
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-131
The Peril of Coronary Perforation in Acute STEMI
By Dena Karina Firmansyah, Dafsah Arifa Juzar, Nanda Iryuza, Arwin Saleh Mangkuanom, Amir Aziz Alkatiri, Doni Firman
Presenter
Dena Karina Firmansyah
Authors
Dena Karina Firmansyah1, Dafsah Arifa Juzar1, Nanda Iryuza1, Arwin Saleh Mangkuanom1, Amir Aziz Alkatiri1, Doni Firman1
Affiliation
National Cardiovascular Center, Indonesia1,
View Study Report
TCTAP C-131
Coronary - Complication Management
The Peril of Coronary Perforation in Acute STEMI
Dena Karina Firmansyah1, Dafsah Arifa Juzar1, Nanda Iryuza1, Arwin Saleh Mangkuanom1, Amir Aziz Alkatiri1, Doni Firman1
National Cardiovascular Center, Indonesia1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A 65 years old female was presented with 3 days onset Inferior ST-elevation Myocardial Infarction (STEMI). She had persistent angina despite optimal medical therapy. The patient had episode of Supraventricular Tachycardia (SVT) that was managed by intravenous Amiodarone. The vital signs were stable without support, the physical examination were unremarkable. The patient was assigned for early invasive strategy.
Relevant Test Results Prior to Catheterization
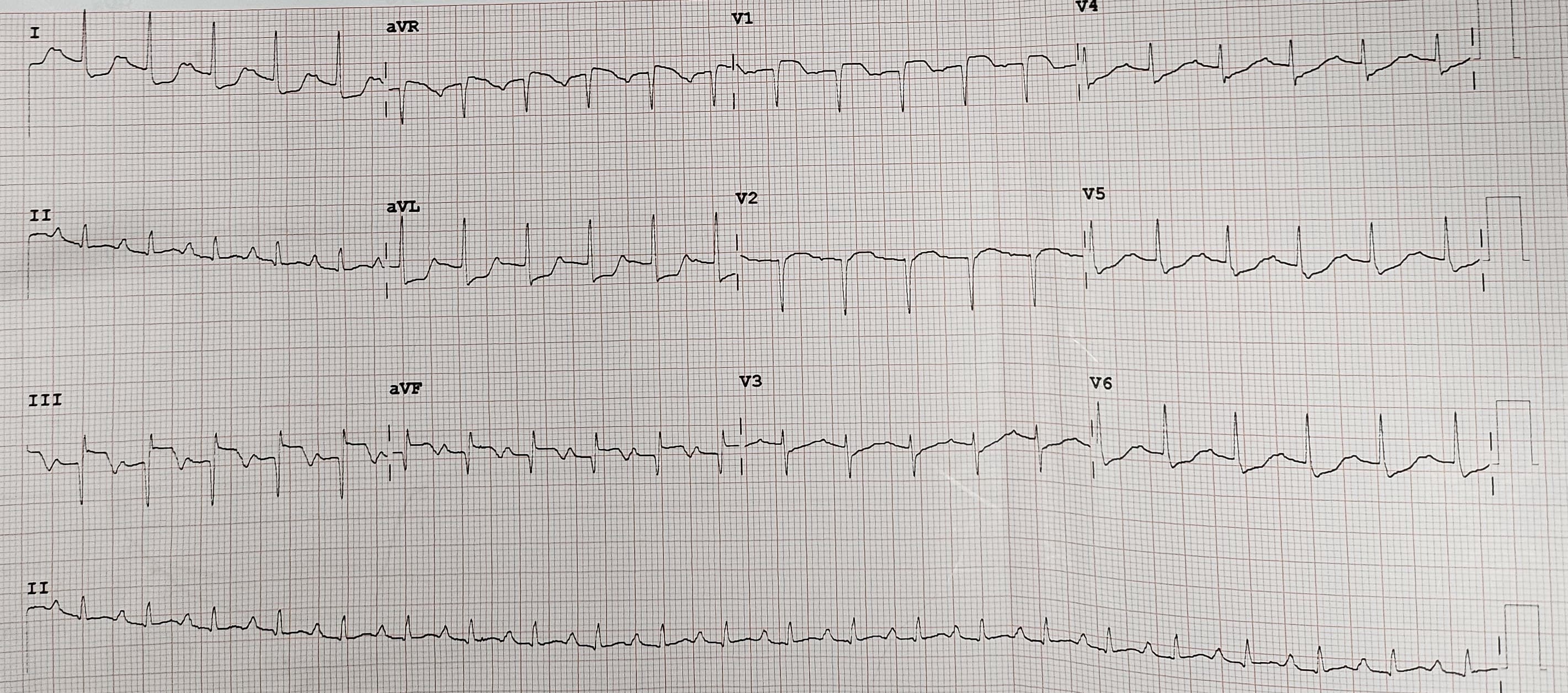
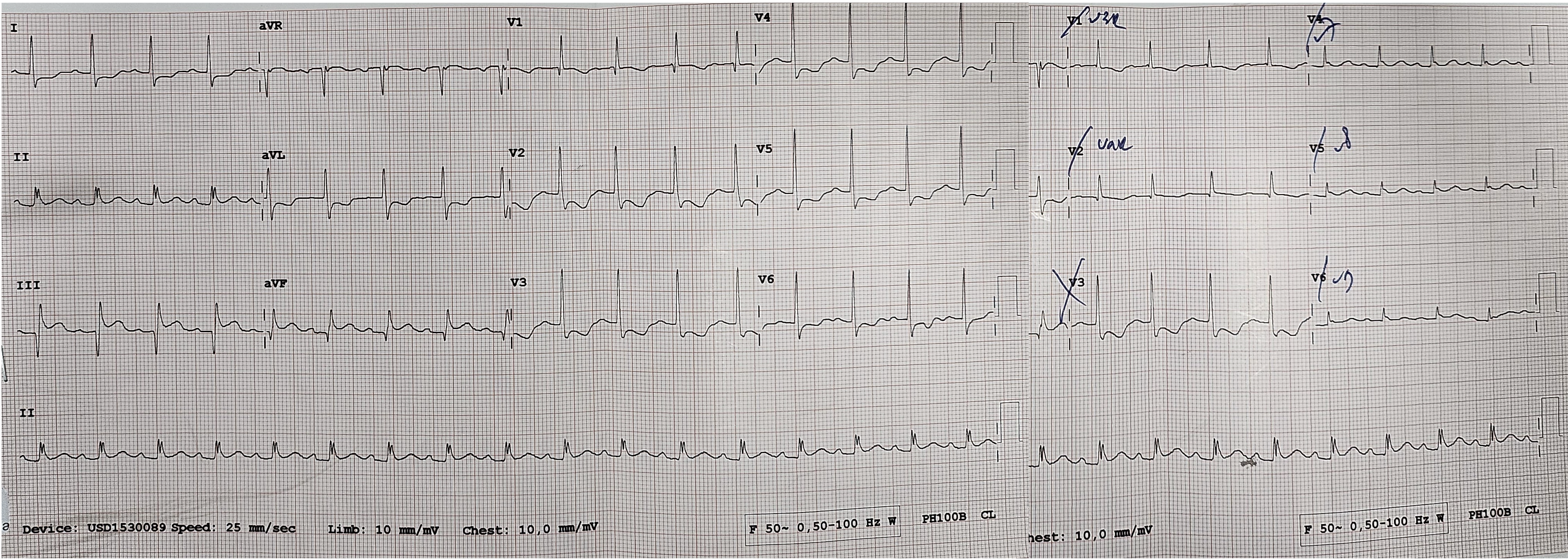
The electrocardiogram prior to catheterization procedure revealed sinus tachycardia with persistent ST-elevation and Q wave at lead III and AVF, ST depression at V4-V6, I, AVL. Echocardiography demonstrated good left ventricular function (LV EF 56%), reduced right ventricular function, global normokinetic and mild tricuspid regurgitation. Laboratory test result were unremarkable.
