
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-060
The Seamless Guardian: Convenience in a New Paradigm
By Fauzi Nugraha, Pramon Sudjana, Aninka Saboe
Presenter
Fauzi Nugraha
Authors
Fauzi Nugraha1, Pramon Sudjana1, Aninka Saboe1
Affiliation
Hasan Sadikin General Hospital, Indonesia1,
View Study Report
TCTAP C-060
Coronary - Complex PCI - Calcified Lesion
The Seamless Guardian: Convenience in a New Paradigm
Fauzi Nugraha1, Pramon Sudjana1, Aninka Saboe1
Hasan Sadikin General Hospital, Indonesia1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
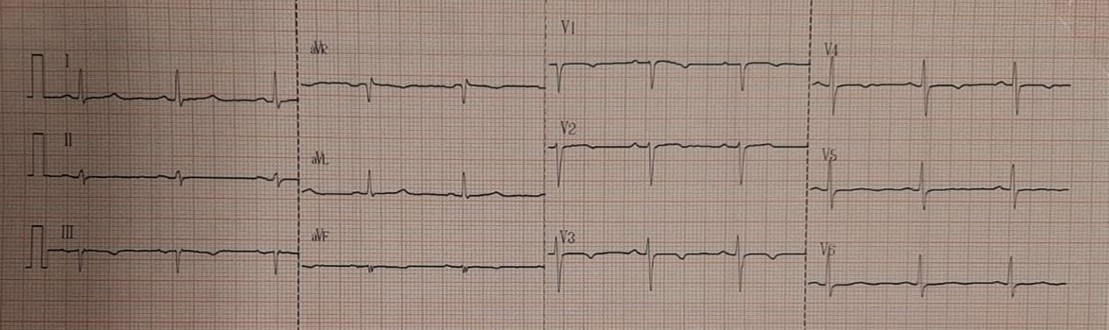
A 63-year-old female presented with exertional angina despite optimal medical therapy. She had a history of hypertension. Physical examination was unremarkable. The electrocardiogram showed T-wave depression in the anteroseptal wall, Laboratory examination revealed an estimated glomerular filtration rate (eGFR) of 83 ml/min/m2.
