
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-227
A Challenging Case Report: Crush the Barrier to Rebuild the Flow
By Kuan-Yu Lin, Jen-Kuang Lee
Presenter
Kuan-Yu Lin
Authors
Kuan-Yu Lin1, Jen-Kuang Lee1
Affiliation
National Taiwan University Hospital, Taiwan1,
View Study Report
TCTAP C-227
Endovascular - Iliac / SFA Intervention
A Challenging Case Report: Crush the Barrier to Rebuild the Flow
Kuan-Yu Lin1, Jen-Kuang Lee1
National Taiwan University Hospital, Taiwan1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
An 84-year-old male suffered from a non-healing left toe wound for months. He underwent femoral bypass surgery with a covered stent between the distal graft and P1 segment of popliteal artery, following unsuccessful endovascular therapy for chronic total occlusion of left superficial femoral artery (LSFA CTO) three months ago. Despite subsequent antibiotic treatment, the wound showed gangrenous change with pulselessness and poikilothermia on physical examination.

Relevant Test Results Prior to Catheterization
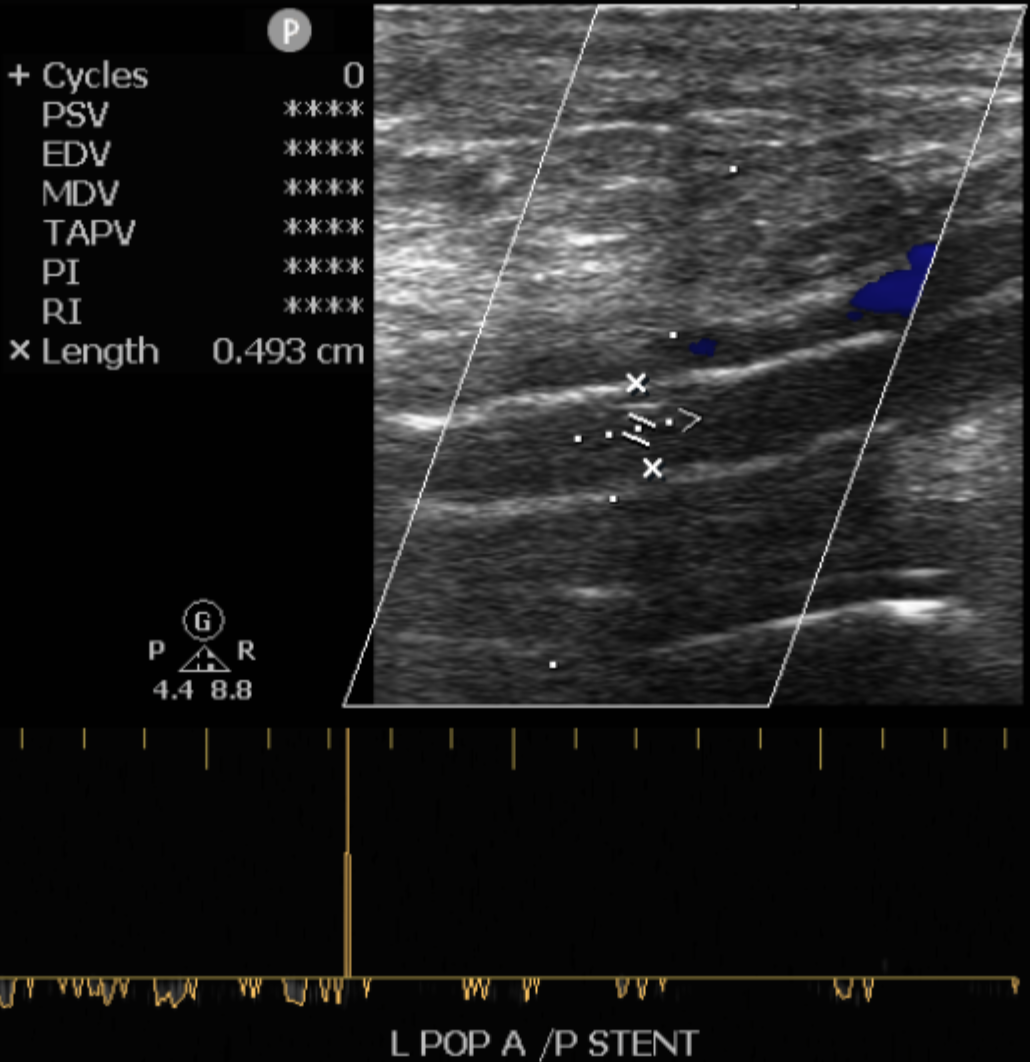
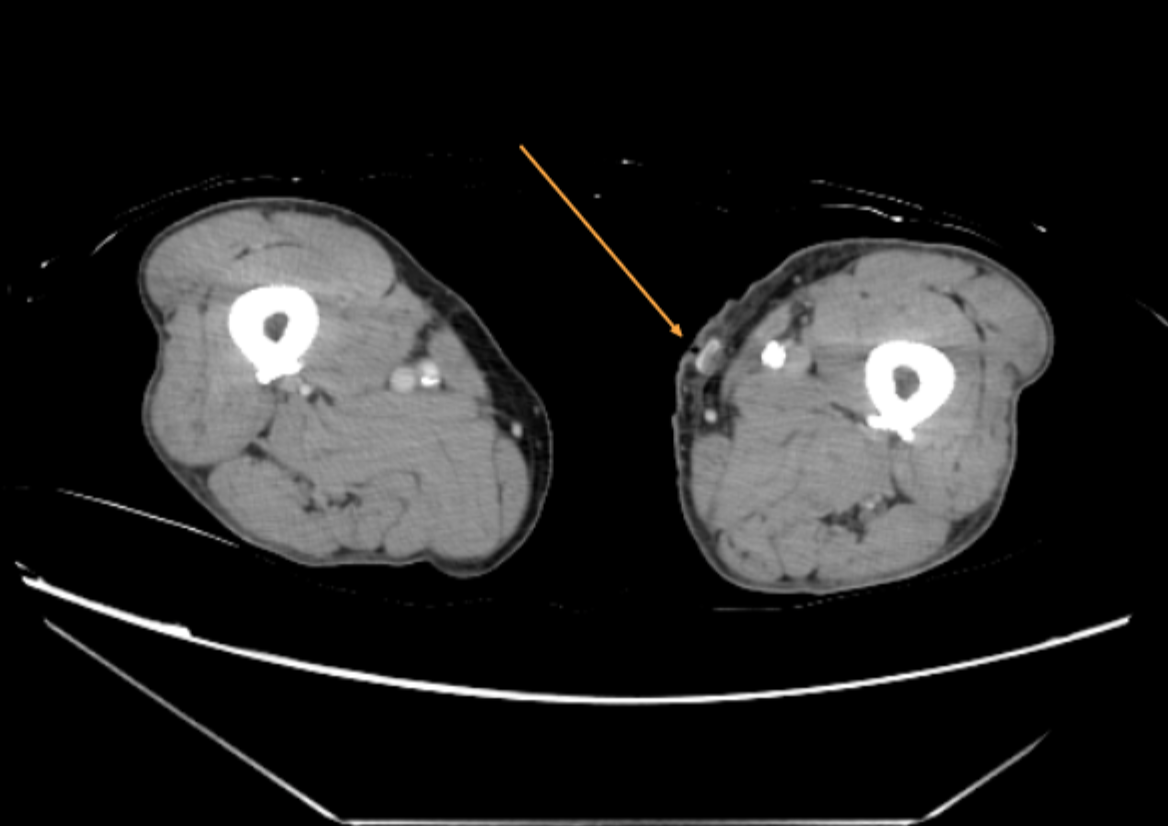
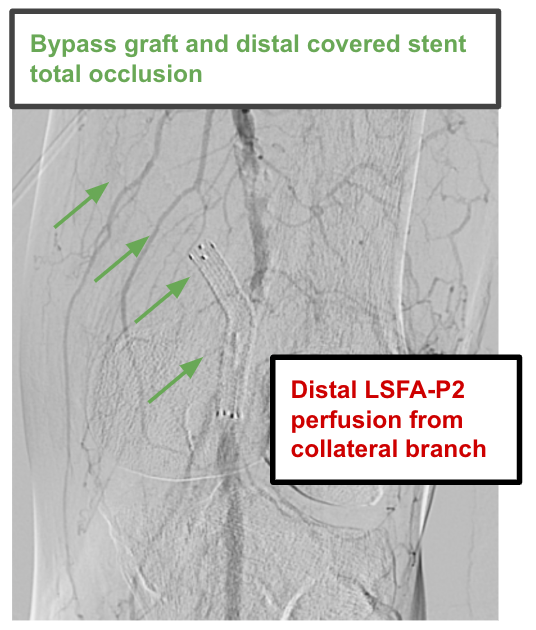
A lower limb vascular doppler ultrasound was performed, revealing absent flow through the left bypass graft and popliteal stent, with collateral vessels supplying the distal popliteal artery. Subsequent Computed Tomography Angiography (CTA) confirmed near-total thrombosis of the graft. As a result, endovascular revascularization was planned for the LSFA CTO.
