
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-123
Overcoming a Rare Encounter: The Cheese Strategy in Giant Coronary Aneurysm Intervention With Ostial Disease
By I Dewa Gde Dwi Sumajaya, Liew Houng Bang, Rustem Dautov
Presenter
I Dewa Gde Dwi Sumajaya
Authors
I Dewa Gde Dwi Sumajaya1, Liew Houng Bang2, Rustem Dautov3
Affiliation
Bali International Hospital, Indonesia1, Queen Elizabeth Hospital II, Malaysia2, Prince Charles Hospital, Australia3,
View Study Report
TCTAP C-123
Coronary - Complex PCI - Multi-Vessel Disease
Overcoming a Rare Encounter: The Cheese Strategy in Giant Coronary Aneurysm Intervention With Ostial Disease
I Dewa Gde Dwi Sumajaya1, Liew Houng Bang2, Rustem Dautov3
Bali International Hospital, Indonesia1, Queen Elizabeth Hospital II, Malaysia2, Prince Charles Hospital, Australia3,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A 71-year-old man came to the cardiology clinic with a history of intermittent typical angina in the last 2 years. Symptoms were appearing, especially when he did a brisk walk or climbed up stairs. Another symptom, like leg swelling, palpitation, and syncope, was denied. He had underlying type 2 diabetes mellitus, hypertension, and dyslipidaemia. He is a former smoker and denied consuming alcohol. He is independent in daily living. Physical examination shows within the normal limit.
Relevant Test Results Prior to Catheterization
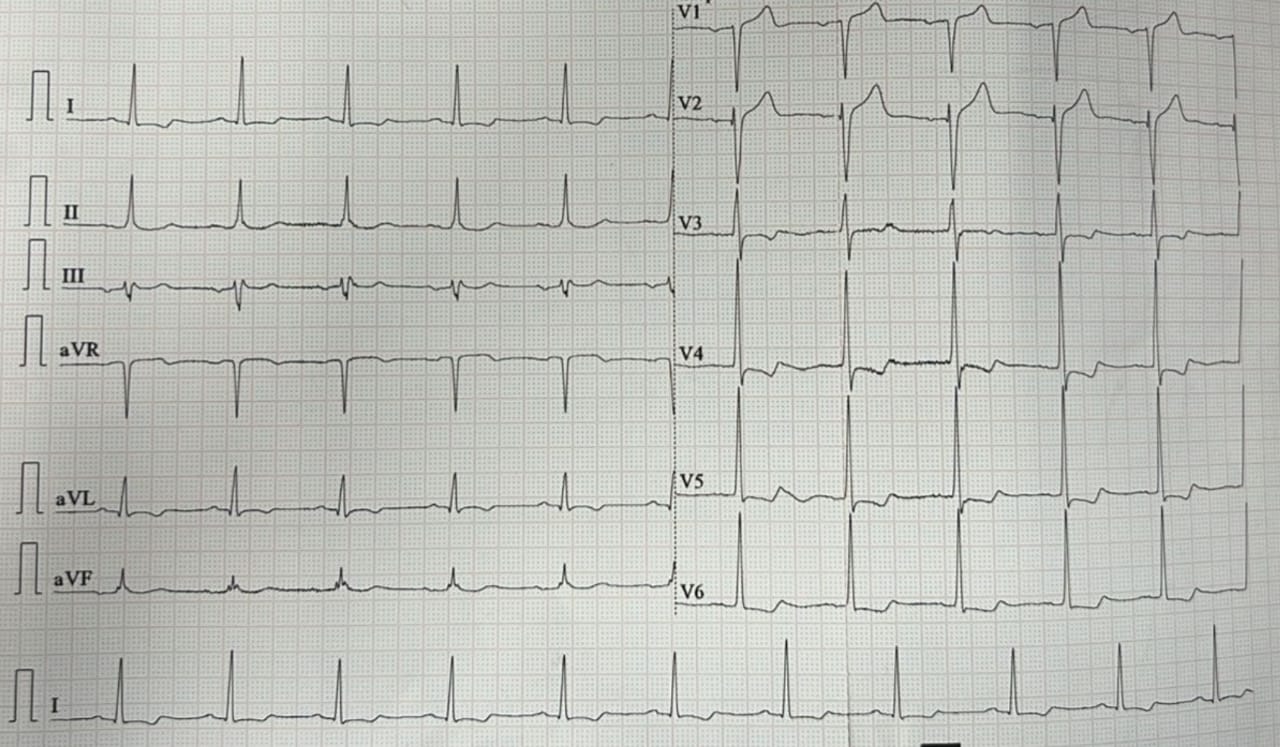
Electrocardiography shows normal sinus rhythm with anterior ischemic pattern. Echocardiography shows mild septal hypertrophy with hypokinetic area at posterior wall and mildly decreased ejection fraction up to 40-45%. Valves within the normal limit.
