
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-065
Tackling a Stubborn Enemy
By Vicknesan Kulasingham, Lu Hou Tee, Gurudevan Mahadevan, Sim Jian Hao, Adelyn Nisha Nerin Henry, Kim Heng Shee, Nur Hazurreen Harryzan
Presenter
Vicknesan Kulasingham
Authors
Vicknesan Kulasingham1, Lu Hou Tee2, Gurudevan Mahadevan1, Sim Jian Hao1, Adelyn Nisha Nerin Henry1, Kim Heng Shee1, Nur Hazurreen Harryzan1
Affiliation
Sultanah Aminah Hospital, Malaysia1, Regency Hospital, Malaysia2,
View Study Report
TCTAP C-065
Coronary - Complex PCI - Calcified Lesion
Tackling a Stubborn Enemy
Vicknesan Kulasingham1, Lu Hou Tee2, Gurudevan Mahadevan1, Sim Jian Hao1, Adelyn Nisha Nerin Henry1, Kim Heng Shee1, Nur Hazurreen Harryzan1
Sultanah Aminah Hospital, Malaysia1, Regency Hospital, Malaysia2,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
67 years old lady with history of Hypertension, End stage Renal Disease on regular Haemodialysis presented to the emergency with history of typical angina at 4pm on 27 July which was relieved with GTN.Pain recurred the following day but did not respond to GTN hence she came to the hospital.She had no failure symptoms and no infective symptoms.Clinically pink, GCS full. BP 152/95, HR 78bpm and SPO2 100% without oxygen.Other examination finding was unremarkable.She was treated for NSTEMI.
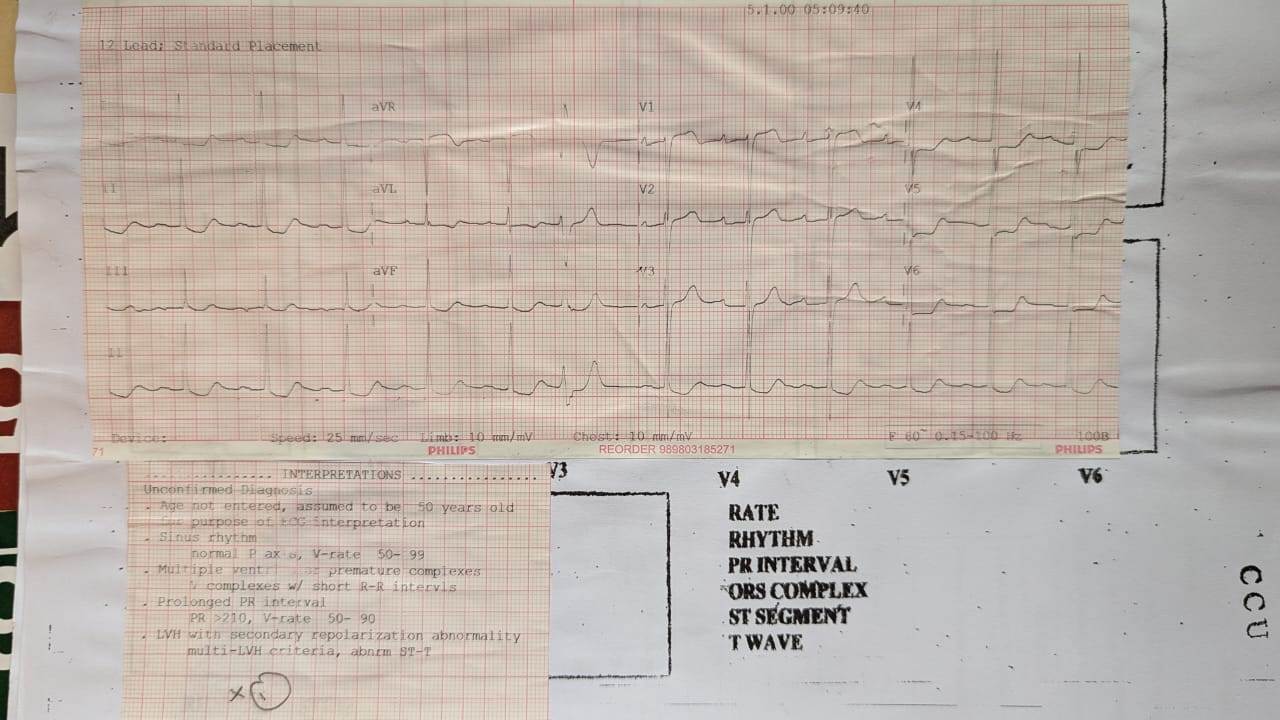
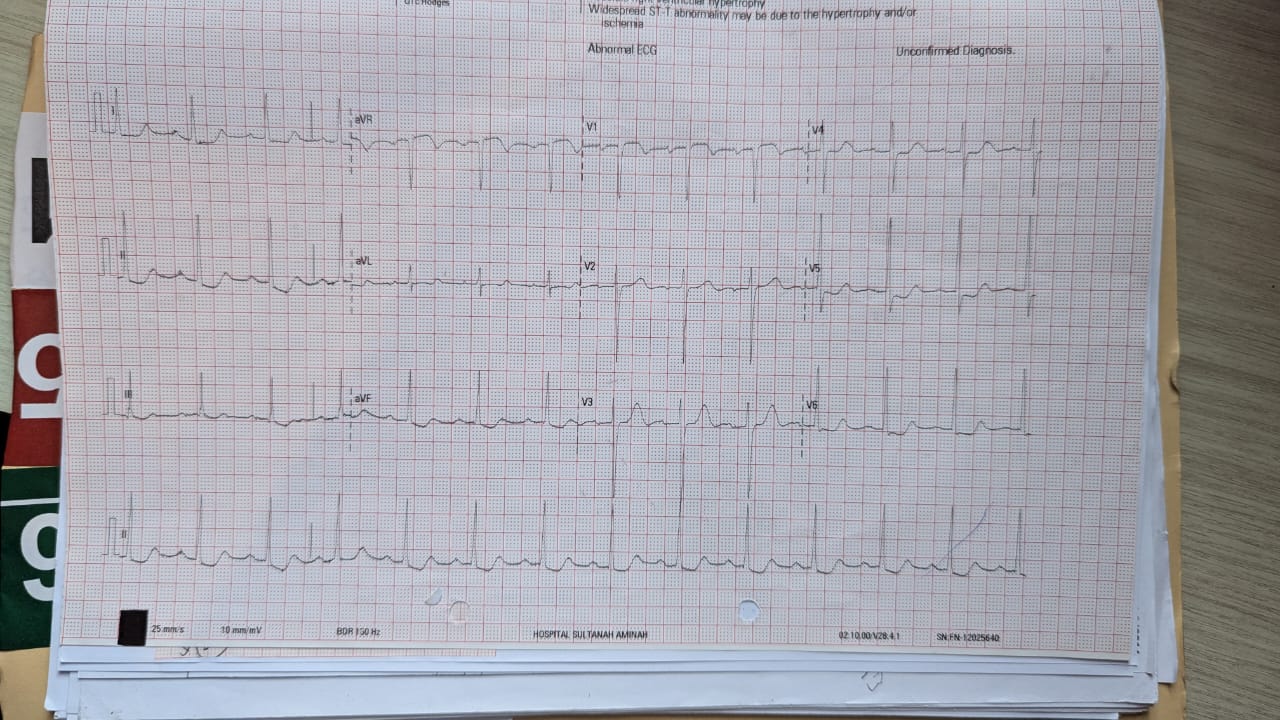
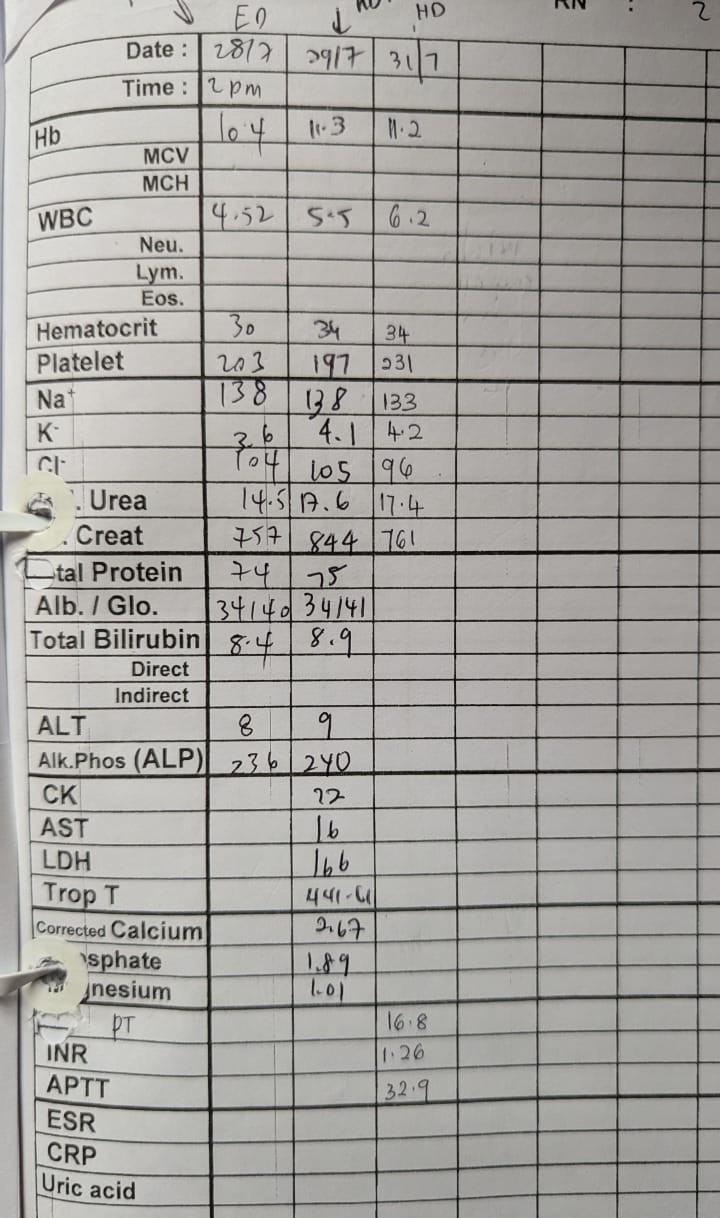
Relevant Test Results Prior to Catheterization
| |||||||||||||||||||||
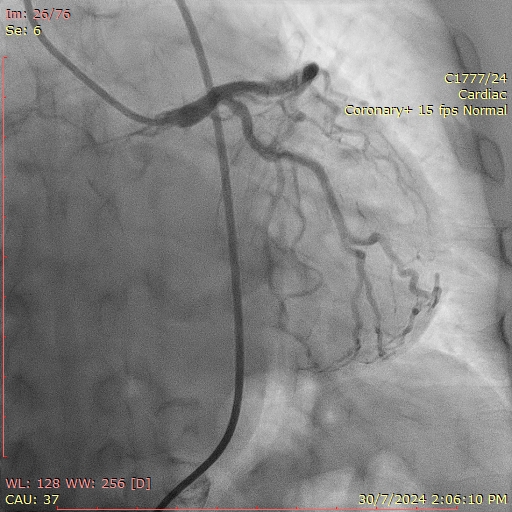
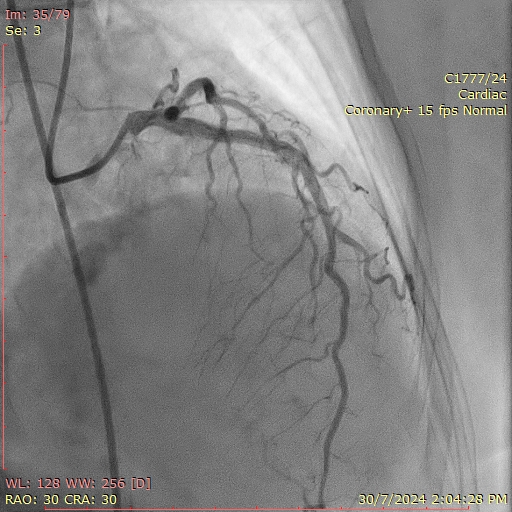
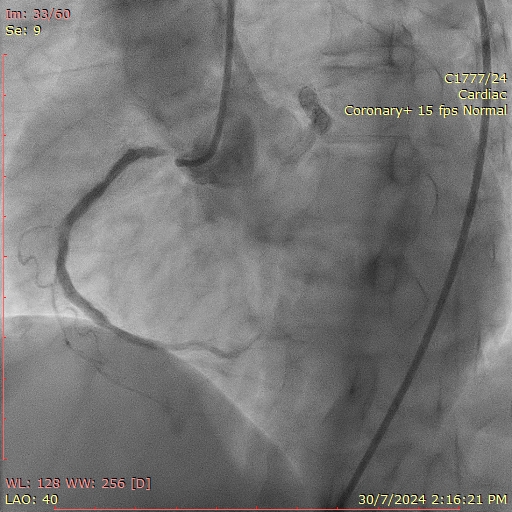
Relevant Catheterization Findings
Left main: NormalLAD stent patentLCX: Proximal 80%RCA: Proximal 50%, Mid RCA 99%, calcified
Interventional Management
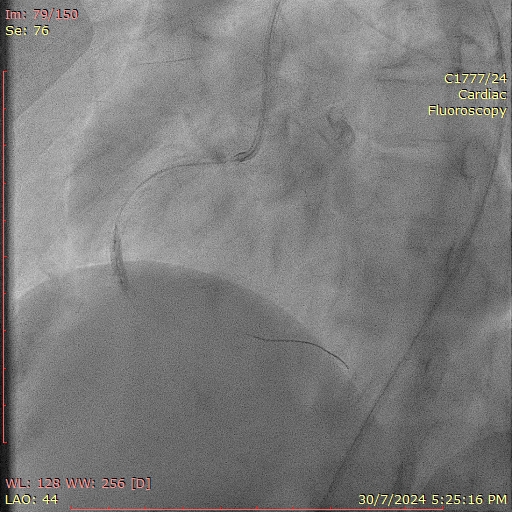
