
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-169
A Case of LAD CTO With Negative Remodeling. Less Is More!
By Chun Yu Fung
Presenter
Chun Yu Fung
Authors
Chun Yu Fung1
Affiliation
Tuen Mun Hospital, Hong Kong, China1,
View Study Report
TCTAP C-169
Coronary - DES/BRS/DCB
A Case of LAD CTO With Negative Remodeling. Less Is More!
Chun Yu Fung1
Tuen Mun Hospital, Hong Kong, China1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A 69-year-old gentleman presented with inferoposterior STEMI
Primary PCI was activated.
Primary PCI was activated.
Relevant Test Results Prior to Catheterization
ECG on admission show STE over inferior and posterior leads with RV involvement
peak CK 4600
peak CK 4600
Relevant Catheterization Findings
stage PCI was arranged
L system was similar to PPCI findings
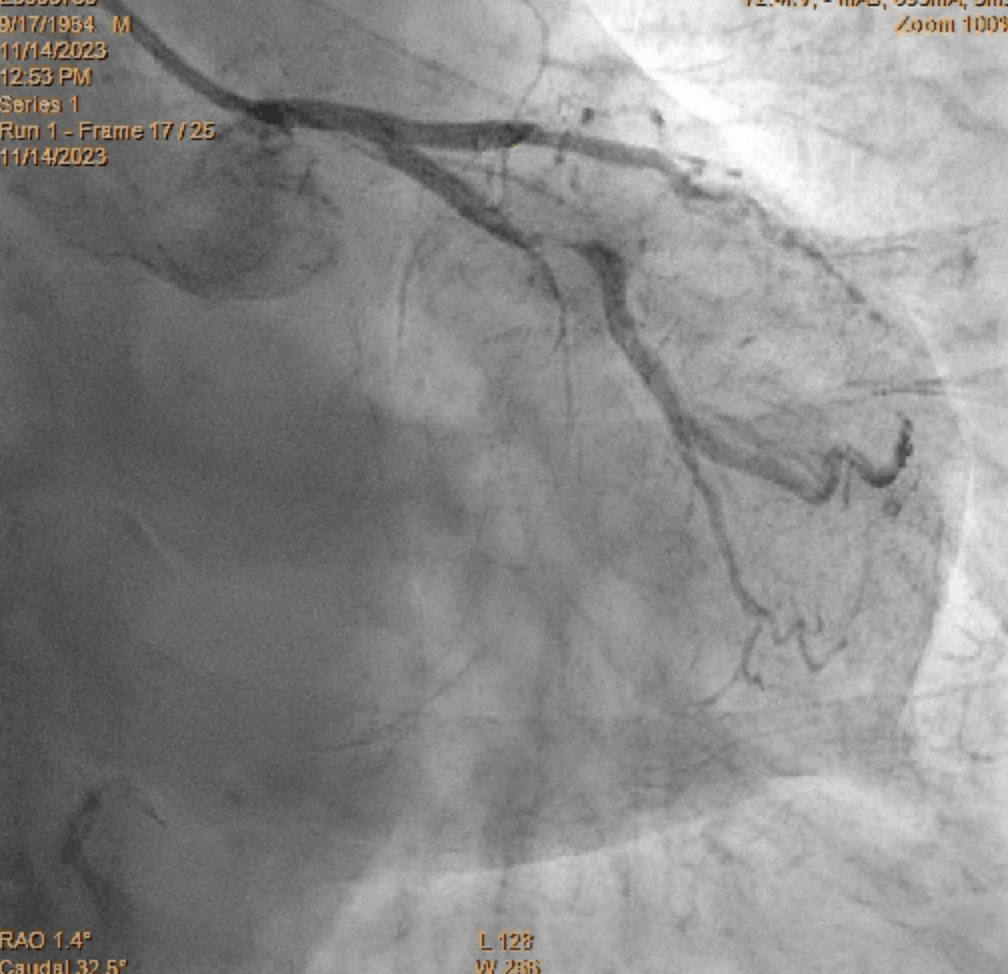
