
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-142
A Twist of Fate: Handling a Broken Guidewire in the Aorta
By Hitendra Bhagwatkar
Presenter
Dr. Hitendra Bhagwatkar
Authors
Hitendra Bhagwatkar1
Affiliation
NKPSIMS & Lata Mangeshkar Hospital, India1,
View Study Report
TCTAP C-142
Coronary - Complication Management
A Twist of Fate: Handling a Broken Guidewire in the Aorta
Hitendra Bhagwatkar1
NKPSIMS & Lata Mangeshkar Hospital, India1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A 62-year-old male with systemic hypertension presented with 2-day history of chest pain radiating to the left shoulder, palpitations, and breathlessness on exertion. Vital signs: HR 86 bpm, BP 140/80 mmHg, RR 28/min, SpO2 96% on 5L O2, afebrile. Cardiovascular system examination revealed S1, S2, with S3. Respiratory system examination revealed basal crepitations. History of systemic hypertension, managed with medication.
Relevant Test Results Prior to Catheterization
Routine blood investigations were within normal limits. ECG was suggestive of heart rate of 150/min, right axis, normal standard with ST elevation in V1 to V4. 2D Echo was suggestive of Regional wall motion abnormalities (RWMA) in the left anterior descending (LAD) artery territory, hypokinesis, dilated LV apex, and ejection fraction (EF) of 20%.
Relevant Catheterization Findings
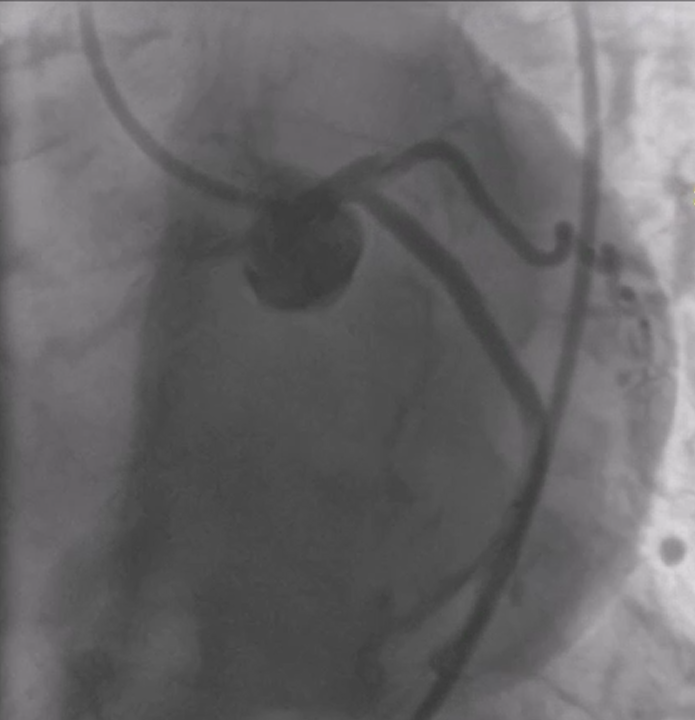
CAG revealed single vessel disease with total occlusion of the ostio-proximal LAD.
Interventional Management
Procedural Step
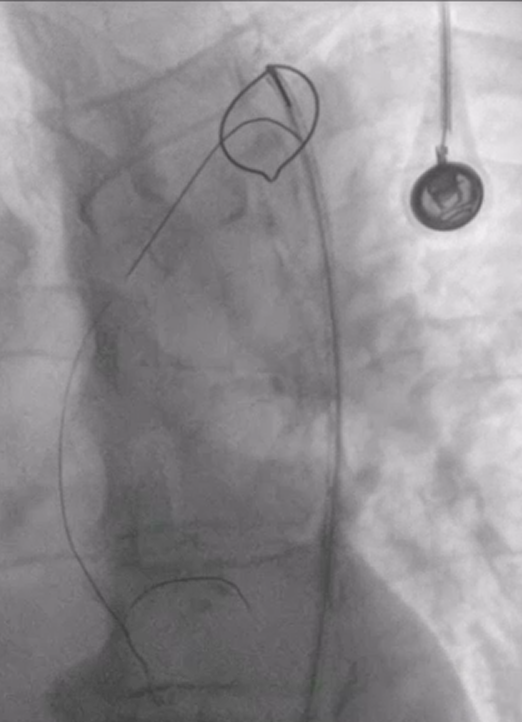
Procedural: The patient underwent percutaneous coronary intervention (PCI) for a chronic total occlusion (CTO) in the left anterior descending (LAD) artery. Initially, a GAIA II wire was used to cross the CTO, but it became stuck at the calcified ostio-proximal segment, and the distal wire tip fractured inside the catheter. A balloon catheter was employed to retrieve the broken wire, but the balloon shaft also broke and became lodged. A snare was used to extract both the wire and balloon, but the wire remained stuck in the aorta. The guide catheter was advanced through the fractured wire tip toward the proximal end, and after rotating the catheter, the wire was successfully removed. However, attempts to open the lesion with a soft wire failed due to the complexity of the occlusion. Given the inability to restore flow via PCI, the patient was referred for coronary artery bypass grafting (CABG). This case underscores the technical challenges of CTO PCI, particularly in calcified lesions, and the need for surgical revascularization when PCI is unsuccessful.

Case Summary
This case highlights the challenges of PCI for CTOs, particularly in calcified lesions, with complications like wire fractures and balloon shaft breaks. Despite multiple attempts, the lesion could not be opened, necessitating referral for CABG. It emphasizes the need for surgical revascularization when PCI fails.