Relevant Catheterization Findings
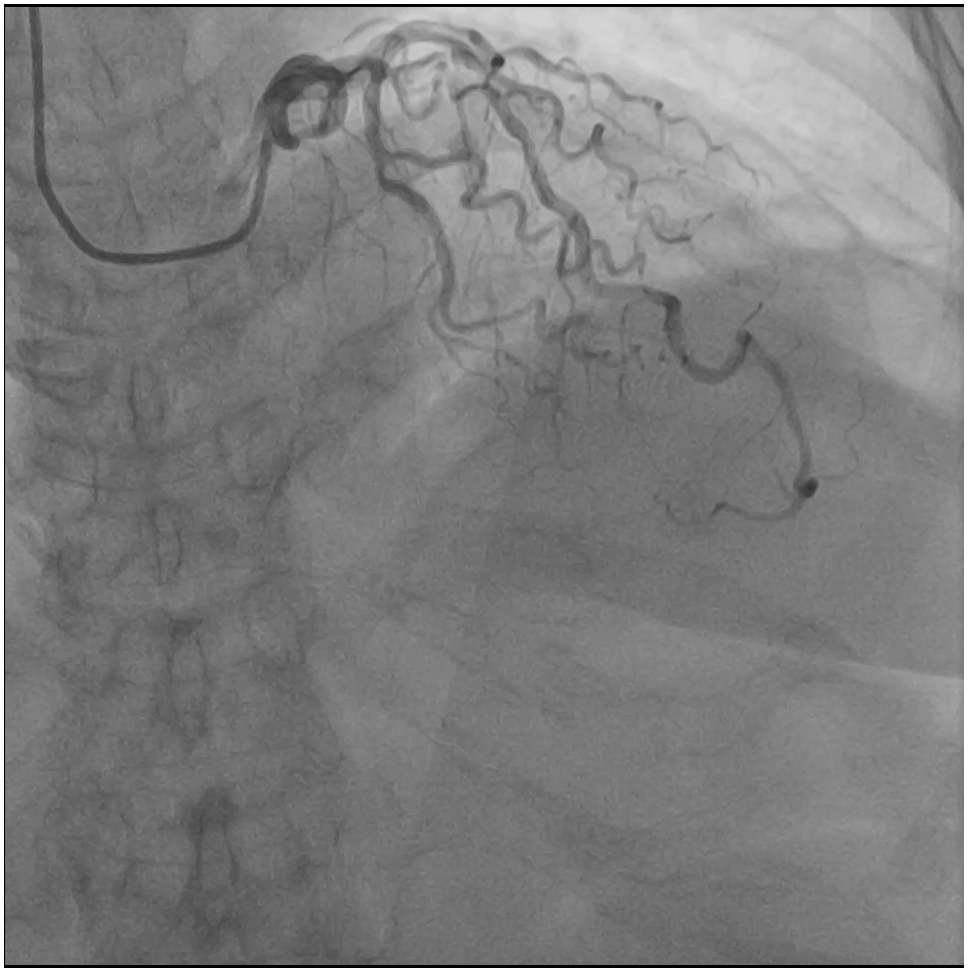
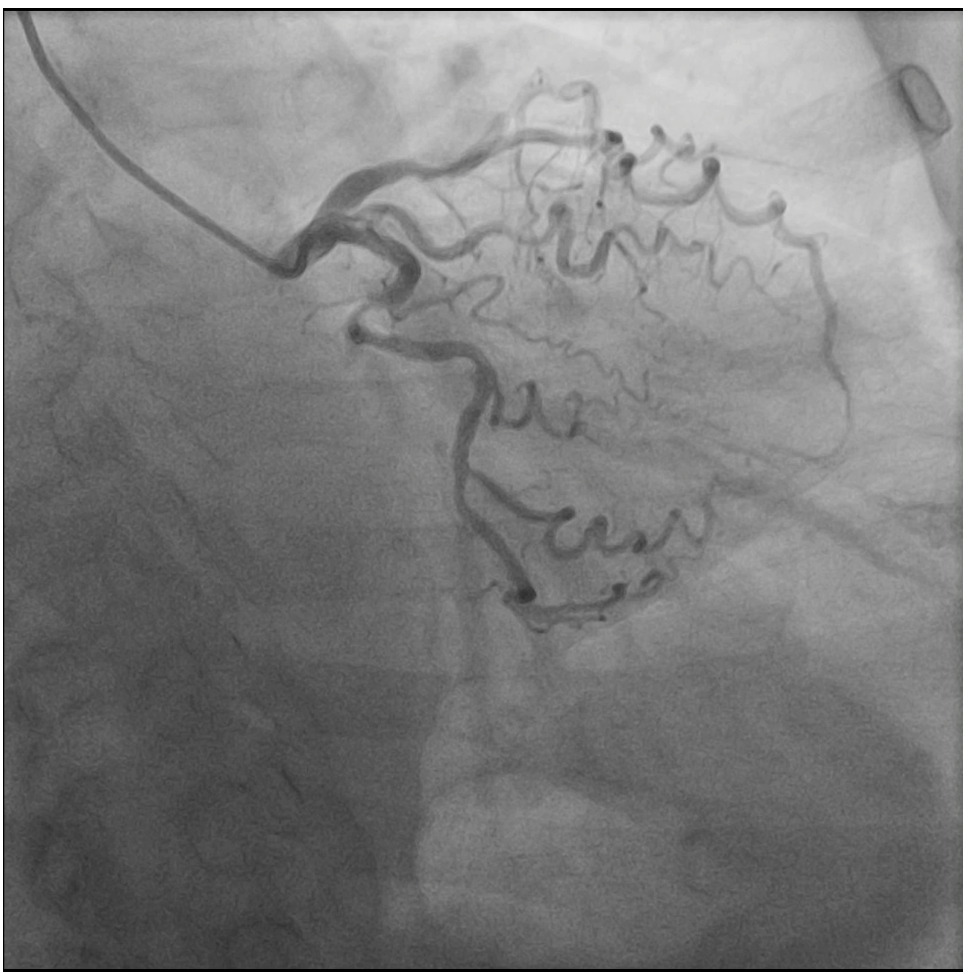
The diagnostic angiography demonstrated a severely tortuous coronary vessels, moderate lesion at LAD and LCX, total occlusion at proximal RCA with no traces of collaterals from the ipsilateral or contralateral circulations.
Interventional Management
Procedural Step
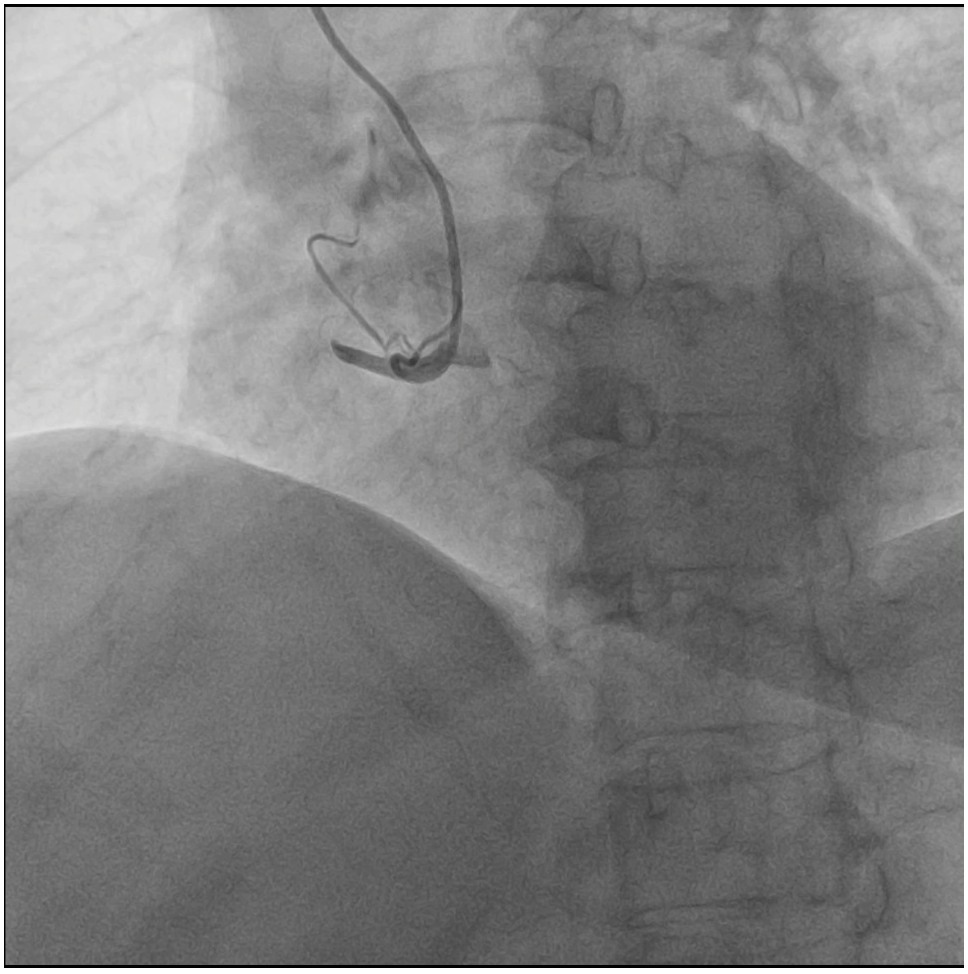
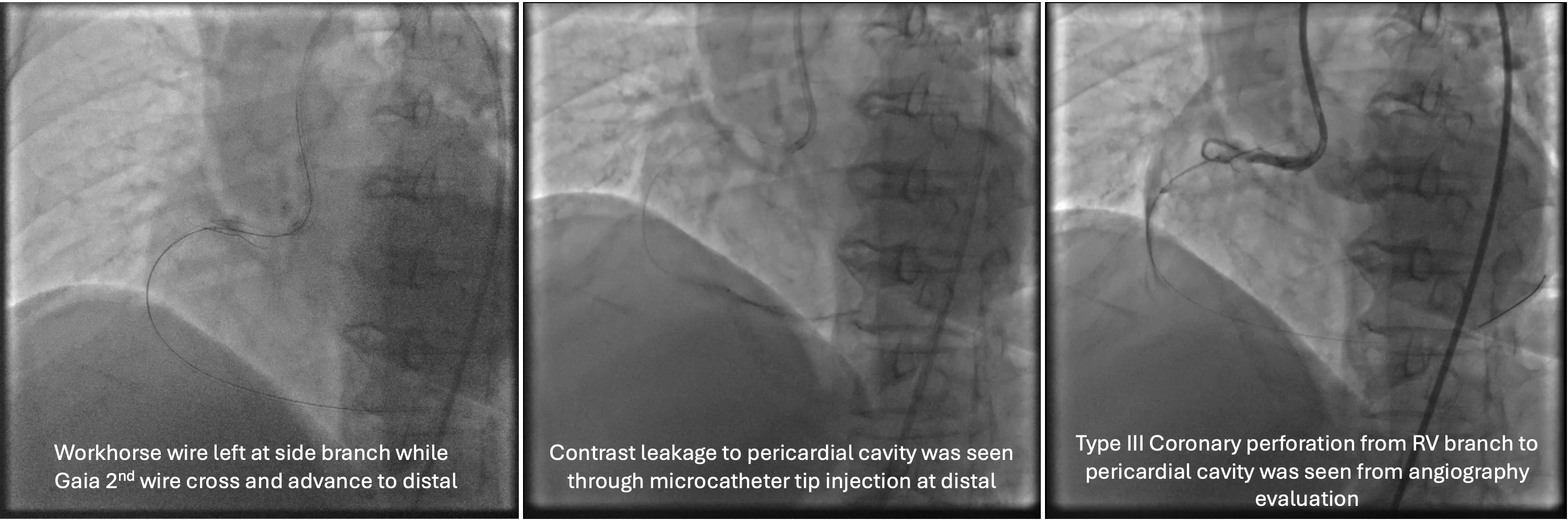
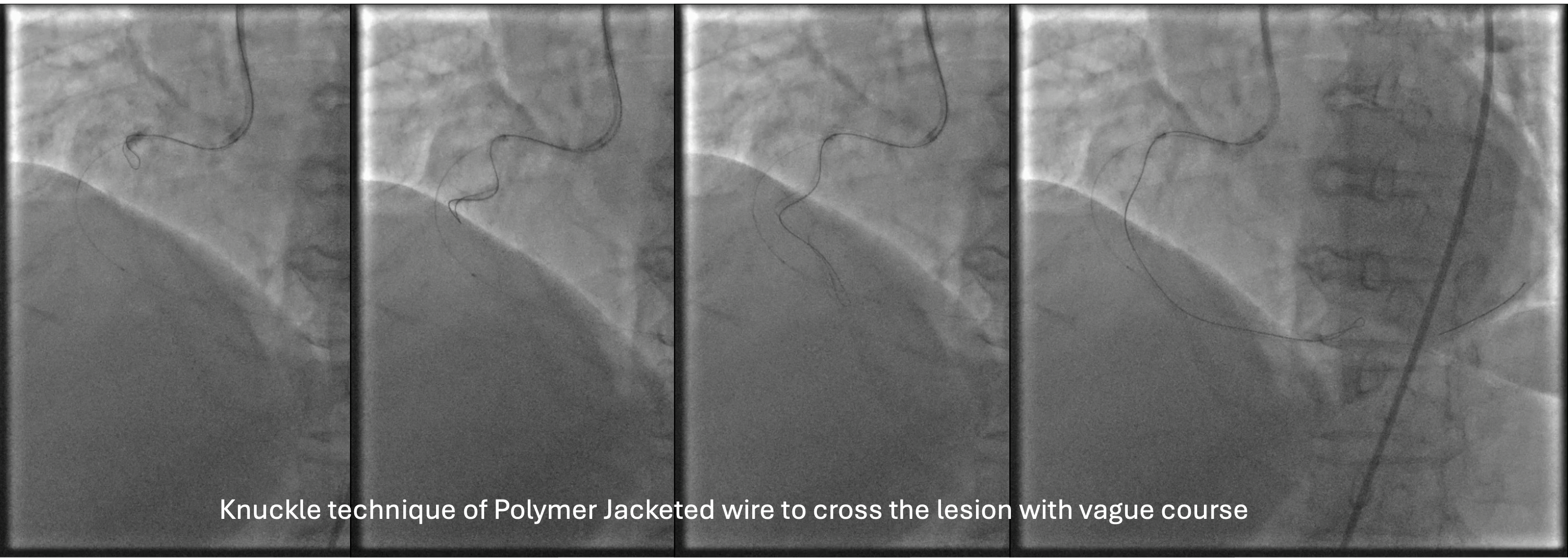
