
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-115
Crack the Rock for the Narrow Escape
By Apichai Marsukjai, Vorarit Lertsuwunseri
Presenter
Apichai Marsukjai
Authors
Apichai Marsukjai1, Vorarit Lertsuwunseri2
Affiliation
Charoenkrung Pracharak Hospital, Thailand1, King Chulalongkorn Memorial Hospital, Thailand2,
View Study Report
TCTAP C-115
Coronary - Complex PCI - Left Main
Crack the Rock for the Narrow Escape
Apichai Marsukjai1, Vorarit Lertsuwunseri2
Charoenkrung Pracharak Hospital, Thailand1, King Chulalongkorn Memorial Hospital, Thailand2,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
An 84-year-old female with underlying disease of paroxysmal atrial fibrillation and dyslipidemia was admitted with non-ST elevation acute coronary syndrome to the provincial hospital. Her blood pressure was 128/83 mmHg, her heart rate was 68 beats per minute. The coronary angiography showed left main disease with double vessel disease. The patient refused to CABG due to risk of operation and elderly age. She was referred for PCI at our center.
Relevant Test Results Prior to Catheterization
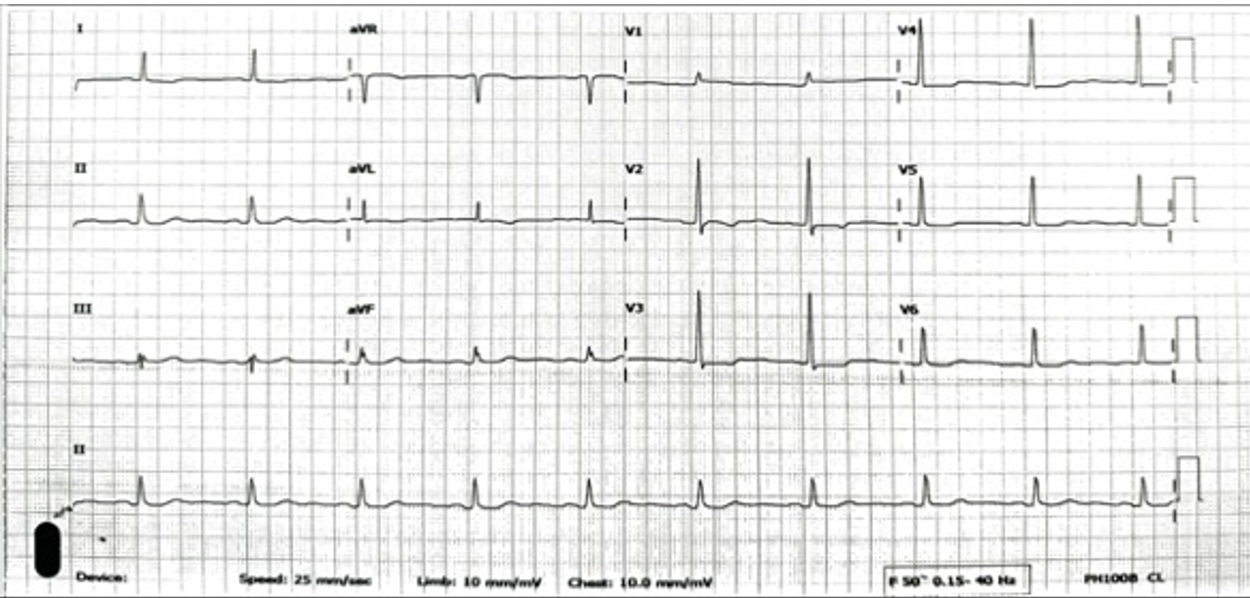
The initial electrocardiogram showed a sinus rhythm rate of 60 beat per minute with horizontal ST depression in V2 to V4. The transthoracic echocardiography demonstrated a left ventricular ejection fraction of 58% with anterior and anteroseptal wall hypokinesia from mid to apex and no significant valvular abnormalities. Basic laboratory results were normal.
