
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-243
An Alternative Retrograde Access Puncture for Endovenous Laser Ablation: A Case Report
By Catur Rizky Kurniawan, Novi Kurnianingsih
Presenter
Catur Rizky Kurniawan
Authors
Catur Rizky Kurniawan1, Novi Kurnianingsih1
Affiliation
Dr. Saiful Anwar East Java Province Public Hospital, Indonesia1,
View Study Report
TCTAP C-243
Endovascular - Venous Disease Intervention
An Alternative Retrograde Access Puncture for Endovenous Laser Ablation: A Case Report
Catur Rizky Kurniawan1, Novi Kurnianingsih1
Dr. Saiful Anwar East Java Province Public Hospital, Indonesia1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A 69-year-old female reports unilateral leg swelling, which has been present since 2023. The swelling worsens with prolonged standing (more than 1 hour) and moderate activity. Physical examination revealed hyperpigmentation and varicose on her leg. signs of arterial abnormalities are unavailable.
Relevant Test Results Prior to Catheterization
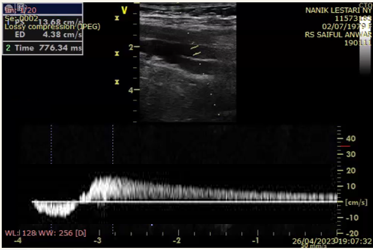
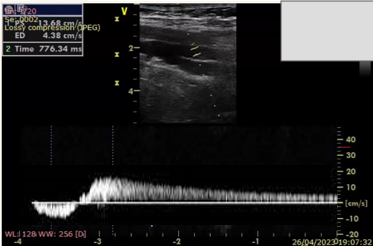
Duplex ultrasound result:
Positive reflux (+) > 750 ms with distal squeeze test on the right great saphenous vein.Positive reflux (+) 500-750 ms with distal squeeze test on the left great saphenous vein.Distal diameter of the right great saphenous vein: 5.9 mm left.Conclusion:Normal blood flow in the arteries of both lower limbs.Severe CVI in the superficial veins of the right lower limb
Positive reflux (+) > 750 ms with distal squeeze test on the right great saphenous vein.Positive reflux (+) 500-750 ms with distal squeeze test on the left great saphenous vein.Distal diameter of the right great saphenous vein: 5.9 mm left.Conclusion:Normal blood flow in the arteries of both lower limbs.Severe CVI in the superficial veins of the right lower limb
Relevant Catheterization Findings
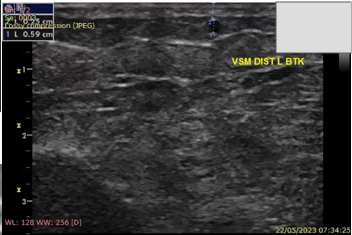
In the preprocedural exam, the narrowest GSV diameter was 5.9 mm near the puncture site. Attempts at IV access through the right GSV using an antegrade approach failed, leading to severe vasospasm (down to 2 mm) that hindered further cannulation. Nitroglycerin (0.2–0.5 mg IV) was locally applied to relieve the spasm, but with minimal improvement, even after exploring other sites and ensuring hydration. A retrograde approach via the proximal SFJ was then considered to bypass the narrowed GSV.
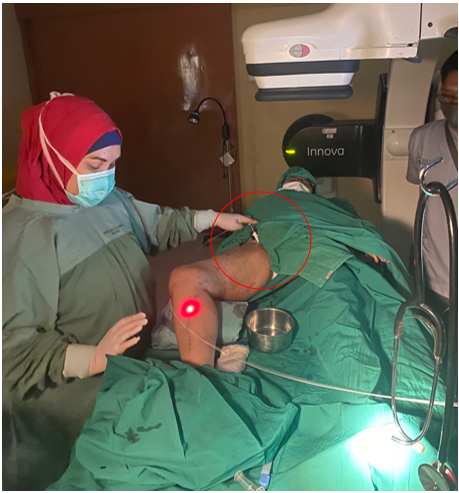
Interventional Management
Procedural Step
In the preprocedural assessment, we identified the narrowest diameter of the great saphenous vein (GSV) as 5.9 mm near the puncture area. An initial attempt was made to establish IV access in the right GSV using an antegrade approach. However, multiple attempts were unsuccessful, and severe vasospasm occurred, reducing the vein's diameter to approximately 2 mm and complicating further cannulation.
To manage this, we applied nitroglycerin (0.2–0.5 mg IV) locally as a vasodilator directly at the affected site, aiming to relieve the vasospasm and facilitate access. Despite these efforts, including exploring alternative cannulation sites and ensuring proper hydration, there was minimal improvement, and cannulation remained challenging.
Due to these difficulties, we opted for a retrograde approach to perform endovenous laser ablation (EVLA) through the proximal saphenofemoral junction (SFJ), effectively bypassing the problematic, constricted portion of the GSV. This approach enabled us to proceed with EVLA while avoiding the complications posed by the severe vasospasm and challenging access through the narrow segment of the GSV.


To manage this, we applied nitroglycerin (0.2–0.5 mg IV) locally as a vasodilator directly at the affected site, aiming to relieve the vasospasm and facilitate access. Despite these efforts, including exploring alternative cannulation sites and ensuring proper hydration, there was minimal improvement, and cannulation remained challenging.
Due to these difficulties, we opted for a retrograde approach to perform endovenous laser ablation (EVLA) through the proximal saphenofemoral junction (SFJ), effectively bypassing the problematic, constricted portion of the GSV. This approach enabled us to proceed with EVLA while avoiding the complications posed by the severe vasospasm and challenging access through the narrow segment of the GSV.
Case Summary
Retrograde Access EVLA is a viable alternative when antegrade access fails.Retrograde access is safe and effective for treating venous insufficiency in severe vasospasm or anatomical challenges.Future Research is needed for long-term efficacy and safety comparison with antegrade EVLA.