
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-155
Twists and Turns: Unraveling Spiral Coronary Dissection and Catheter Kinking in Diagnostic Angiography
By Verry Gunawan Sohan, Amir Aziz Alkatiri, Doni Firman, Arwin Saleh Mangkuanom, Nanda Iryuza
Presenter
Verry Gunawan Sohan
Authors
Verry Gunawan Sohan1, Amir Aziz Alkatiri1, Doni Firman1, Arwin Saleh Mangkuanom1, Nanda Iryuza1
Affiliation
National Cardiovascular Center, Indonesia1,
View Study Report
TCTAP C-155
Coronary - Complication Management
Twists and Turns: Unraveling Spiral Coronary Dissection and Catheter Kinking in Diagnostic Angiography
Verry Gunawan Sohan1, Amir Aziz Alkatiri1, Doni Firman1, Arwin Saleh Mangkuanom1, Nanda Iryuza1
National Cardiovascular Center, Indonesia1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A 71 year old male presented with worsening shortness of breath with strenuous activity. Vital signs were within normal limits. Physical examination revealed a grade 4 pansystolic murmur at the left lower sternal border. The patient was scheduled for routine cardiac catheterization prior to mitral valve replacement due to severe mitral regurgitation.
Relevant Test Results Prior to Catheterization
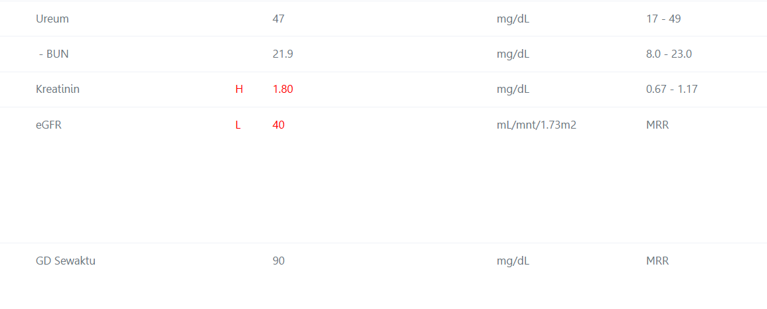
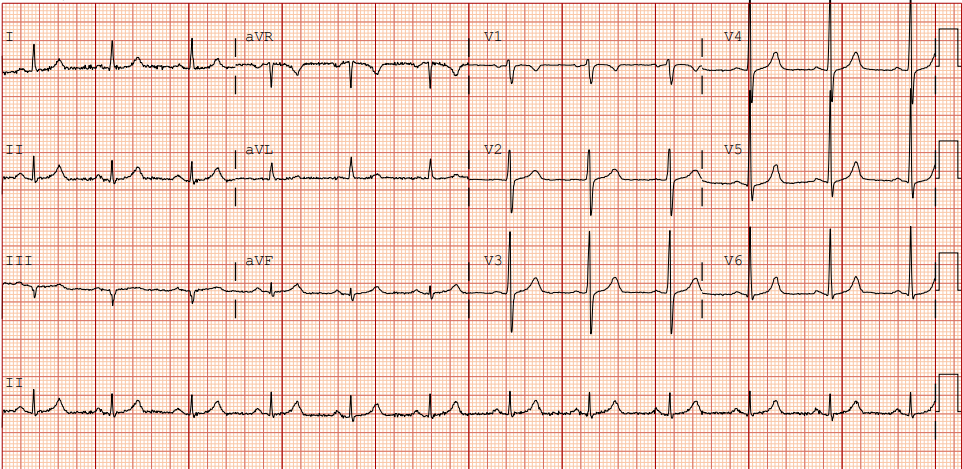
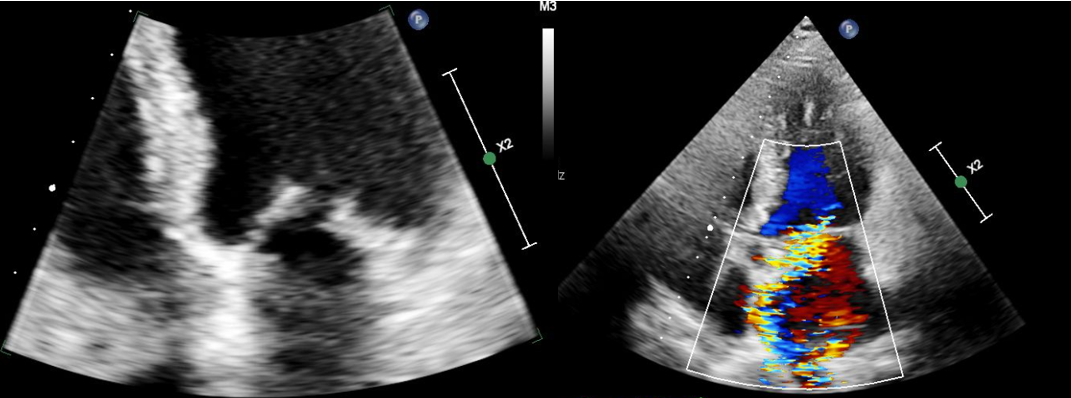
Electrocardiogram before catheterization showed normal sinus rhythm. Echocardiography revealed severe mitral regurgitation with left ventricular dilation, and normal left ventricular systolic function (LVEF 67%). Laboratory results indicated decreased kidney function (eGFR 40 ml/min), while other lab values were within normal limit.