RCA: TIMI III flow, significant plaque at pRCA and dRCA
Interventional Management
Procedural Step
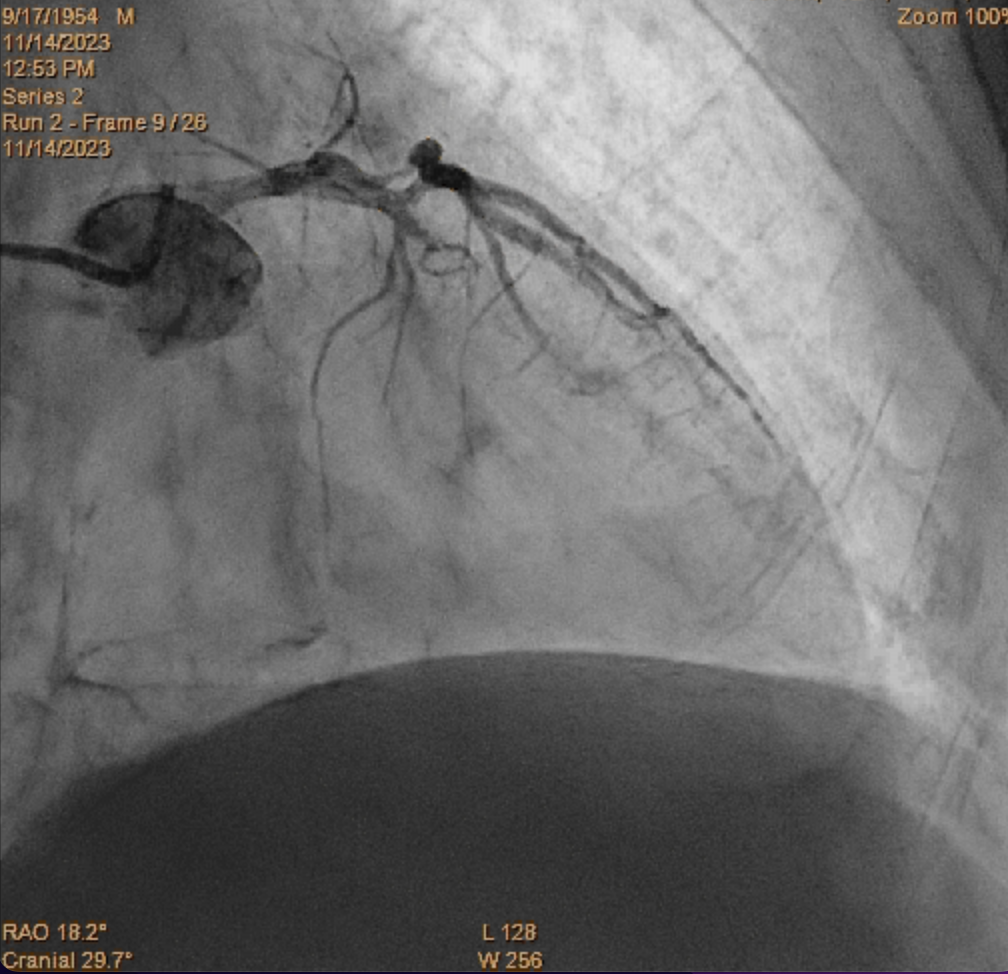
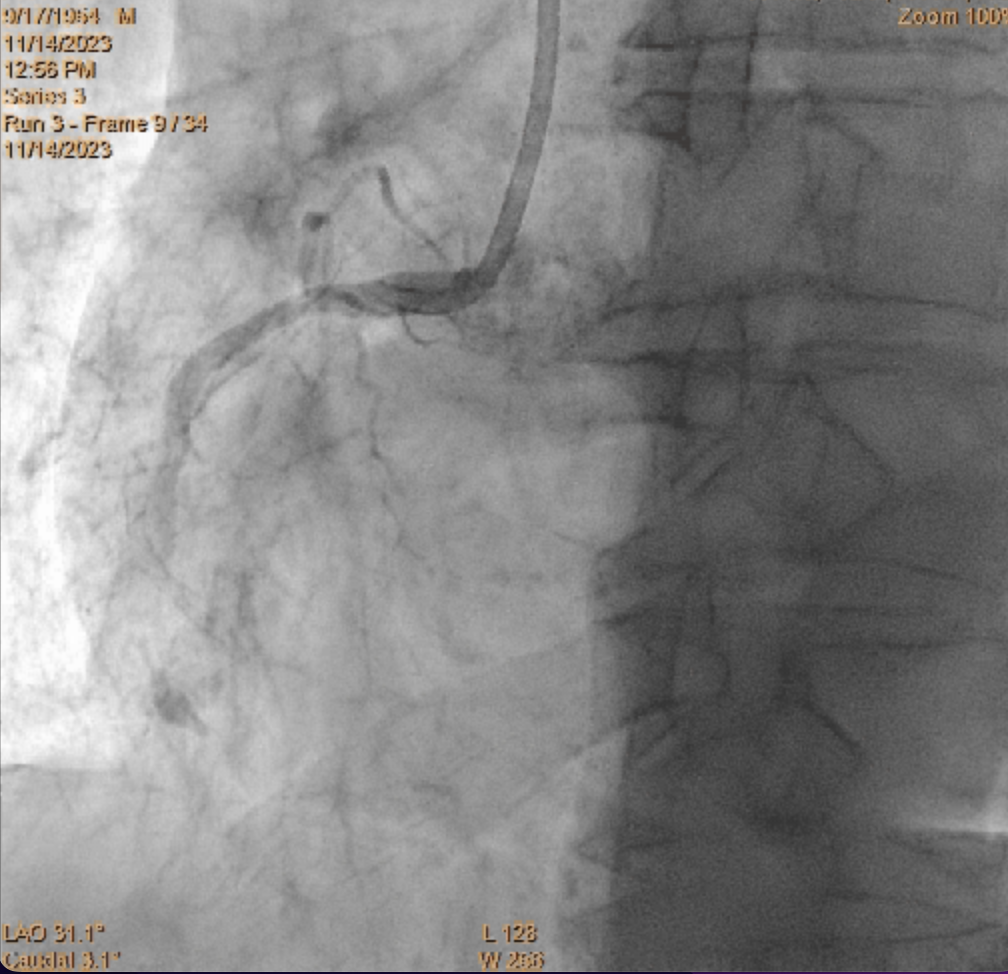
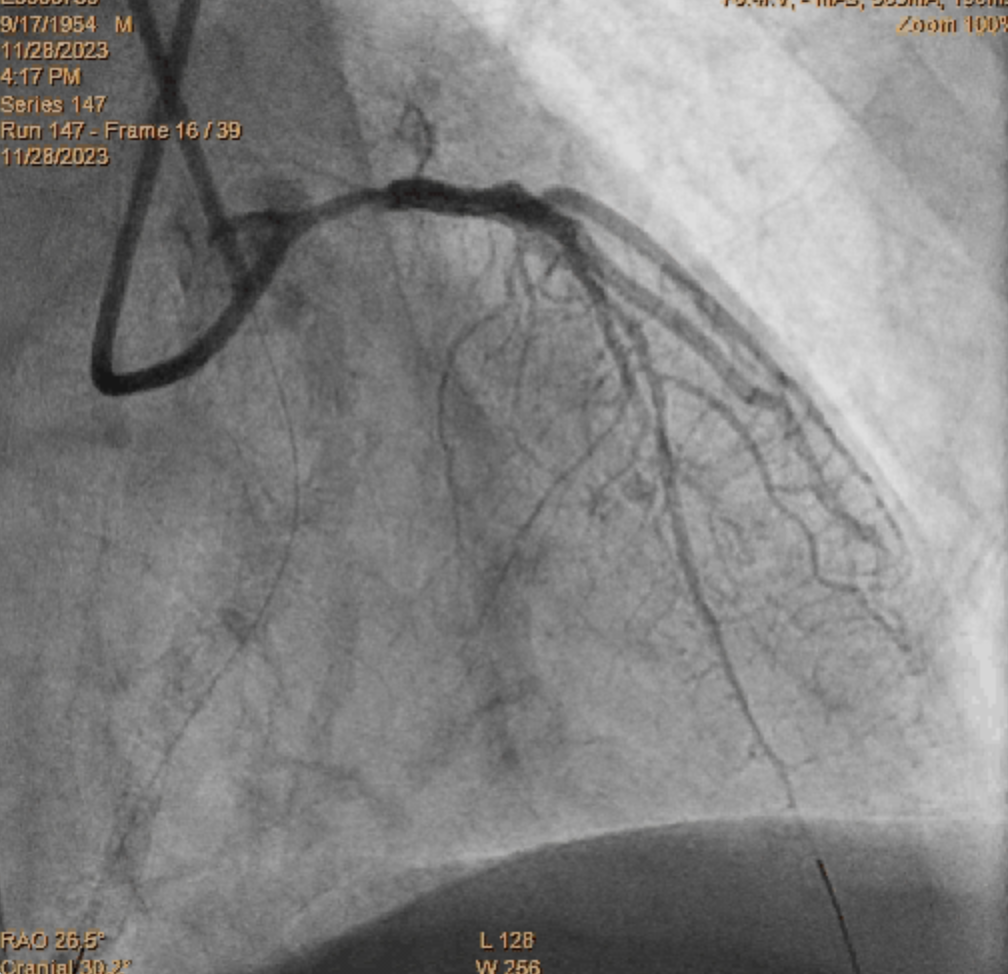
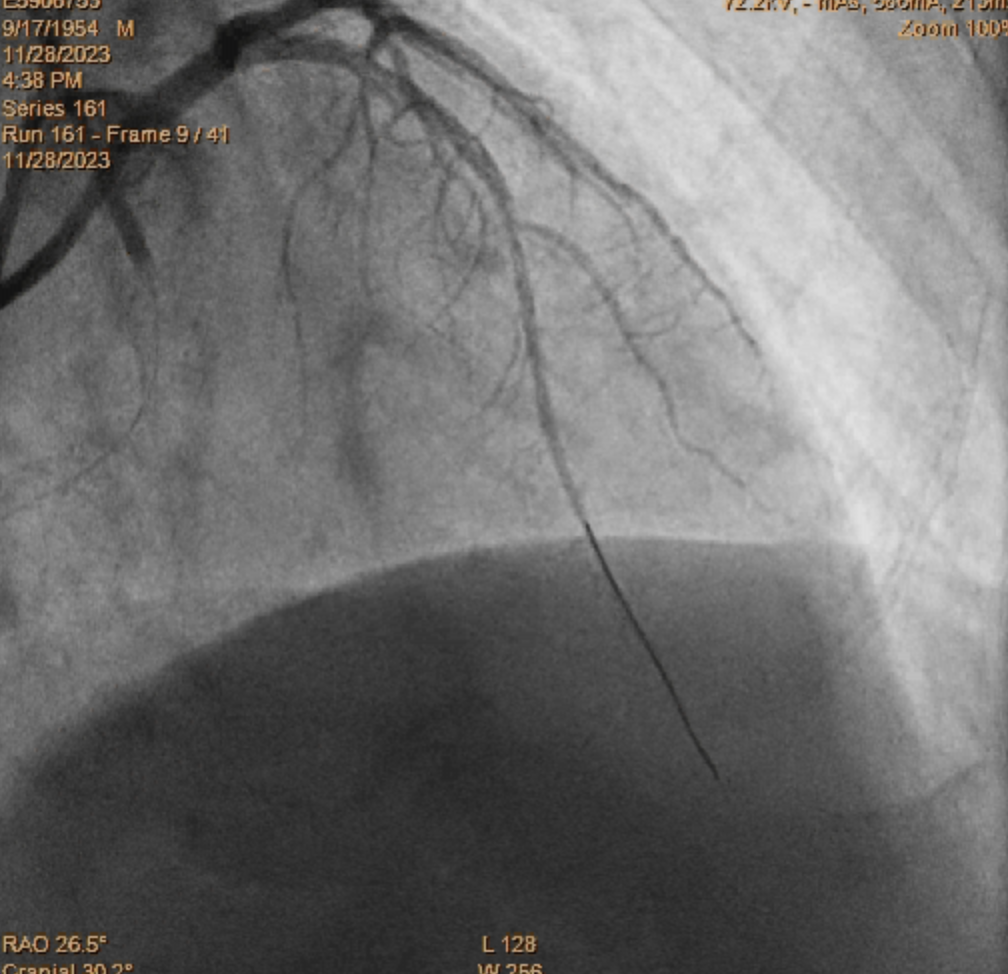
Stage PCI to RCA with JR4 6Fr GCIVUS: under-expansion of stent, significant plaque distal to stent. Another lesion in pRCA with heavy plaque burden and plaque rupture Lesion prepared with Raiden 4.0/15 and NSE 4.0/13
