
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-100
A Challenging Case Report: IVUS-Guided Retrograde Tip-in for RCA PL CTO
By Po Hsueh Su
Presenter
Po Hsueh Su
Authors
Po Hsueh Su1
Affiliation
Taiwan National Cheng Kung University Hospital, Taiwan1,
View Study Report
TCTAP C-100
Coronary - Complex PCI - CTO
A Challenging Case Report: IVUS-Guided Retrograde Tip-in for RCA PL CTO
Po Hsueh Su1
Taiwan National Cheng Kung University Hospital, Taiwan1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
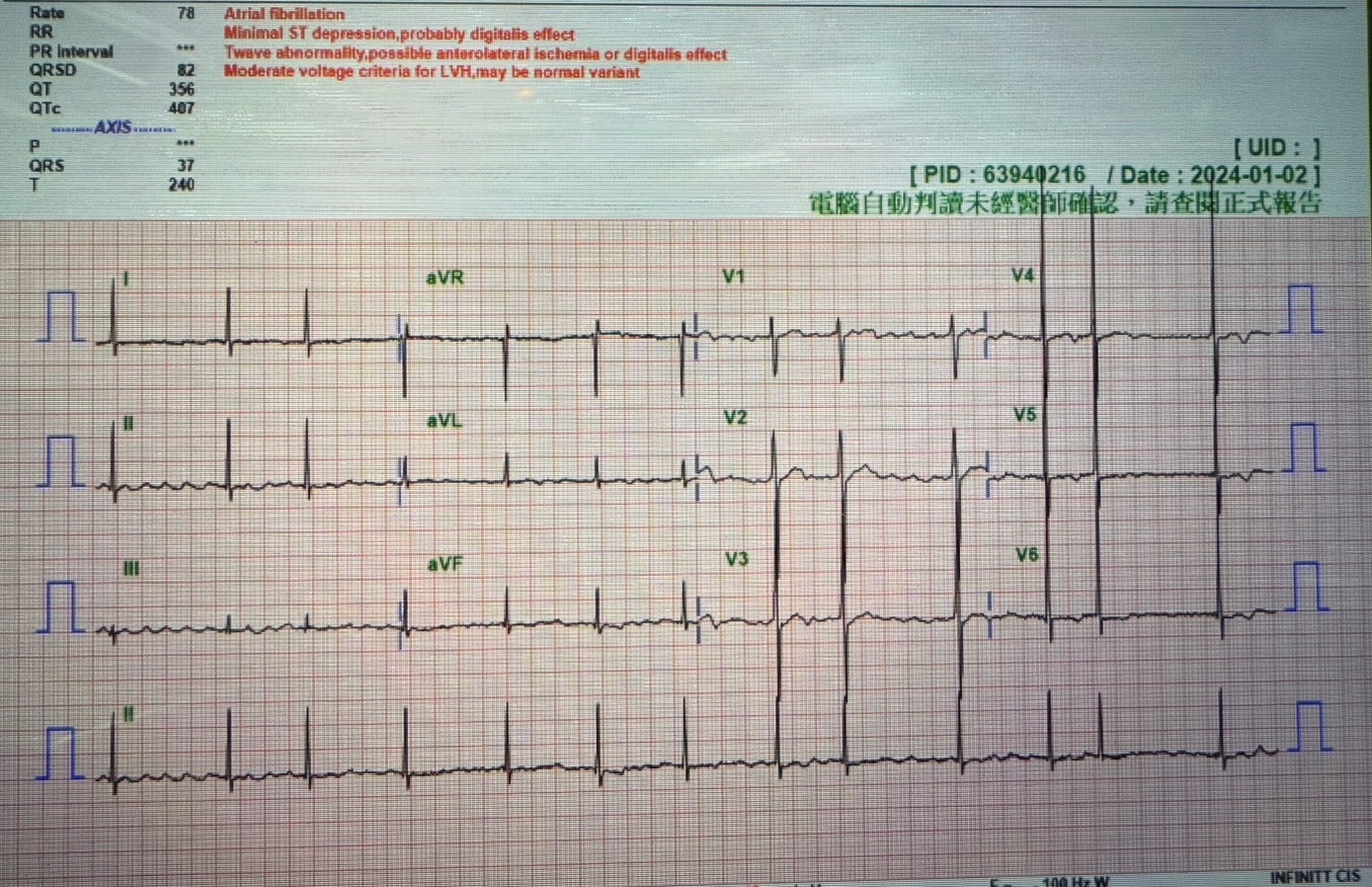
This is a 72-year-old male patient presented with chest tightness for days, then he was brought to our hospital. He had underlying disease of hypertension, diabetes mellitus, Dyslipidemia, Sick sinus syndrome, status post permanent pacemaker implantation and atrial fibrillation under chronic medical treatment. Physical examination showed irregular heart beats and mild lung congestion. Thallium scan revealed positive and invasive coronary angiography was indicated.