Relevant Catheterization Findings
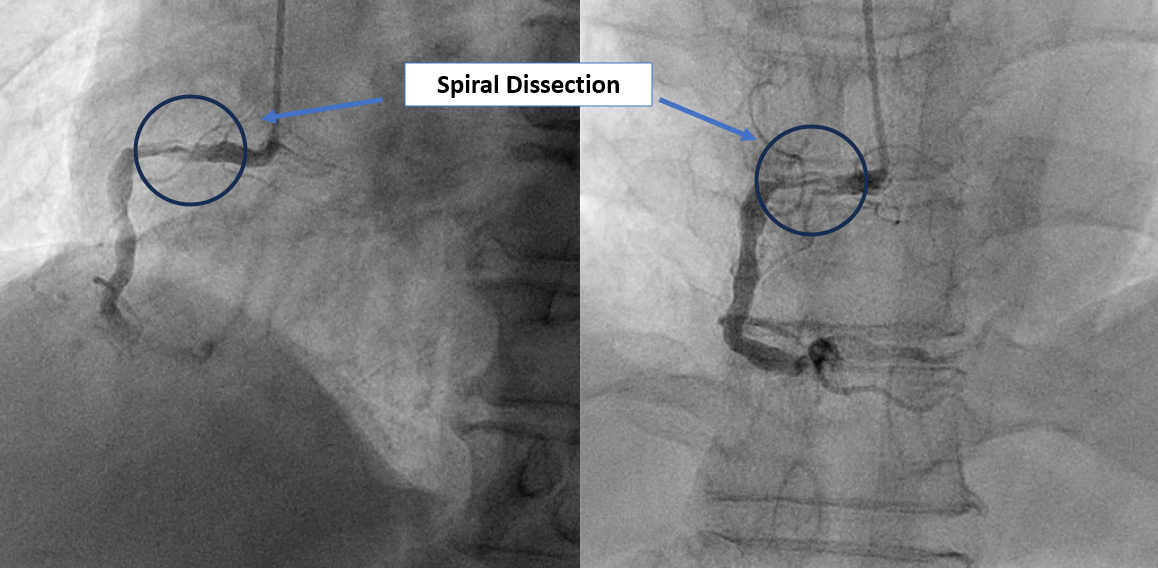
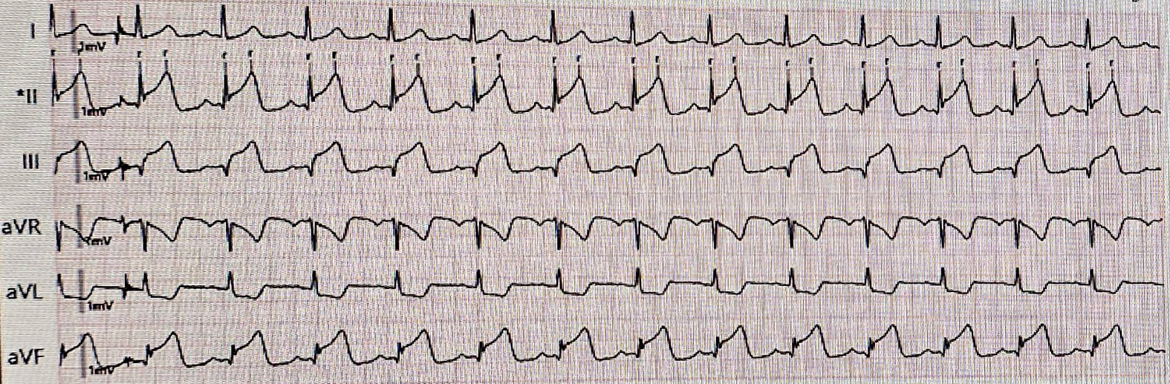
During RCA canulation, the patient complained of chest pain with blood pressure 70/40 mmHg. The ECG monitor displayed peaked ST segment elevation in leads II, III, and aVF. Diagnostic angiography revealed spiral coronary arterial dissection at the proximal RCA with TIMI 1 Flow to distal RCA.