Relevant Test Results Prior to Catheterization
The Echocardiogram demonstrated preserved left ventricular ejection fraction. Coronary computed tomography angiography (CTA) revealed multivessel disease, with a calcium score (Agaston) of 2274, and a calcium score of 856 in left anterior descending (LAD) artery.

Relevant Catheterization Findings
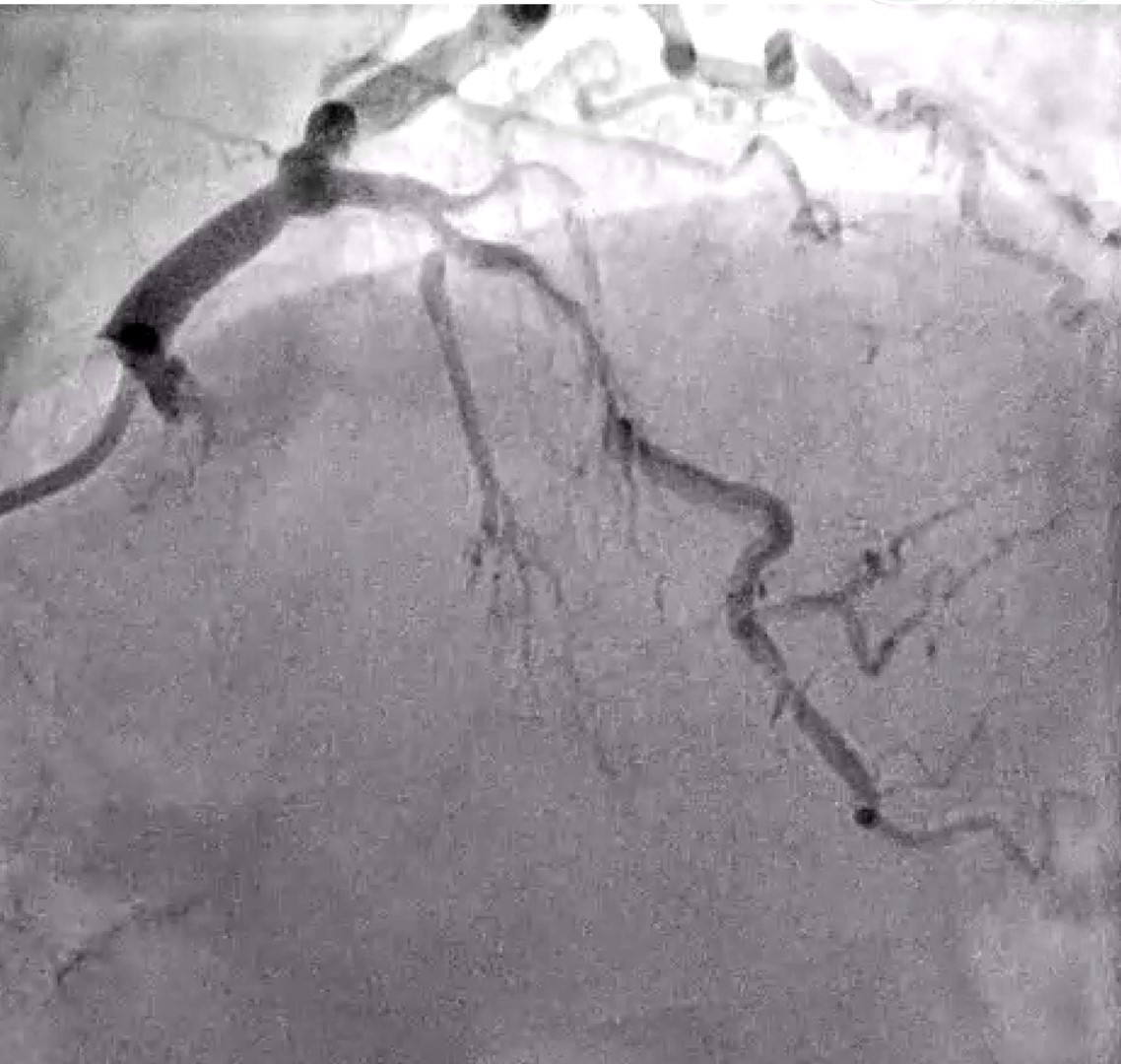
Coronary angiography (CAG) revealed multivessel disease and severe stenosis in the mid-portion of the LAD, with increase radiopacity indicative of heavy calcification

Interventional Management
Procedural Step
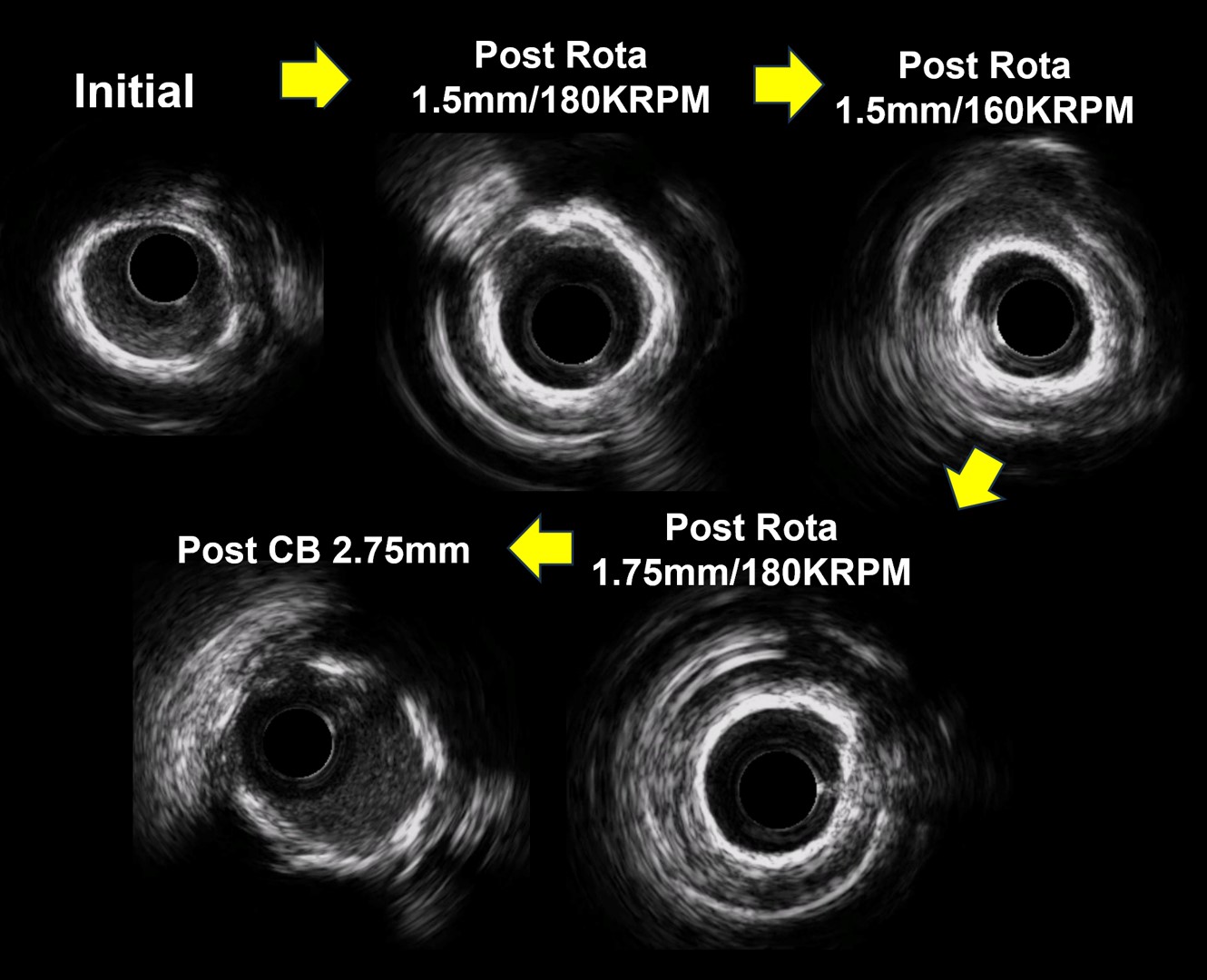
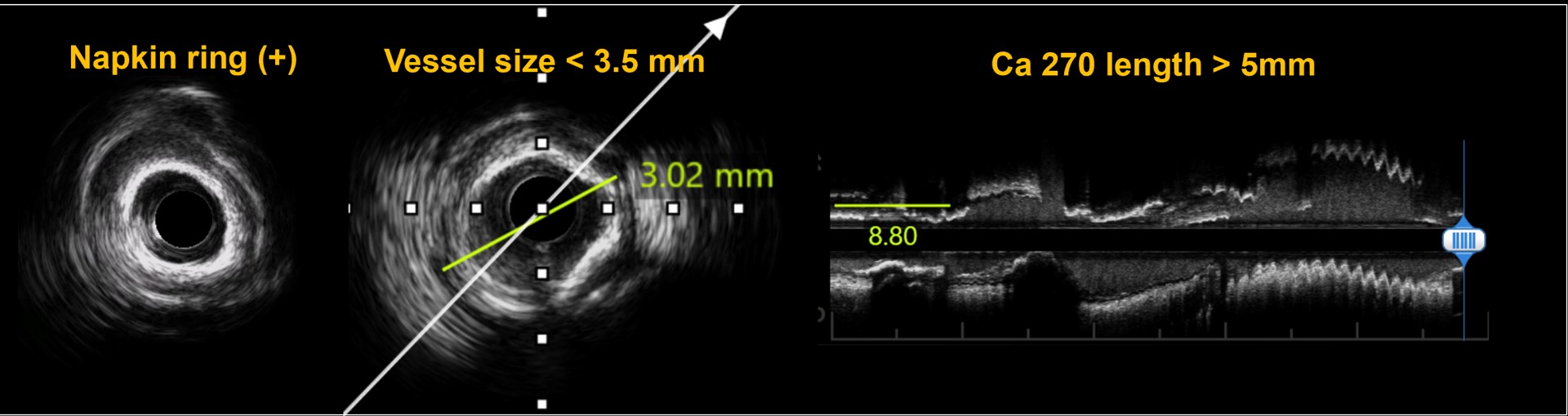