Relevant Test Results Prior to Catheterization
Thallium scan
Stress- induced ischemia at inferolateral to inferior wall(medium extent) is favor
Stress- induced ischemia at inferolateral to inferior wall(medium extent) is favor
Relevant Catheterization Findings
CAD/LM+3VD, distal RCA 90% stenosis, PL CTO, distal LM 70% stenosis, proximal to middle LAD 80% stenosis, distal LAD myocardial bridge, middle LCX 50% stenosis, s/p DES*2 at LM-mLAD, antegrade failure approach PL branch on 2024/03/13, successful retrograde approach for PL from epicardial channel, s/p DES*2 at m-dRCA to PL on 2024/04/10.
Interventional Management
Procedural Step
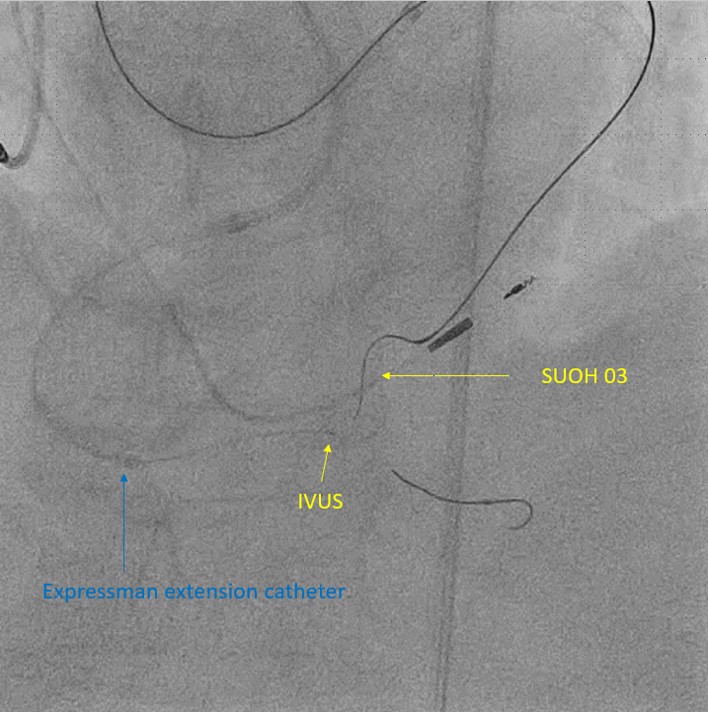
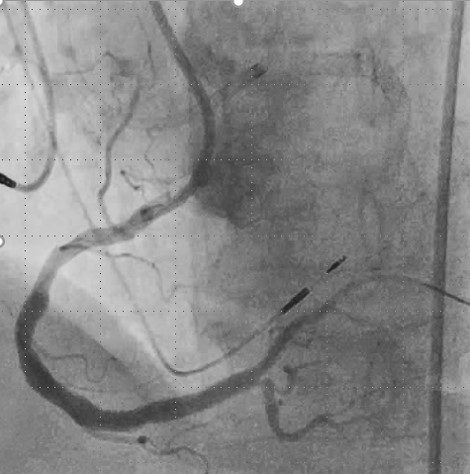
1. We tried to used SAL1/SH/7F guiding catheter to engage RCA orifice and EBU3.75/SH/6F for LM orifice to have bilateral injection. 2. The runthrough wire to PDA and used IVUS to view proximal PL CTO CAP and localized at fluoroscopy. 3. We tried a Caravel microcatheter with fielder FC to explore PL CTO antegradely, then tried Gaia II, but failure to advance. 4.We tried retrograde approach through LCX epicardial channel. 5.We used caravel microcatheter with SIOH and SUOH wire and successful reach proximal PL CAP, but failure to advance due to the hard texture. 6.We tried Gaia II and Conquest Pro, and successfull retrograde reach distal RCA. 7.Due to Caravel couldn't advance to PL proximal Cap, we used Ryurei balloon and mini TREK 1.5*6 balloon to dilated PL with 14 bars. 8. The conquest pro 9 wire was tip in antegrade microcatheter and tried to use fielder FC to reach PL. 9. We used a TREK 2.5*15mm balloon to have kissing technique at PL and PDA. 10.A Xience sierra 3.0*33 stent was deployed at dRCA to PL with 10 bars. 11.A Xience sierra 4.0*33mm stent was deployed at dRCA with 10 bars. 12.Post stent dilatation with a NC TREK 4.5*15mm balloon NC TREK 3.0*15mm balloon with 20 bars. 13.IVUS showed well stent expansion. 14.Final angiography showed better RCA flow and no extravasation at LCX epicardial channel.

Case Summary
CAD/LM+3VD, distal RCA 90% stenosis, PL CTO, distal LM 70% stenosis, proximal to middle LAD 80% stenosis, distal LAD myocardial bridge, middle LCX 50% stenosis, s/p DES*2 at LM-mLAD, antegrade failure approach PL branch on 2024/03/13, successful retrograde approach for PL from epicardial channel, s/p DES*2 at m-dRCA to PL on 2024/04/10.