Interventional Management
Procedural Step
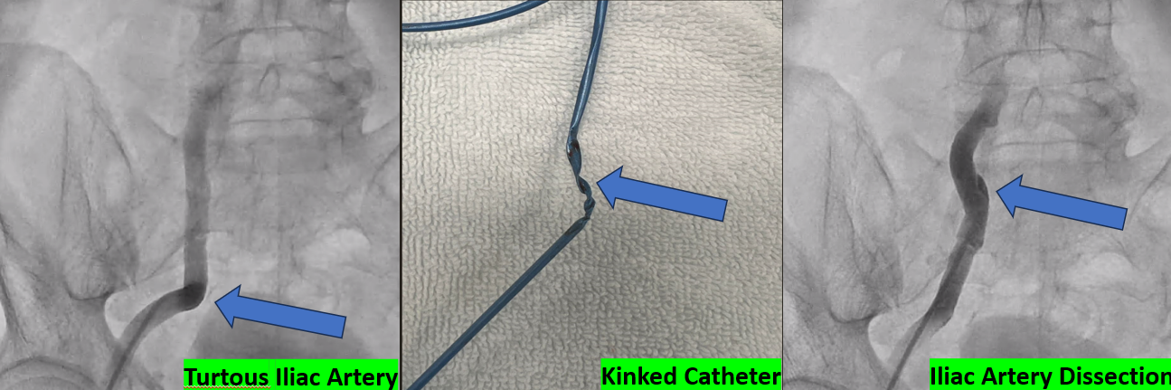
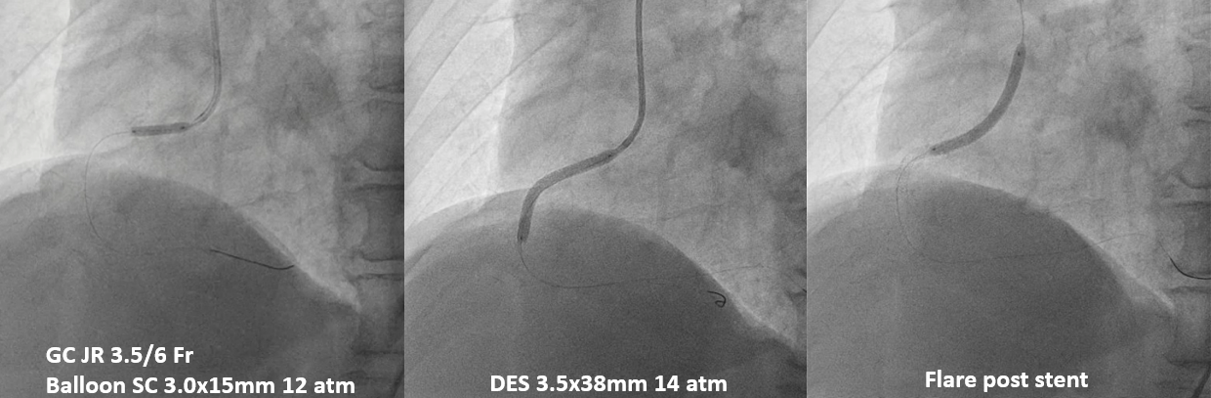
The patient had a periprocedural acute inferior STEMI and was promptly opted for primary percutaneous coronary intervention. Radial access was not feasible due to radial artery occlusion caused by severe spasm. Right femoral artery access was challenging because of tortuosity. Rapid manipulation of the guiding catheter caused a difficult to release kinked catheter that eventually leading to the catheter being forcefully removed and resulted in a dissection of the right iliac artery. Consequently, access was shifted to the left femoral artery. Cannulation was performed with JR3.5/ 6 Fr guiding catheter. The lesion was successfully crossed with workhorse wire to the distal RCA. A pre-dilation was performed with 3.0 x 15 mm semi compliant (SC) balloon at the proximal RCA, thus immediately restore the flow. A 3.5 x 38 mm Drug-eluting stent (DES) was deployed at 14 atm. Post dilatation was performed with the same balloon up to 16 atm. The chest pain subsided, and the final angiography revealed TIMI 3 flow, with no residual stenosis or dissection.

Case Summary
Iatrogenic spiral coronary artery dissection, particularly during diagnostic angiography, is a rare but serious complication that can lead to myocardial ischemia or infarction. Although catheter-induced dissections occur in less than 0.2% of cases, they pose significant risks, including compromised coronary blood flow. Careful catheter manipulation is crucial; excessive twisting can lead to kinking and subsequent dissection. Proper pre-procedural assessment and skilled techniques are essential to mitigate these risks. Awareness of potential complications is vital for improving patient outcomes during angiographic procedures.