
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-032
Shock the Rock
By Swee En Goay, David, Tat Wei Yong, Chee Kiang Teoh
Presenter
Swee En Goay
Authors
Swee En Goay1, David, Tat Wei Yong1, Chee Kiang Teoh1
Affiliation
National Heart Institute, Malaysia1,
View Study Report
TCTAP C-032
Coronary - Adjunctive Procedures (Thrombectomy, Atherectomy, Special Balloons)
Shock the Rock
Swee En Goay1, David, Tat Wei Yong1, Chee Kiang Teoh1
National Heart Institute, Malaysia1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
66 years old gentleman presented with worsening chest pain with exertional dyspnea for 1 week. He has Hypertension, Chronic Kidney Disease and Coronary Artery Disease with Angioplasty to Left Anterior Descending artery in 2013. He described the current chest discomfort as heavy in nature and increased in frequency over last 1 week. It worsened with exertion, limiting his activities of daily living. Physical examination was unremarkable with Heart rate 64bpm, Blood pressure 123/76mmHg.

Relevant Test Results Prior to Catheterization
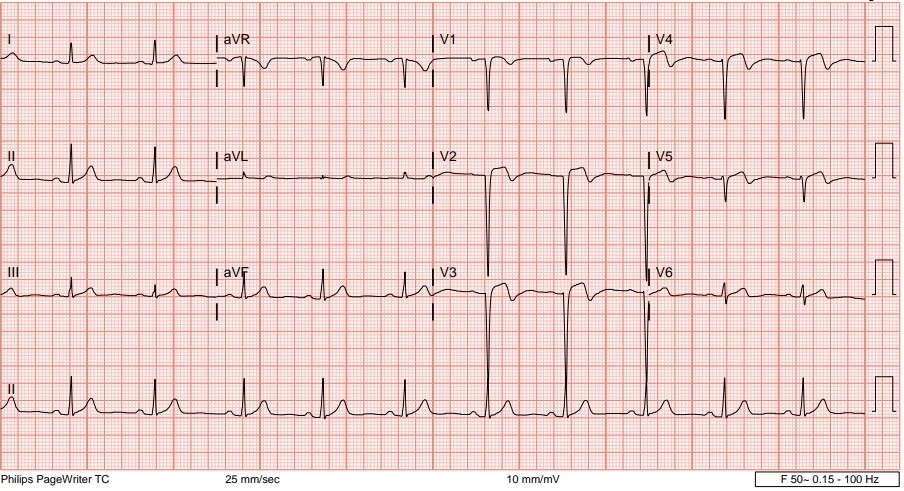
ECG showed Sinus rhythm, biphasic T V2-V5, Troponin T was raised at 470ng/ml. His creatinine measured 195 with an eGFR of 30ml/min/1.73m2. ECHO showed ejection fraction of 57% with normal valves. He was treated for Non-ST Elevation Myocardial Infarction (NSTEMI) and underwent coronary angiogram.
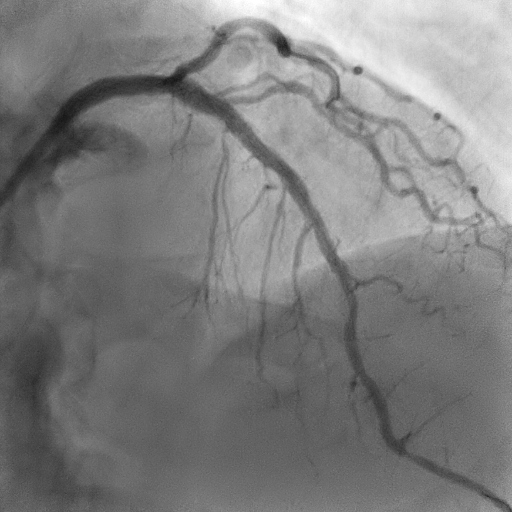
Relevant Catheterization Findings
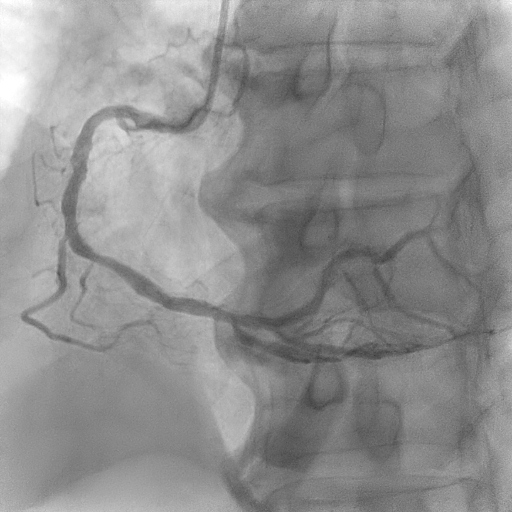
Coronary angiogram showed severe calcified lesion at proximal Left anterior descending (LAD) with patent mid LAD stent. There is mild disease over proximal Left circumflex (LCx) &moderate lesion over mid Right coronary artery (RCA).