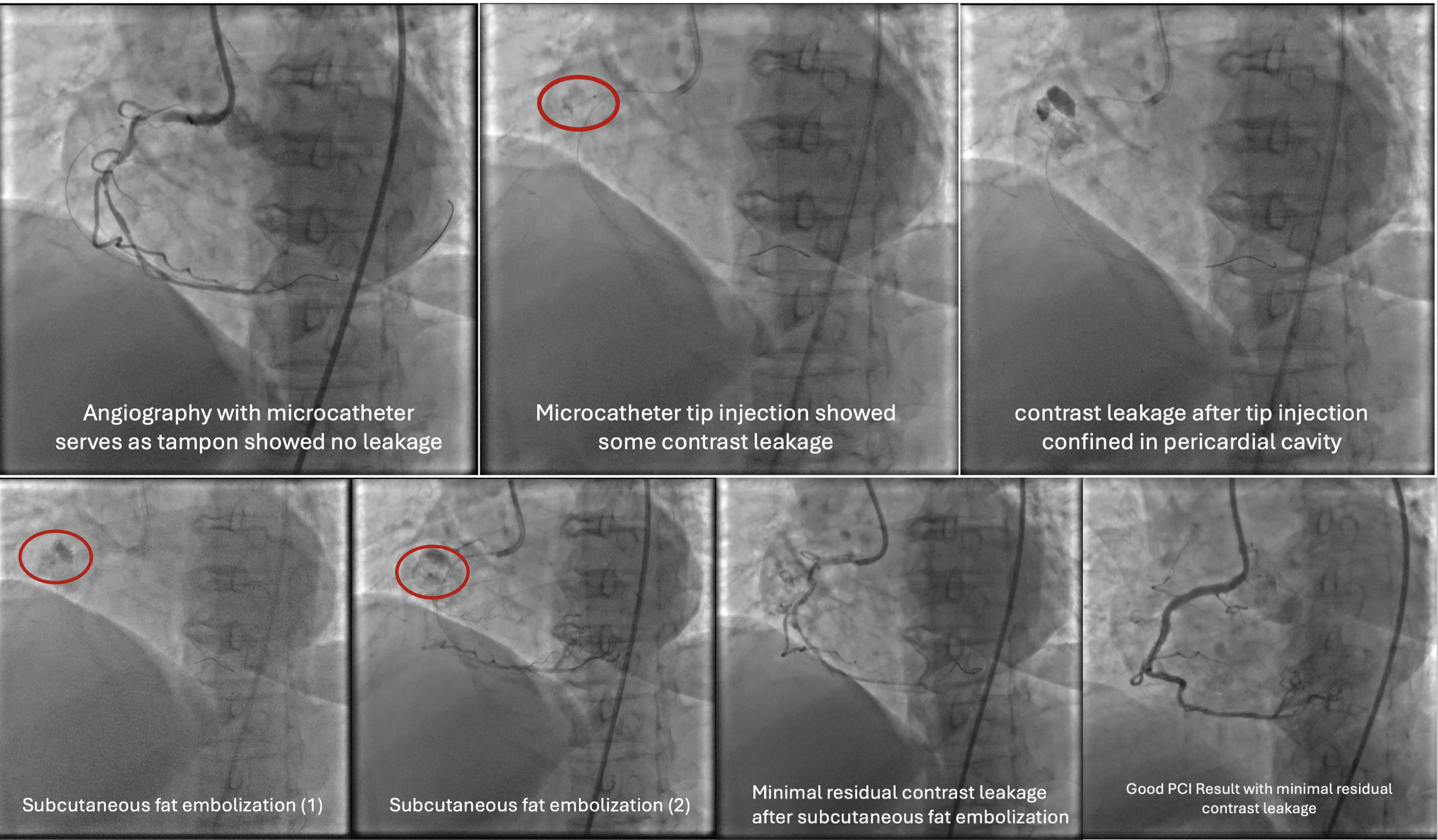
Several attempts to cross the lesion with workhorse wire and polymer jacketed wire with microcatheter support were failed because the wire went into small branch proximal to the occlusion. Guide catheter AL 0.75/7F was exchanged for JR 3.5/7F because of frequent pressure damping associated with deep engagement. Workhorse wire was left at the small branch while the second stiff wire was attempted to cross. The stiff wire (Gaia 