
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-073
The Approach of the Long Length of In-Stent Restenosis Associated Chronic Total Obstruction: A Case Report
By Kuo-Ming Yang
Presenter
Kuo-Ming Yang
Authors
Kuo-Ming Yang1
Affiliation
Kaohsiung Veterans General Hospital, Taiwan1,
View Study Report
TCTAP C-073
Coronary - Complex PCI - CTO
The Approach of the Long Length of In-Stent Restenosis Associated Chronic Total Obstruction: A Case Report
Kuo-Ming Yang1
Kaohsiung Veterans General Hospital, Taiwan1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
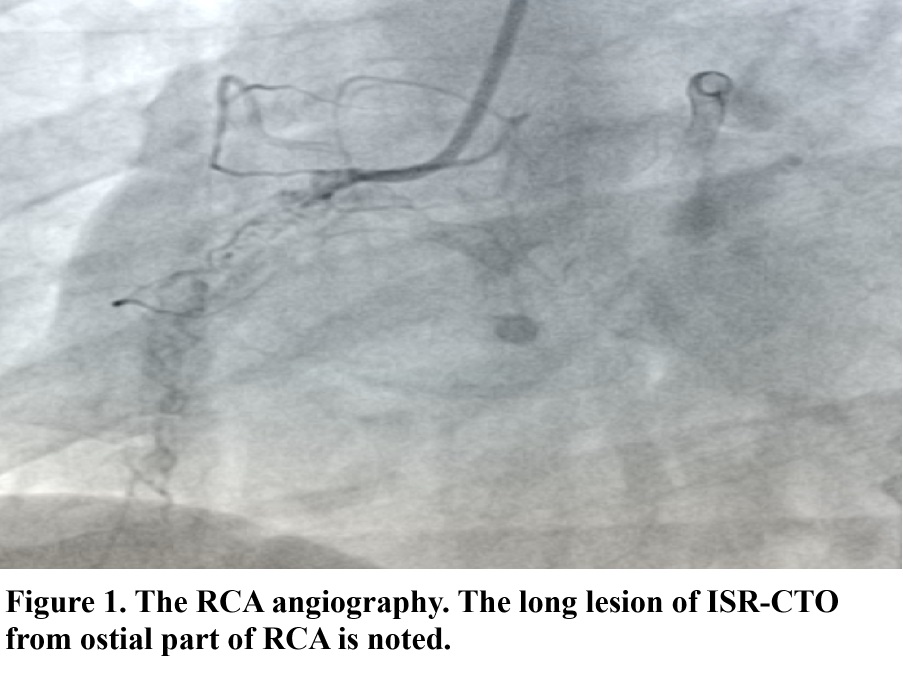
This is a 39-year-old male smoker with CAD s/p stenting in 2013. However, his symptoms were deteriorated gradually. He presented to our outpatient clinic for help in 2021. After survey, the positive result of myocardial perfusion scan was detected. He received 1st PCI in 2021 but a long ISR-CTO lesion in RCA was noted (Fig. 1). Thus, further strategy of recanalization was necessary. The 2nd PCI was provided for recanalization of this ISR-CTO lesion in 2022. No other specific finding was noted.
Relevant Test Results Prior to Catheterization
Theseries tests were provided on him prior to catheterization including laboratorytest, chest X-ray, electrocardiography, echocardiography, andmyocardial-perfusion scan. The echocardiography showed 47% of left ventricularejection fraction with mild hypokinesia of left ventricular inferior wall. 30-50% decreased perfusion in inferoseptal andinferior walls was detected by myocardial perfusion scan. The rest of testswere unremarkable.
