
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-087
A Case of RCA Chronic Total Occlusion That Was Difficult to Treat Despite a Retrograde Approach via Saphenous Vein Graft (SVG) With Severe Stenosis
By Ryoki Narita, Shozo Ishihara
Presenter
Ryoki Narita
Authors
Ryoki Narita1, Shozo Ishihara1
Affiliation
Mimihara General Hospital, Japan1,
View Study Report
TCTAP C-087
Coronary - Complex PCI - CTO
A Case of RCA Chronic Total Occlusion That Was Difficult to Treat Despite a Retrograde Approach via Saphenous Vein Graft (SVG) With Severe Stenosis
Ryoki Narita1, Shozo Ishihara1
Mimihara General Hospital, Japan1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
Case: 61 year-old man was underwent PCI for RCA chronic total occlusion (CTO) due to worsening chest pain. He had a past history of coronary artery bypass graft (CABG) 6 years ago. (Coronary Risk Factor)Hypertension, Diabetes, Smoking.

Relevant Test Results Prior to Catheterization
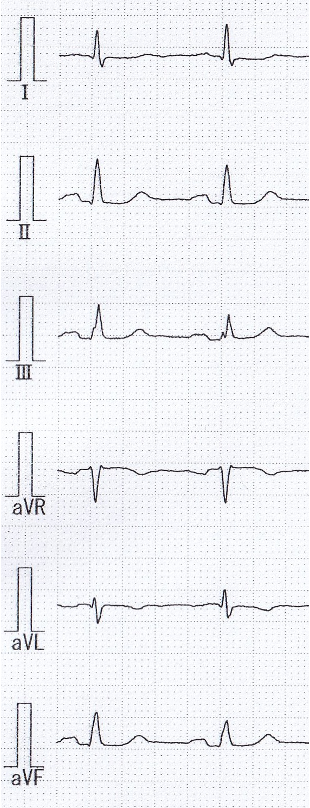
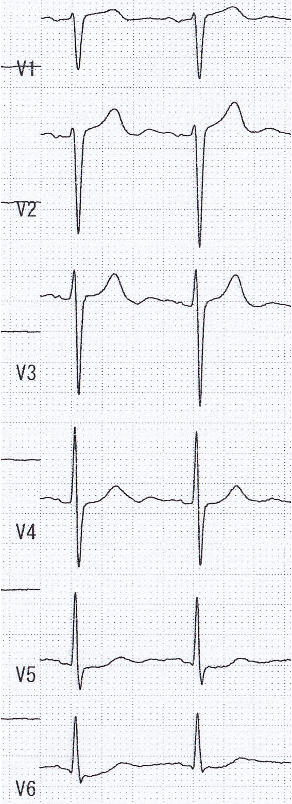
ECG: sinus,ST depression in I,aVL,V5,V6 leads.UCG:LVEF 60%,wallmotion anteroseptal mid~apex hypokinesis, inferior severe hypokinesis. No ventricular wall thinning. No significant valvular disease observed.Blood examination:HbA1c 9.1%,LDL-chol 101 mg/dL,Cre 1.23 mg/dL,eGFR 47.8,Hb 15.8 g/dL,CPK 51 IU/L,BNP 109.1 pg/mL.Exercise electrocardiography: ST depression in Ⅱ,Ⅲ,aVF leads.