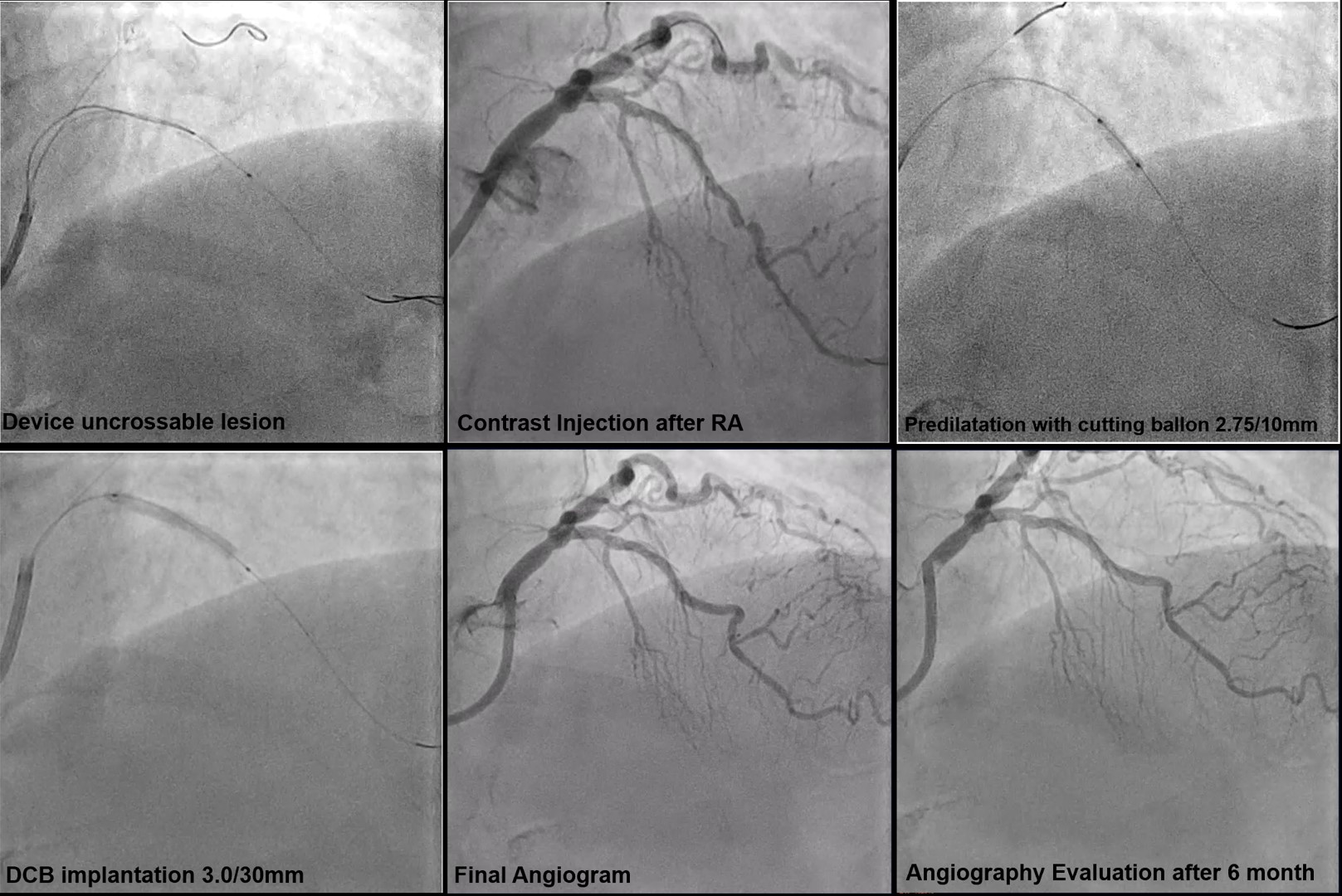
We chose left distal radial access with a 7Fr guiding catheter (EBU 3.5). Considering the need for atherectomy. After successfully passing the guidewire through the lesion, Intravascular ultrasound (IVUS) was performed. The IVUS catheter could not pass through the mid part of lesion, confirming the lesion as fibro-calcified lesion with IVUS calcium score of 3 (Napkin ring sign, lumen size < 3.5mm, calcium> 270o extending more than 5 mm). Rotational Atherectomy (RA) was then performed using 1.5 mm burr at speed 160.000 and 180.000 RPM followed by a 1.75mm burr at 160.000 RPM. Each step of RA guided and evaluated by IVUS. Lesion preparation continued with a cutting balloon (2.75/10mm). Final IVUS showed successful modification of calcified lesion, with multiple cracks, reverberation and increasing of lumen diameter. A DCB (Paclitaxel 3.0/30mm) was inflated at proximal-mid LAD for 1 minute. The final angiogram showed a good result without coronary flow disturbance. Three months later, a follow up angiogram revealed an improvement in vessel size at proximal-mid portion of LAD.
Case Summary
We present a case of diffuse calcified lesion treated with IVUS-guided PCI. Rotational atherectomy and a modified ballon were done for calcium modification, with IVUS evaluation at each step, leading to optimal lesion preparation. This approach resulted in a DCB-only strategy, which offer several advantages, particularly for long lesions, it avoids the potential failure to meet optimal DES implantation in calcified lesion, allows for a shorter duration of dual antiplatelet therapy (DAPT).