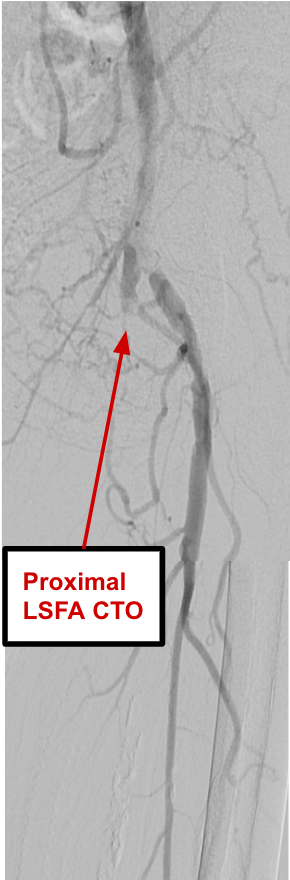
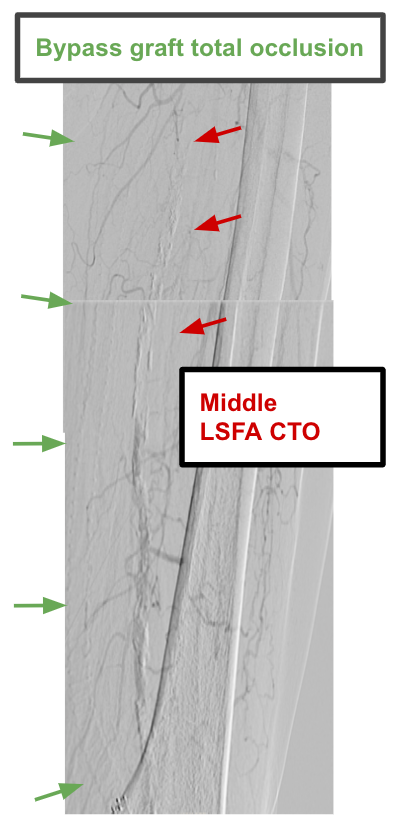
Relevant Catheterization Findings
1. Common to External iliac artery (CIA-EIA): 80% focal stenosis2. Common femoral artery (CFA): Patent3. SFA: CTO4. CFA bypass graft with distant covered stent connecting to P1 segment: Total occlusion5. Popliteal artery: Patent in P2-P3 segment from collateral branches6. Below the knee: 70% stenosis at proximal anterior tibial artery (ATA); Peroneal and Posterior tibial artery were patent7. Below the ankle: Dorsalis pedis and dorsal-plantar arch were patent but relatively slow flow
Interventional Management
Procedural Step
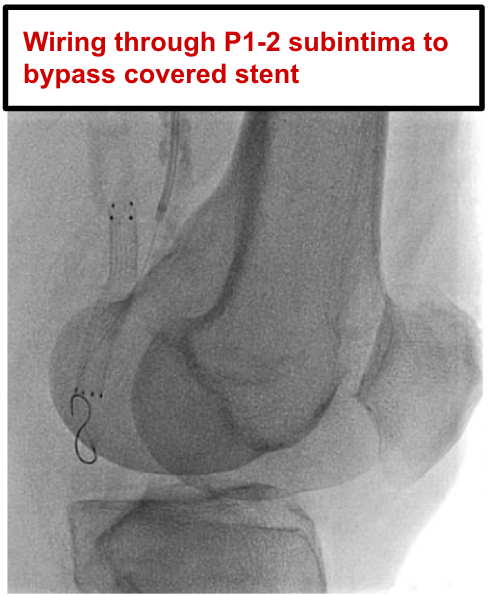
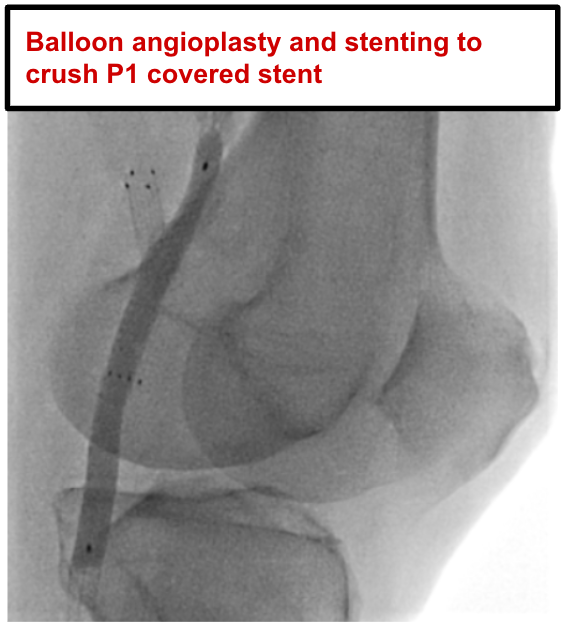
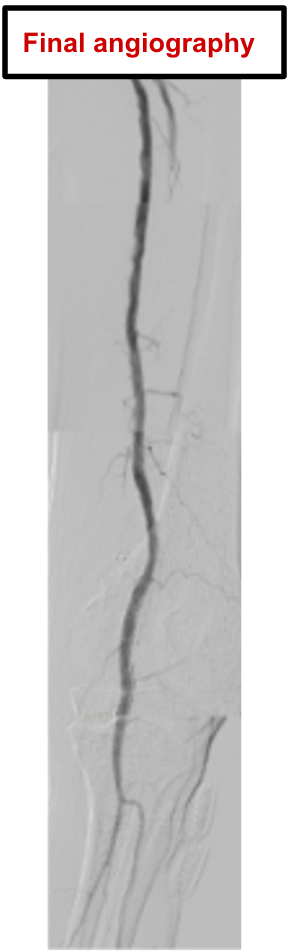
From a right femoral approach with an ANL0 guiding sheath to LCIA, we performed balloon angioplasty at LCIA-LEIA focal stenosis. We applied Antegrade Wire Escalation technique, using ASAHI Astato XS 20 under the support of COOK CXI micro-catheter for wiring across LSFA CTO to P1 segment. To bypass the upcoming endoluminal covered stent at P1 segment, we intentionally wired through P1-P2 subintima with ASAHI Gladius MG14. Balloon angioplasty was done to crush the covered stent, but subsequent re-entry into the distal true lumen was challenging. Therefore, a TP trunk access was established for a retrograde approach. BOSTON V-18 wire was advanced along P2-P3 subintima using knuckle wire technique to kiss MG14 wire. After several attempts, we achieved anterograde re-entry into P3 segment, confirmed by tip injection, and advanced wire further into distal ATA. Both retrograde access and wire were removed with prolonged balloon inflation for hemostasis. Sequential stent deployment was performed with two Medtronic Resolute Onyx DES at proximal ATA, two Abbott Supera Stents from distal SFA to P3 segment to fully crush covered stent at P1 segment and one Boston Scientific Eluvia stent from proximal to middle SFA. Final angiography showed good distal runoff.
Case Summary
This 84-year-old male patient suffered from chronic limb-threatening ischemia, resulting from failed femoral-popliteal bypass graft with its distal covered stent across P1 segment involved. During endovascular therapy for LSFA-P1 CTO, intentional wiring through P1 subintima and subsequent balloon angioplasty and stenting to crush the covered stent was the key to rebuilding distal runoff. The patient’s wound infection was brought under control afterwards.