (ISDN) 5 mg as needed for chest pain.

Relevant Test Results Prior to Catheterization
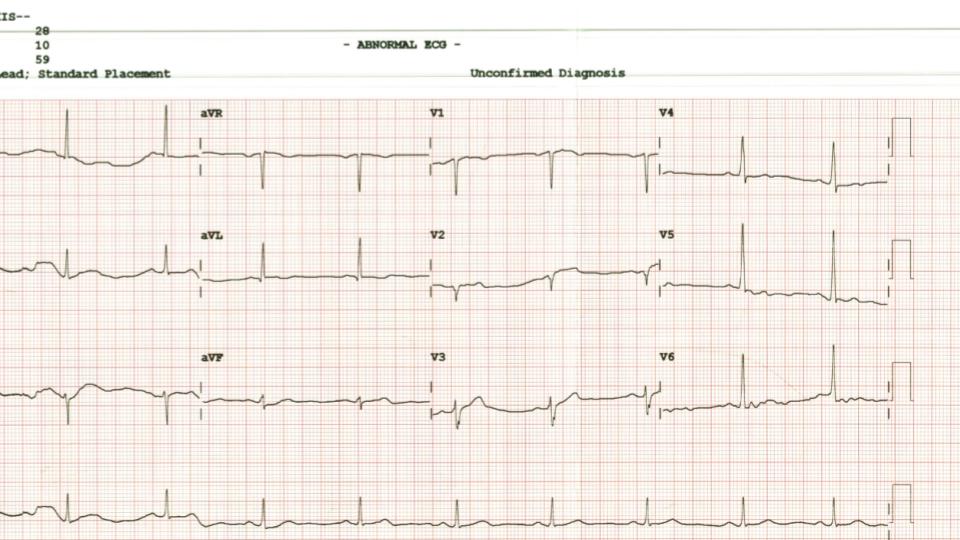
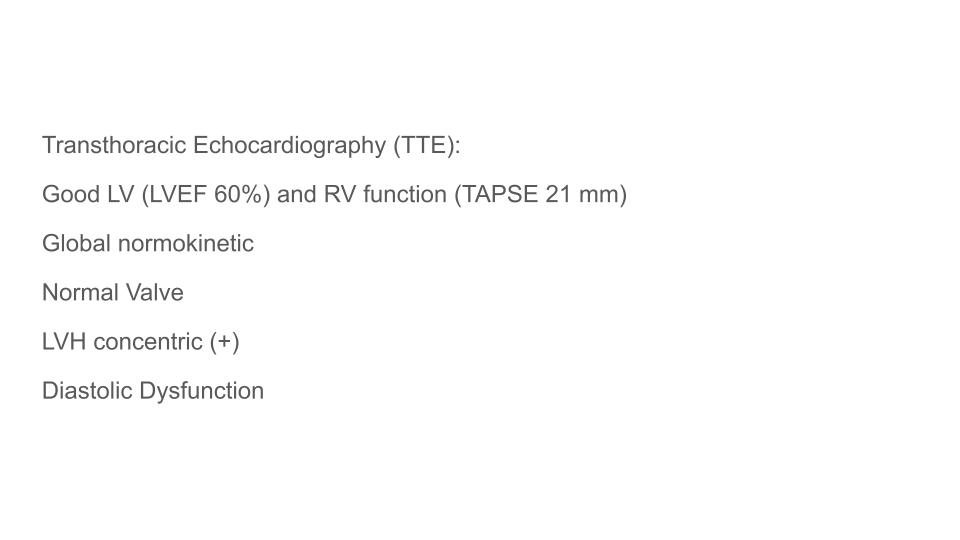
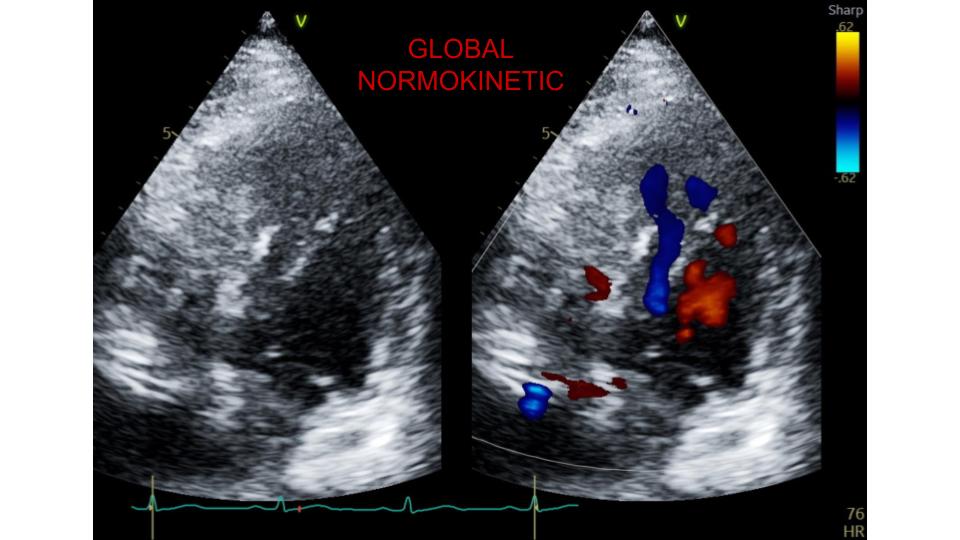
Laboratory results for the patient indicate a hemoglobin level of 12.1 mg/dL, creatinine level of 1.44 mg/dL, estimated glomerular filtration rate (eGFR) of 55 mL/min, blood glucose level of 90 mg/dL, and potassium level of 4.2 mEq/L. A treadmill test showed a positive ischemic response. TTE showed good LV and RV function, Normal Valve. The patient is diagnosed with stable angina pectoris (SAP) CCS class III, CAD with two-vessel involvement, and chronic total occlusion (CTO) of the LAD.