Interventional Management
Procedural Step
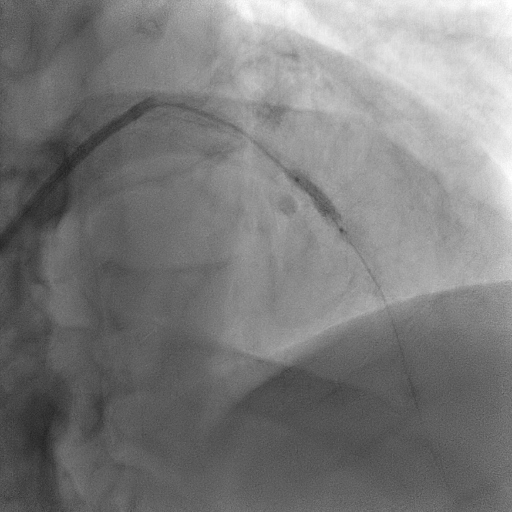
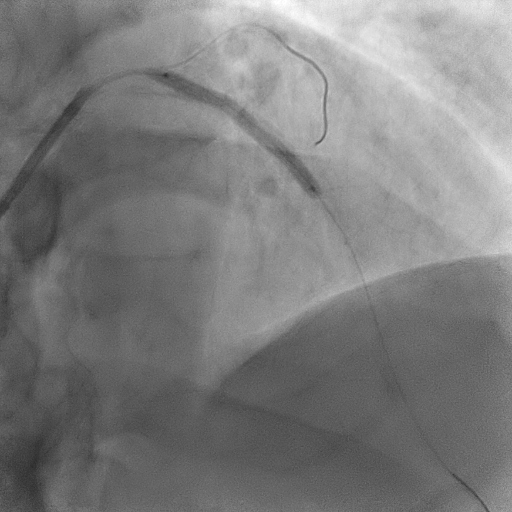
We proceeded with Percutaneous Coronary Intervention to LAD using EBU 3.5/6Fr as guiding catheter. After crossing the LAD lesion using Run through floppy workhorse wire, we did an Intravascular Ultrasound (IVUS) study which showed a concentric calcified lesion proximal to mid LAD with a patent mid LAD stent. Intravascular lithotripsy (IVL) SHOCKWAVE 3.0/12mm was delivered for 12 cycles before further predilated the calcified lesion with WEDGE NC 3.5/15mm up to 14 atm. After adequate lesion preparation, we stented the proximal LAD lesion with ORSIRO 3.0/35mm at 10 atm overlapping with the previous mid LAD stent before further post dilatation with NC EMERGE 3.5/15mm up to 16 atm.Final IVUS study showed a well opposed stent with no dissection.Patient was discharged home well the next day and remain well during his clinic review.
Case Summary
Coronary artery calcification represents one of the challenging and demanding subsets of percutaneous coronary intervention. Intravascular lithotripsy (IVL) is a novel approach to lesion preparation of severely calcified plaques in coronary vessels. It emits circumferential mechanical energy and disrupts the calcium, minimizes soft-tissue injury while aiding stent deployment. It is relatively simple to perform, safe and effective in facilitating stent implantation and expansion in severely calcified lesions while significantly reducing the risk of complications to make procedures more predictable and efficient.