Relevant Catheterization Findings
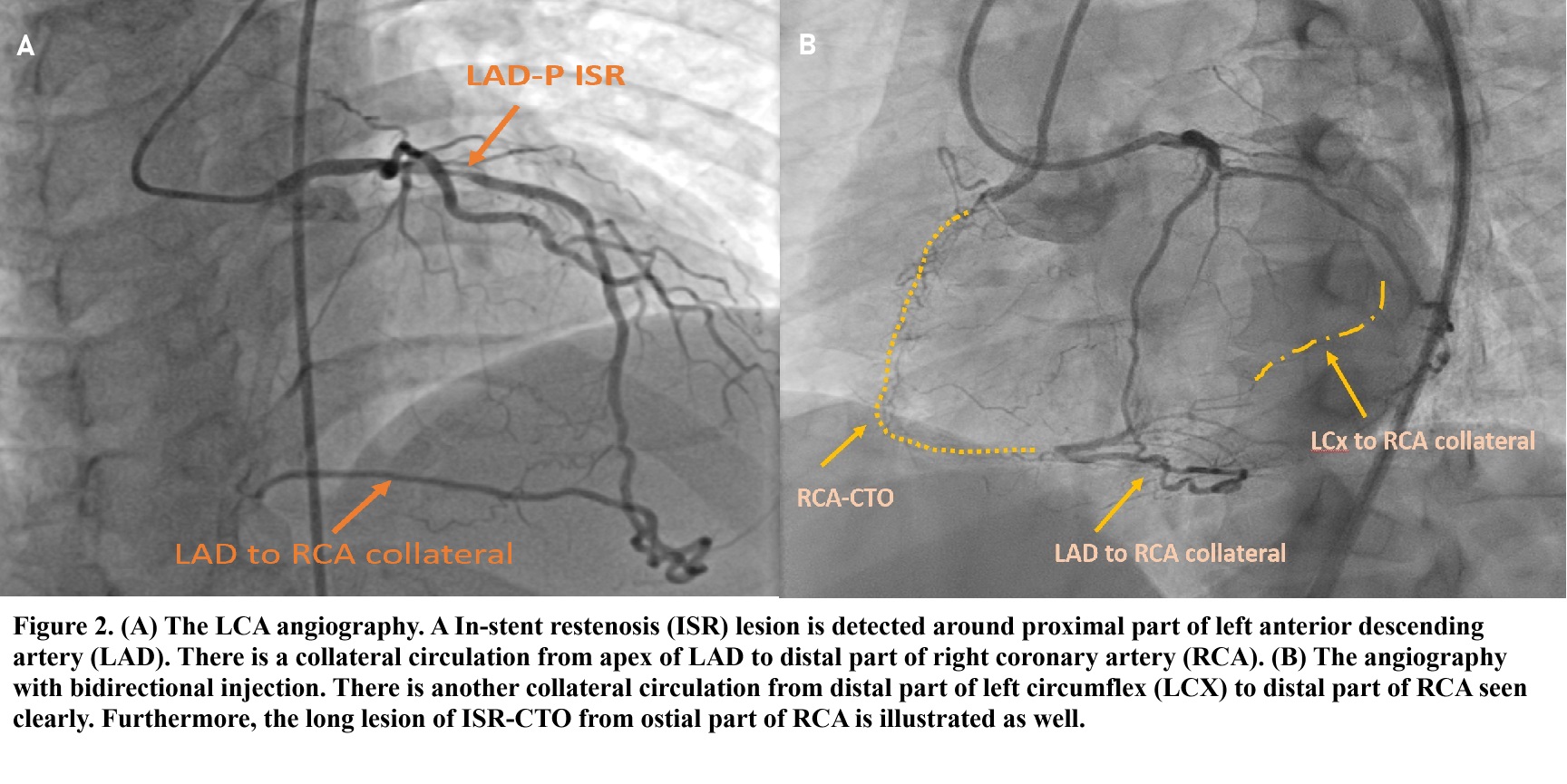
During the 2nd PCI, the bidirectional injection was done. An ISR lesion in proximal part of LAD with two collateral supplies from LAD and LCx to distal part of RCA was noted. The length of ISR-CTO lesion in RCA was from ostial part to distal part. The angiography was showed as figure 2.