Relevant Catheterization Findings
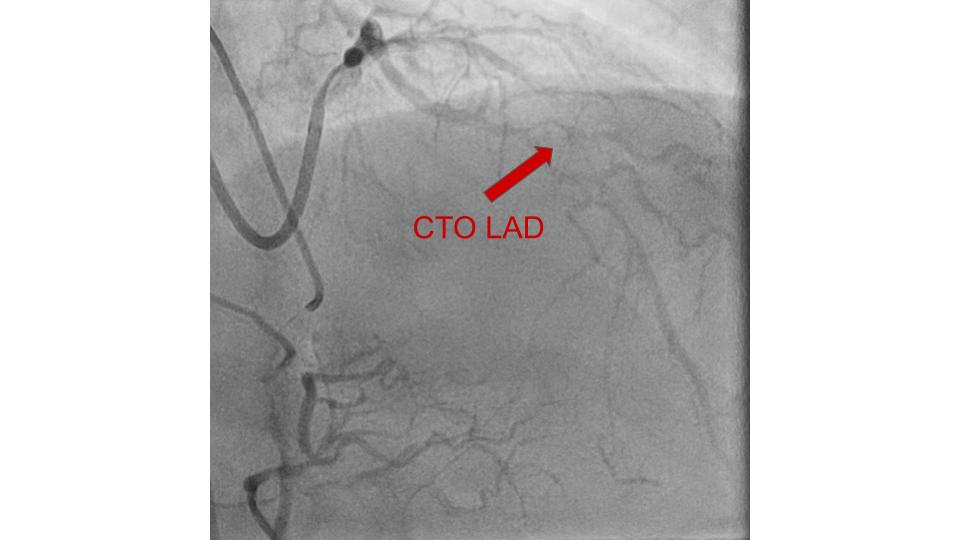
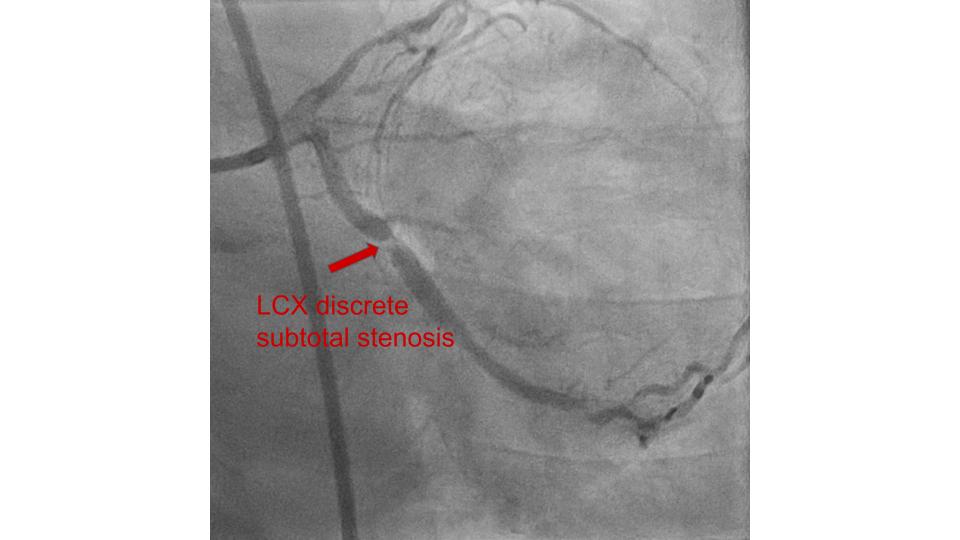
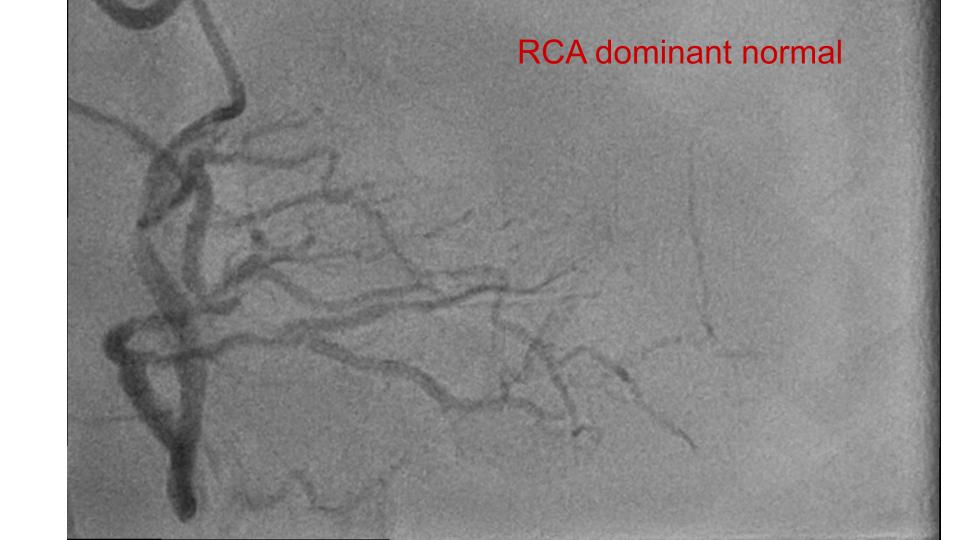
The angiography revealed a normal Left main Coronary Artery (LMCA), diffuse stenosis in the Left Anterior Descending (LAD) Artery with chronic total occlusion (CTO) at bifurcation of proximal LAD and diagonal-2, and significant stenosis at the distal part in the left circumflex artery (LCx). Right Coronary Artery (RCA) is Dominant and Normal.
Interventional Management
Procedural Step
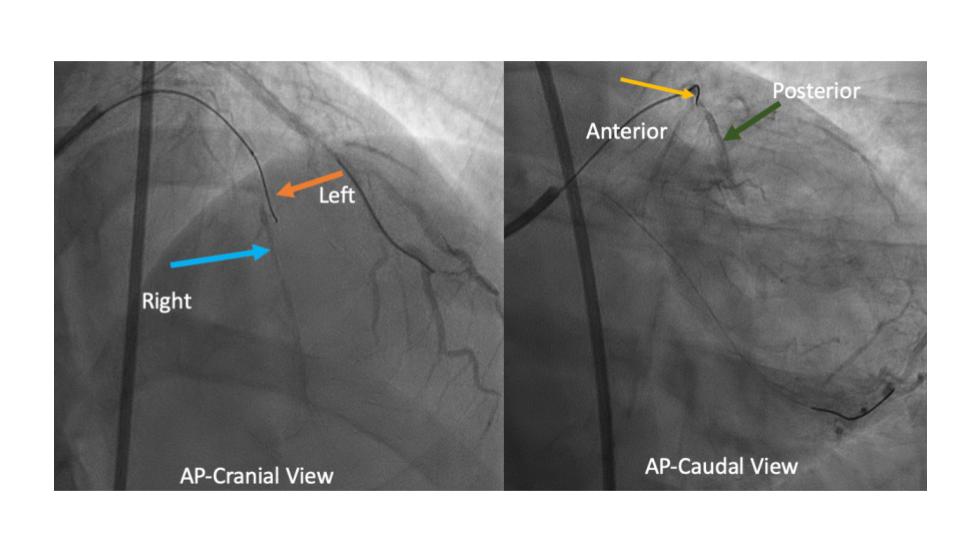
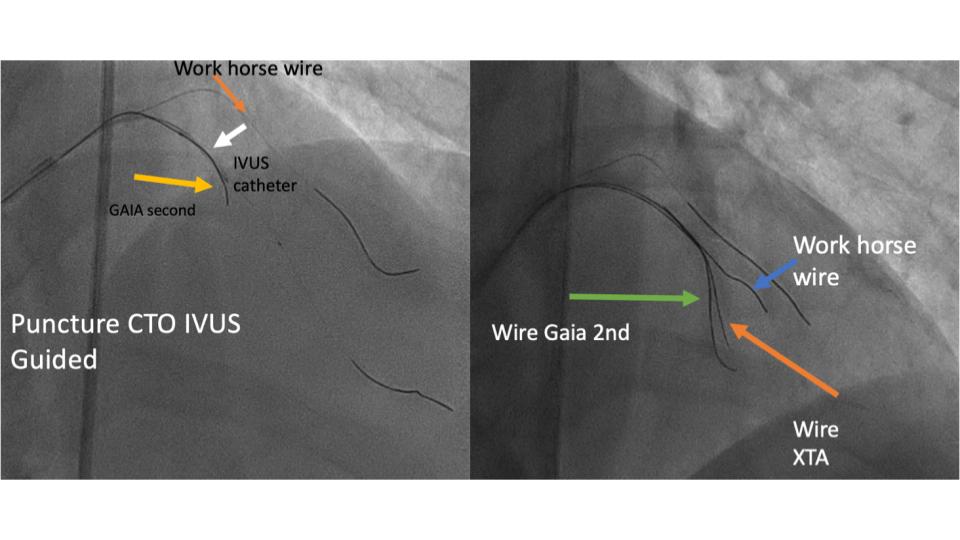
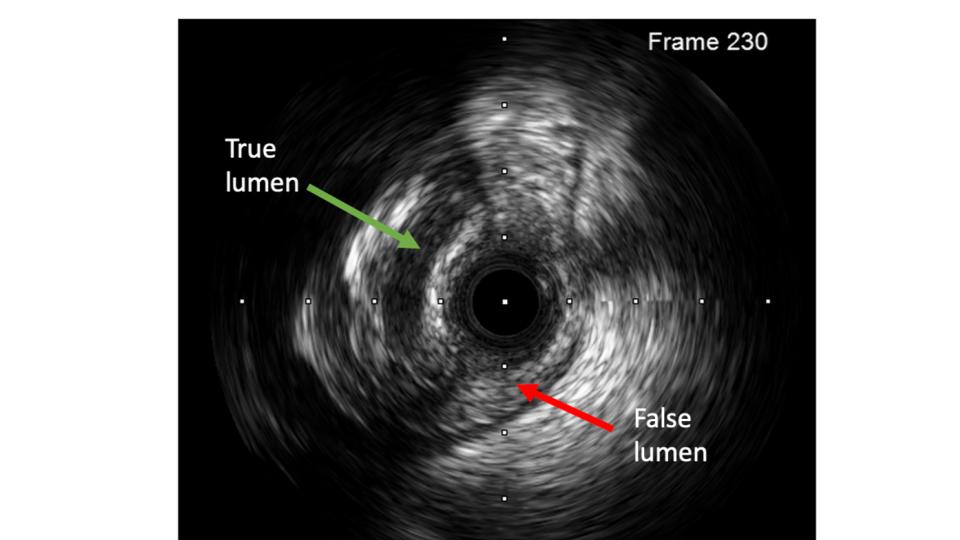
This case involved a PCI after successful punctures of the right radial and femoral arteries, allowing the insertion of 7F and 6F sheaths. Heparin (100 IU/kg) and nitroglycerin (300 mcg) were administered intra-arterially. The procedure began with dual angiography