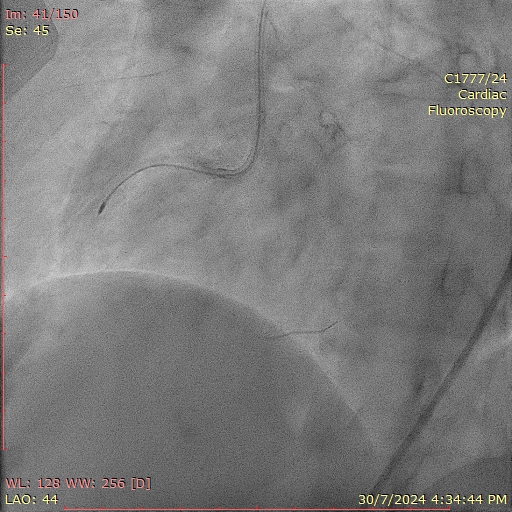
Procedural Step
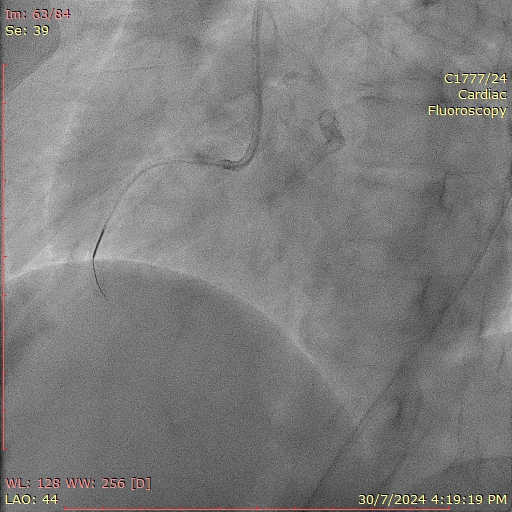
PCI to RCA.LFA approach,7Fr and attempted to engage with AL0.75 but failed. Changed to SAL0.75 but engaged non selective.Attempted to wire into RCA with sion blue and Finecross MC but failed.Changed to Gaia 2nd and managed to wire into DRCA but MC could not pass.Predilated with 1.2mm balloon but MC can't pass.Attempt to wire with rotadrive wire and runthrough floppy with MC at MRCA but failed.Changed to Fielder XTR and managed to wire into DRCA.Predilated with 0.85mm balloon followed by 1.0mm balloon but Finecross still could not pass.Changed to Turnpike LP MC and managed to advanced pass MRCA.Changed fielder to Rotawire.Rotablation with 1.25mm burr at 180krpm from mrca to ostial rca.predilated with NC 2.0mm, 3.0mm and cutting balloon 3.0mm.performed IVUS.Presence of circumferential calcium(min crack) and calcium nodule(no cracks).Decided for IVL 4.0mm and delivered 120pulses from mRCA to ostial RCA.IVUS performed, cracks seen. Stented mrca with des 3.5x38mm and prca 4.0x34mm.post dilated with NC 4.0mm. IVUS showed well expanded and apposed stent.TIMI 3 flow
Case Summary
Calcified lesion has been one of the well known "enemy" for interventional cardiologist and it is commonly seen in elderly and in patient on haemodialysis. In this case we had to use 2 calcium modification technique to get an optimal results. Using a combination of rotational atherectomy and intravascular lithotripsy balloon demonstrates the efficacy of hybrid approach. Rotablation effectively modifies the dense calcium and facilitates device delivery while IVL provides precise and controlled plaque fracture ensuring optimal luminal expansion. Importance of imaging no doubt has important role to characterise the lesion.