Interventional Management
Procedural Step
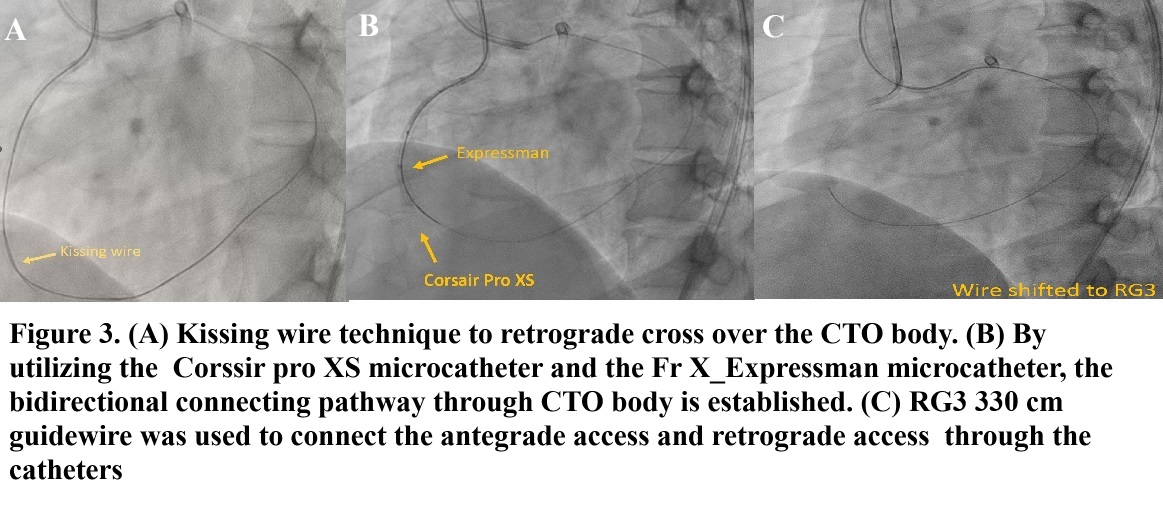
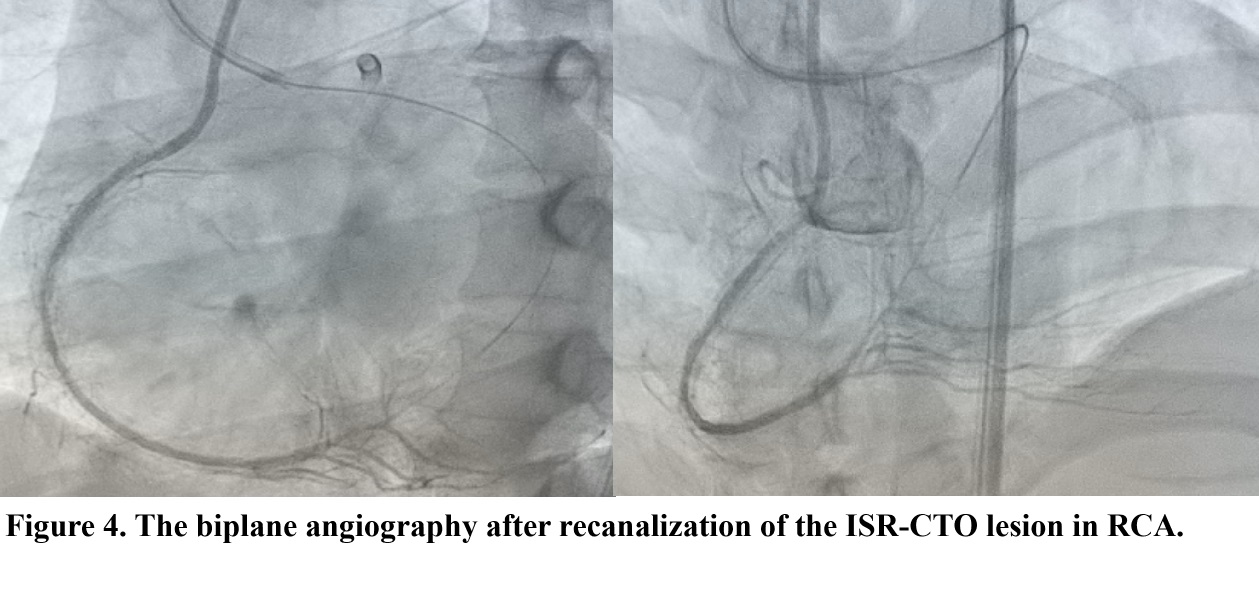
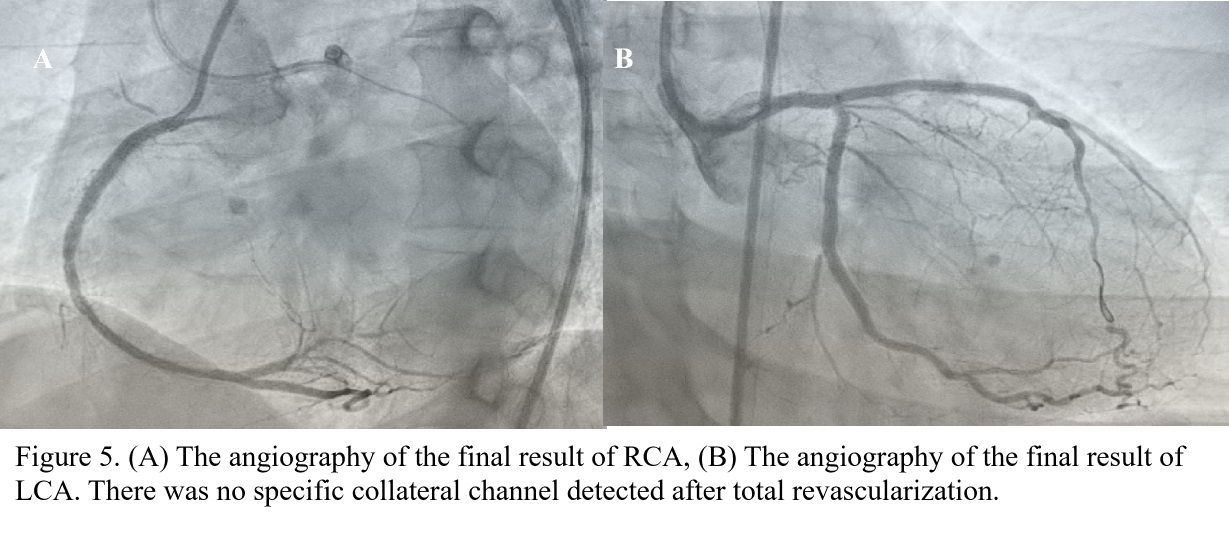
In terms of CTO lesion, the hybrid technique was considered. The conquest pro CTO guide wire with finecross microcatheter was used to penetrate through lesion antegradely but failed due to hard CTO body. Retrograde approach with gaia 3rd CTO guide wire and caravel microcatheter through LCX collateral circulation was utilized. Kissing wire technique was used to establish the connection bidirectionally as figure 3A illustrated. Several small balloons were used to dilate the CTO lesion afterwards. The 2.1 Fr x 150 cm Corssir pro XS microcatheter and the 6.0 Fr X_Expressman microcatheter were utilized to establish the connecting pathway bidirectionally based on the kiss wire technique (figure 3B). Furthermore, RG3 330 cm guidewire was used to connect the antegrade access and retrograde access through the catheters (Figure 3C). Figure 4 illustrated the result of recanalization of the ISR-CTO lesion after larger balloons dilatation. Secondary, theintravascular ultrasound (IVUS) was applied to check the CTO lesion condition,size and length carefully. In terms of the observed lesions, 3.5x30 and 3.0x30 support C drug coating balloons (DCB) were used to manage the ISR-CTOlesion in RCA, 2.5x18 mm Resolute Onyx stent and 3.0x48 mm Eucatech AG stent were implanted in posterior-lateral vessel (PLV) around RCA and proximal part of LCX, and 3.5x15 mm support C DCB was used to fix the ISR in LAD-M. After total revascularization, TIMI 3 flow without any complication was noted as figure 5 showed.
Case Summary
Afterassessing this patient’s characters, it was a highly complex PCI case. The J-CTOscores to his lesion were higher than 4, and the documented successful rate wasabout 73%. The lower procedural success rate for ISR-CTO lesion compared to denovo CTO lesion was also reported previously (86.0% vs. 90.3%). Thus, hydrideapproach was utilized for recanalization of the ISR-CTO lesion to increase theprocedural success rate. Furthermore, the appropriate device approach andexperienced operator were also the specific factors to increase the successfulrate. By utilizing severe CTO-PCI devices, the long ISR-CTO lesion wasrecanalized successfully.