LCA with EBU 3.5/7F and RCA cannulation with GR JR 3.5/6F.An NS workhorse wire was placed in the distal LCx as an anchor. Initial attempts to access the proximal LAD with Finecross microcatheter were unsuccessful, prompting a redirection of the wire to the D2 branch while the microcatheter remained in the proximal LAD. Predilation was performed with an SC balloon. Further wiring attempts with a Gaia Next microcatheter did not penetrate the lesion. An IVUS Opticross catheter was introduced at the ostial D2 for IVUS-guided CTO puncture. Although the Gaia Next microcatheter crossed the lesion, it often entered the false lumen. A Fielder XT-A wire successfully traversed the lesion but also ended in the false lumen, where it was retained as an anchor. Another attempt with the Gaia Second microcatheter successfully accessed the distal LAD, confirmed by a tip injection. The wire was then exchanged for an NS workhorse wire in the distal LAD. Predilation with an SC balloon was performed. IVUS revealed a dissection distal to the LAD stent with underexpansion, whereas the LCx stent was well-apposed. Final angiography demonstrated favourable outcomes
Case Summary
This case highlights the significance of IVUS, the effective use of Modified Parallel Wire Technique by mapping proximal cap in navigating complex coronary lesions.This case report illustrates that chronic total occlusion (CTO) can be effectively addressed through IVUS-guided techniques utilising Modified Parallel Wire.Even when faced with a true-false-true lumen scenario, successful stenting was achieved.The integration of IVUS not only facilitated precise navigation but also enhanced the optimization of the percutaneous coronary intervention procedure.These results highlight the critical importance of IVUS in managing complex CTO cases, ultimately contributing to improved patient outcomes.