Relevant Catheterization Findings
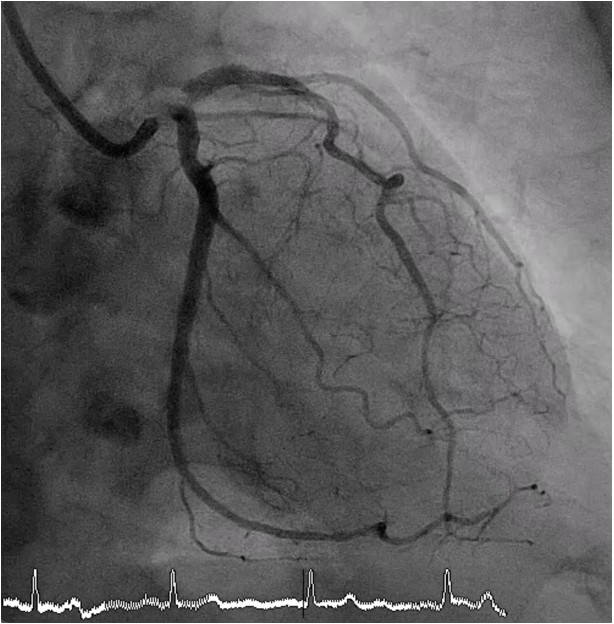
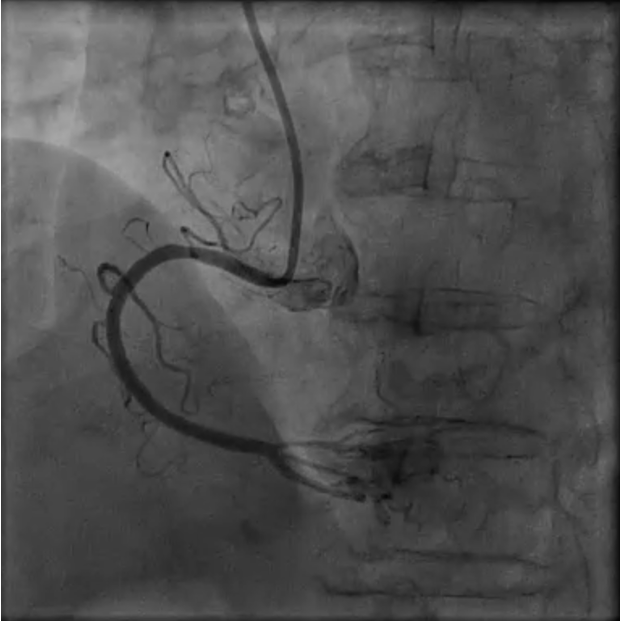
Coronary angiography revealed critical stenosis of the distal left main with calcified nodule at the left main bifurcation (Medina 1-1-1), 90% stenosis at ostial LAD and 90% stenosis at ostial LCx.
Interventional Management
Procedural Step
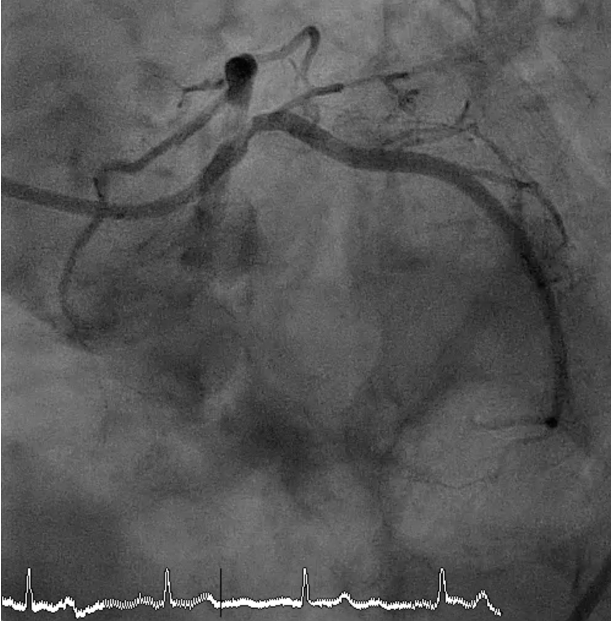
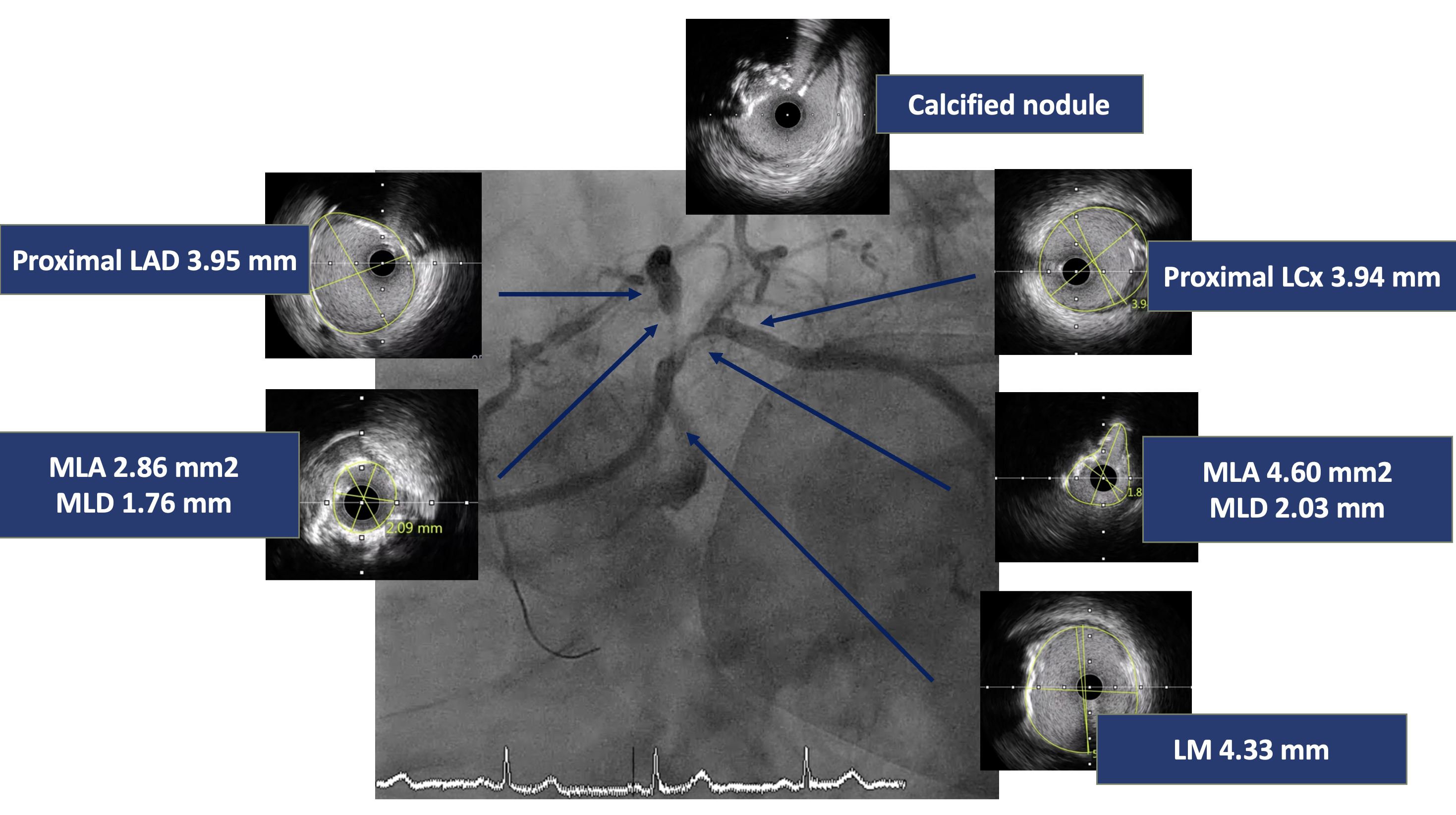
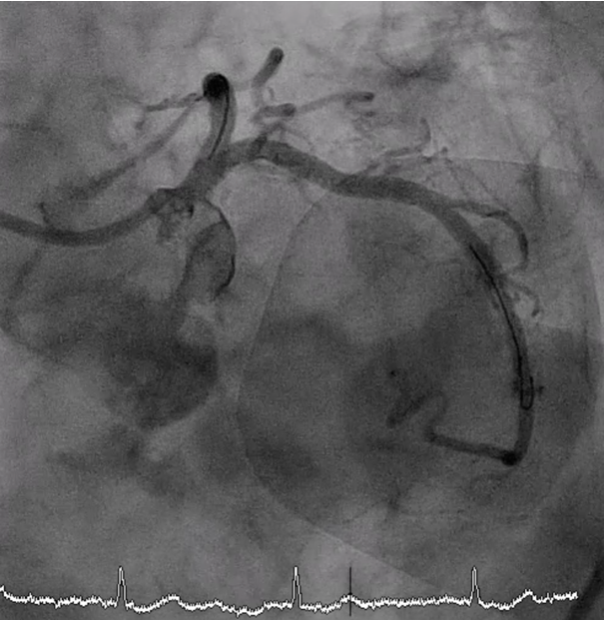
A 7 Fr JL 4.0 guiding catheter was engaged into LCA via RFA. We planned to perform PCI at LM bifurcation with Culotte technique. We successful wired to distal LAD using Finecross microcatheter with Conquest Pro guidewire (Failed using Sion blue, Fielder XT and Gaia Next2 guidewires). The microcatheter could not pass LAD lesion. Successfully passed the lesion using Tornus microcatheter. Then we exchanged RotaWire Floppy wire. Rotational atherectomy was done at LM-proximal LAD with Burr 1.25 mm at 180,000 rpm total 2 runs and step up Burr to 1.75 mm at 180,000 rpm total 2 runs for further debulking. Then we wired to LAD with Sion blue and LCx with Sion guidewires. IVUS was performed in LM, LAD and LCx. IVUS from LM-LAD showed eruptive calcified nodules with cracked calcific plaques and reverberation with MLA 2.86 mm2. IVUS from LM-LCx showed MLA 4.6 mm2. We prepare the lesion LM-LAD with non-compliant 4.0/15 mm balloon at 20 atm. A 4.0/18 mm stent was deployed from LM to LAD then re-wiring. We prepare the LM-LCx with semi-compliant 2.0/15 mm balloon (for opening strut) at 14 atm, 2.5/15 mm balloon at 14 atm and non-compliant 4.0/15 mm balloon at 20 atm. A 4.0/23 mm stent was deployed from LM to LCx. The KBI was performed with non-compliant 4.0/15 mm balloons at 10 atm. POT was performed with non-compliant 4.0/15 mm balloon at 14 atm. Final angiogram showed good coronary blood flow and IVUS demonstrated well stent expansion, no malapposition and no stent edge dissection.
Case Summary
Left main bifurcation PCI with calcified nodule is challenging due to it causes high risk of stent underexpansion. Multimodality techniques were used for wiring and plaque modification in this case. Intravascular imaging is also useful in determining strategy and technique for optimizing left main bifurcation PCI outcome.