Relevant Catheterization Findings
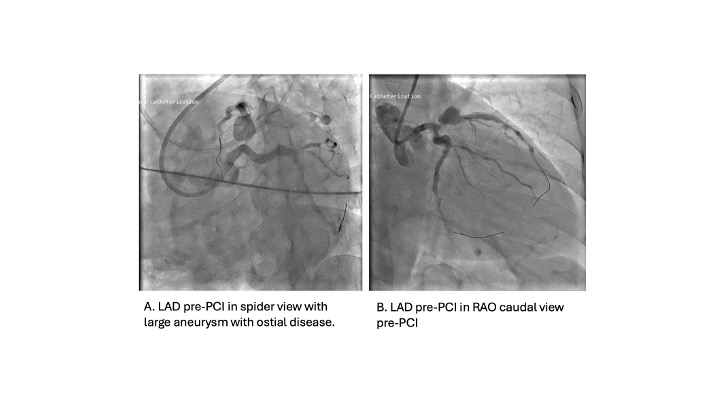
Coronary angiography reveal distal left main disease with 50% stenosis. Left anterior descending artery show giant coronary aneurysm at near ostium with short edge to left main, distal tight lesion 70-80% didisease. Left circumflex with distal disease 80% stenosis and right coronary artery show proximal CTO.
Interventional Management
Procedural Step
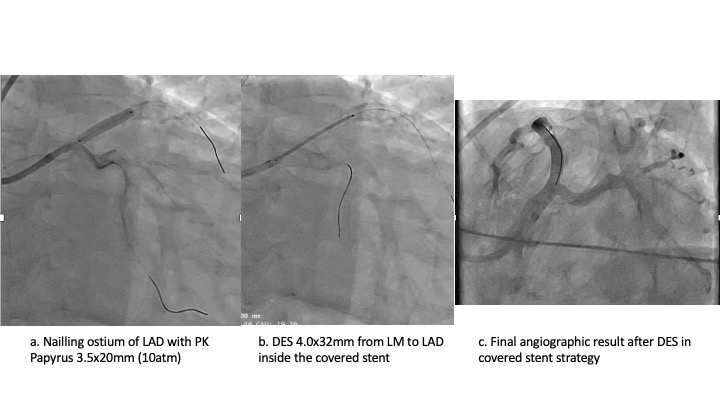
The aneurysmatic region located near the ostium of the LAD is the primary obstacle in this instance. Therefore, we employed a 7Fr EBU 3.5 GC and connected the distal LAD and LCx. Initially, we address the distal LCx lesion by pre-dilating it with NC Scoreflex Trio 3.0x15mm. Subsequently, we treat it with PCB 3.0x15mm, which results in minimal recoil and no dissection. Subsequently, we conducted an IVUS examination of the LAD lesion. Some calcification was noted at mid-to-distal LAD; beyond the aneurysmatic segment, the aneurysmatic segment couldn't be measured as the IVUS depth could not reach the wall. It is estimated from angiography to be 15 mm in size. Ostial LAD and distal to aneurysmatic segment is prepared up to NC Scoreflex Trio 3.0x15mm. Next, we carefully place a covered stent at the ostial LAD to cover the aneurysm segment, ensuring it does not cover the circumflex. We used a PK Papyrus 3.5x20mm and post-dilated the edge of the cover stent using NC 4.0x12mm. Next, we stented the left main to the proximal LAD, passing the cover stent through with a DES Megatron 4.0x32mm. This was succeeded by a POT balloon measuring 4.5x6mm and operating at 20 atm. Next, we utilise a scoring balloon to prepare the mid- to distal LAD lesion and administer Paclitaxel DCB 3.0x30mm. The final IVUS results were favourable, with an LM MSA of 13mm2 and an ostial LAD of 10.47mm2, and no obstruction to the circumflex ostium.
Case Summary
A covered stent is a relatively new therapeutic option for PCI in giant coronary aneurysms. Several limitations were observed with covered stent angioplasty, including the high percentage of restenosis, occlusion of side branches, and difficulty of stent delivery. Stent-assisted coiling or surgical intervention are typically the recommended options for large aneurysms, particularly those located near major branches. In this article, we emphasise the successful intervention of a challenging giant coronary aneurysm with a short proximal edge and ostial disease using PK Papyrus superimposed with a drug-eluting stent.