Consideration for stenting- small vessel size at distal landing, high risk of future ISR- potential positive remodeling in future and stent malapposition
Further prepare lesion with Scoreflex 2.5/15, Apollo 3.0/15
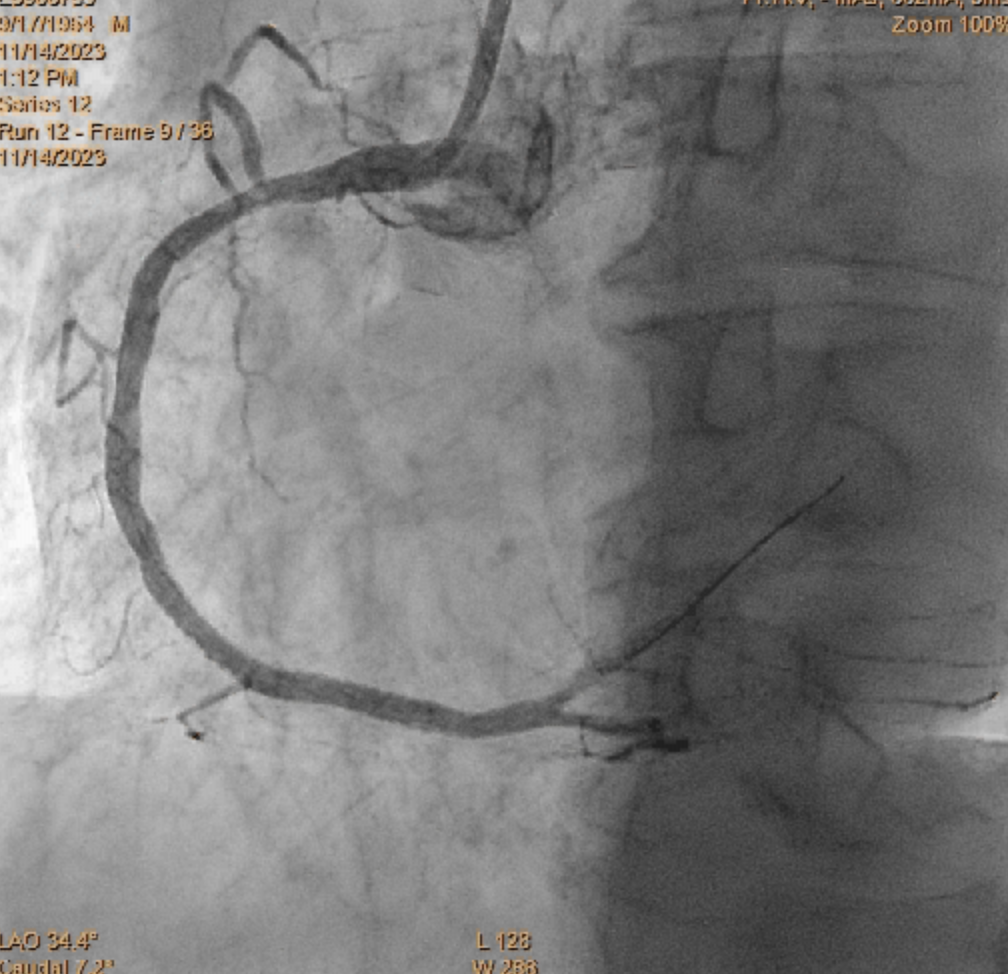
Restudy coro after 10 months:
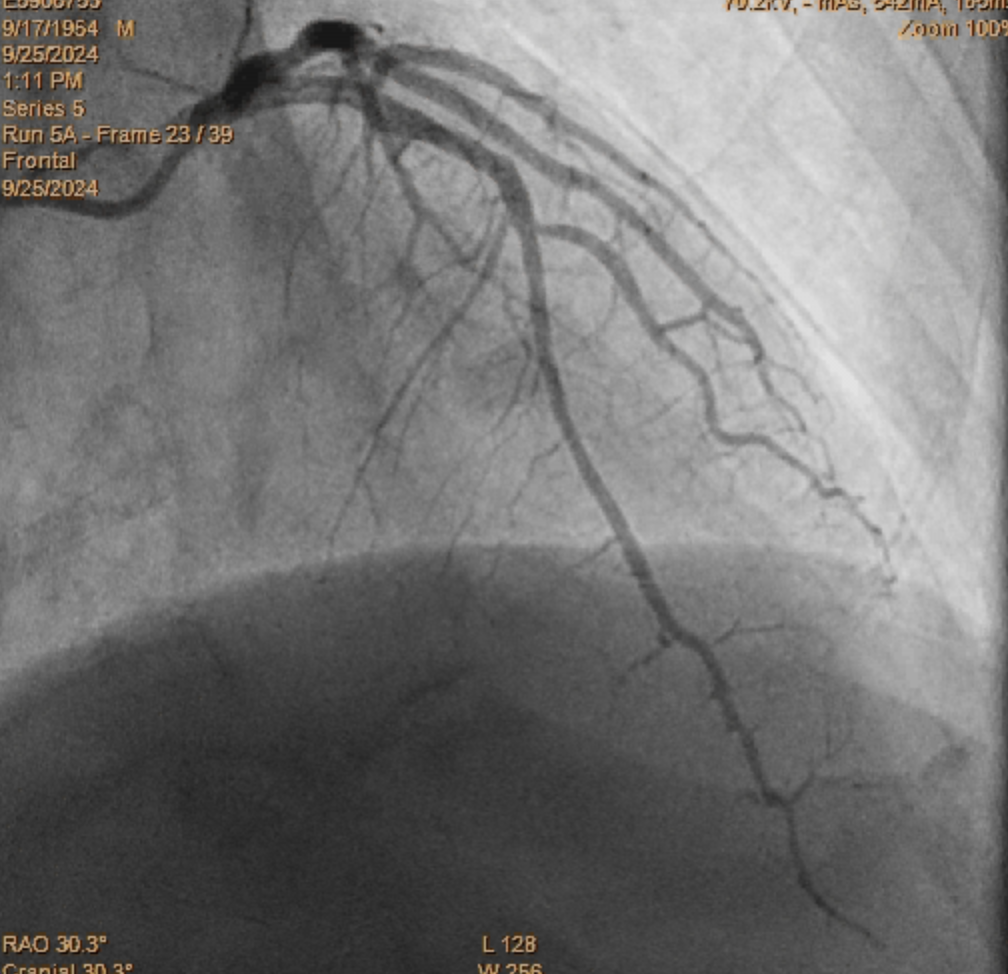
Consideration for stenting- small vessel size at distal landing, high risk of future ISR- potential positive remodeling in future and stent malapposition
Further prepare lesion with Scoreflex 2.5/15, Apollo 3.0/15
Restudy coro after 10 months:
Case Summary
Although the recent REC-CAGEFREE I trial show that drug eluting balloon (DEB) fail to achieve non-inferiority compared with drug eluting stenting (DES) for de novo, non-complex coronary artery disease. DEB still have a role in treating specific condition, such as lesion in small vessels. Our case demonstrate that DEB is useful for CTO lesion with distal vessel negative remodelling. Had a undersized DES been deployed in our case, the risk of stent thrombosis and restenosis will be high. Our case also demonstrate that minor type B dissection after DEB can be managed conservatively, healing is possible and no stenting is needed if TIMI III flow is preserved.