2nd wire) and microcatheter was successfully cross and advanced to the distal. Microcatheter tip injection revealed contrast leakage to pericardial cavity. The stiff wire was exchanged for less traumatic workhorse wire and microcatheter was left to tampon the coronary perforation. Due to vague course of the vessel, rewiring to RCA was done with polymer jacketed wire in knuckle technique that eventually succeeded to cross the lesion and enter the true lumen. Pre-dilatation with semi-compliant balloon 2.5x15 mm at proximal-mid RCA was done to restore the flow. Angiography revealed tortuous and calcified RCA with some contrast leakage confined to pericardium. Subcutaneous fat embolization was attempted several times to seal the perforation. With minimal residual leakage, pre-dilatation with non-compliant balloon 3.0x18 mm was proceeded. Stent DES 3.0x38 mm was implanted at the proximal-mid RCA with the aid of 6F guide extension catheter. Angiography evaluation demonstrated good PCI result leaving only minimal residual contrast leakage confined to pericardium.
Case Summary
When the vessel course is unclear, avoid using stiff wire. Second wire might be used as parallel wire while the other cross the lesion. In case of coronary perforation, prompt identification and appropriate management strategy is mandatory. Microcatheter tamponade of perforation and subcutaneous fat embolization may serve as appropriate strategy to manage vessel perforation.