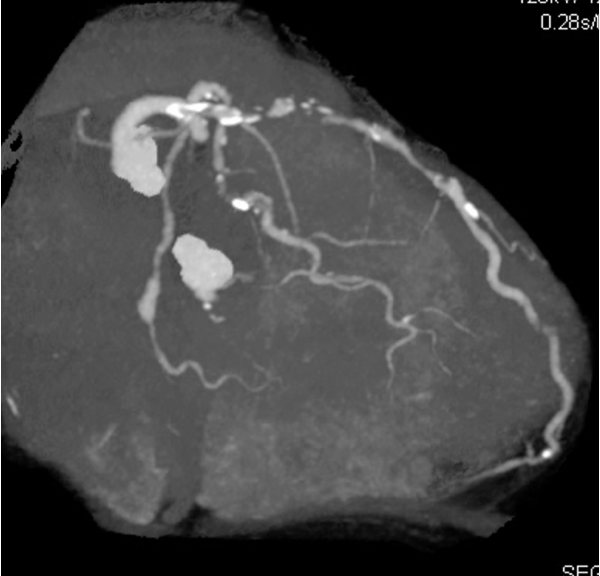

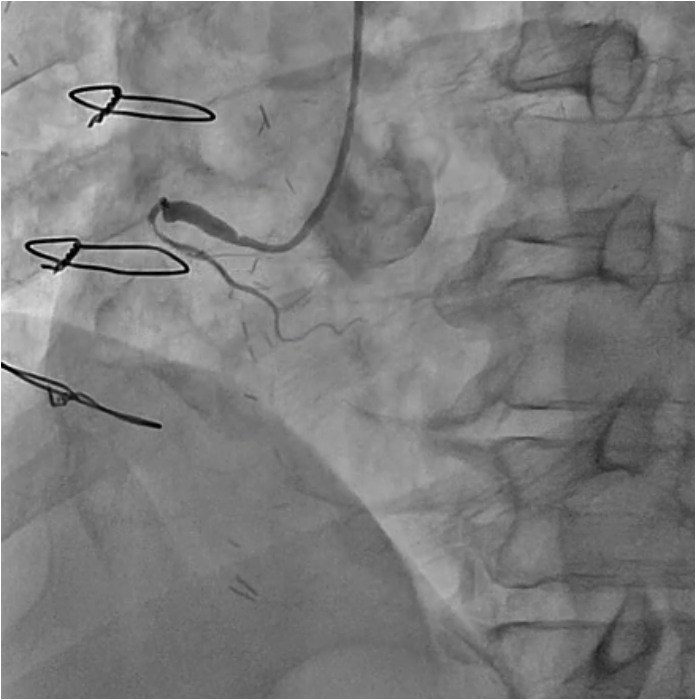
Relevant Catheterization Findings
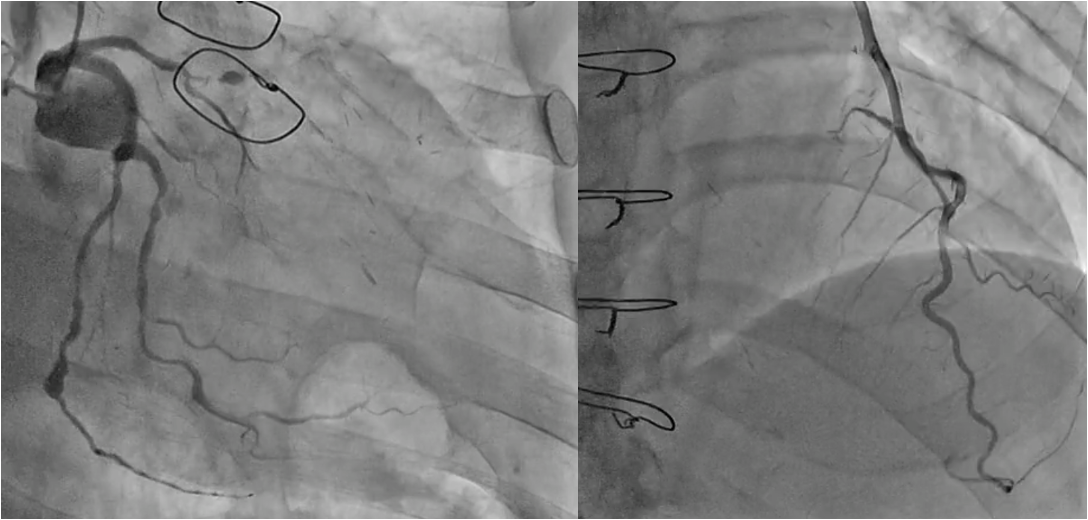
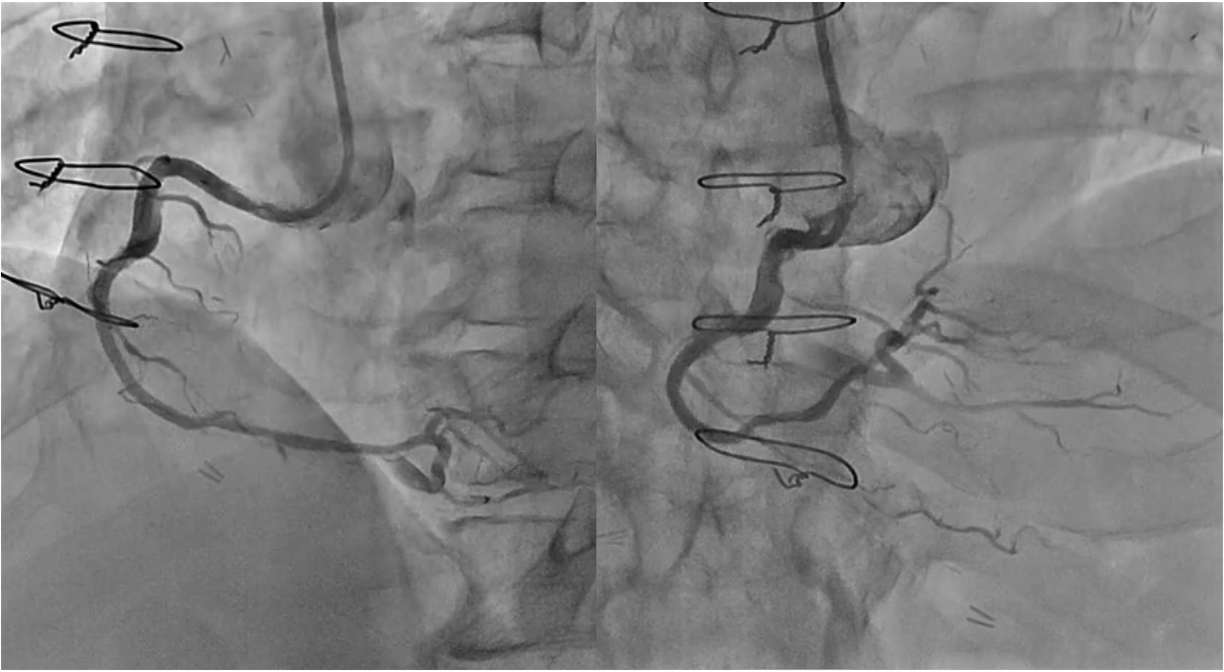
RCA: Seg1)total occlusion, Bypass graft SVG-RCA 99%. LCA:LAD Seg7)total occlusion,LCx Seg12)90%,seg13)90%.seg14)total occlusion, Bypass graft LITA-LAD・FreeRITA-LCX patent, SVG-seg9)occluded.
Interventional Management
Procedural Step
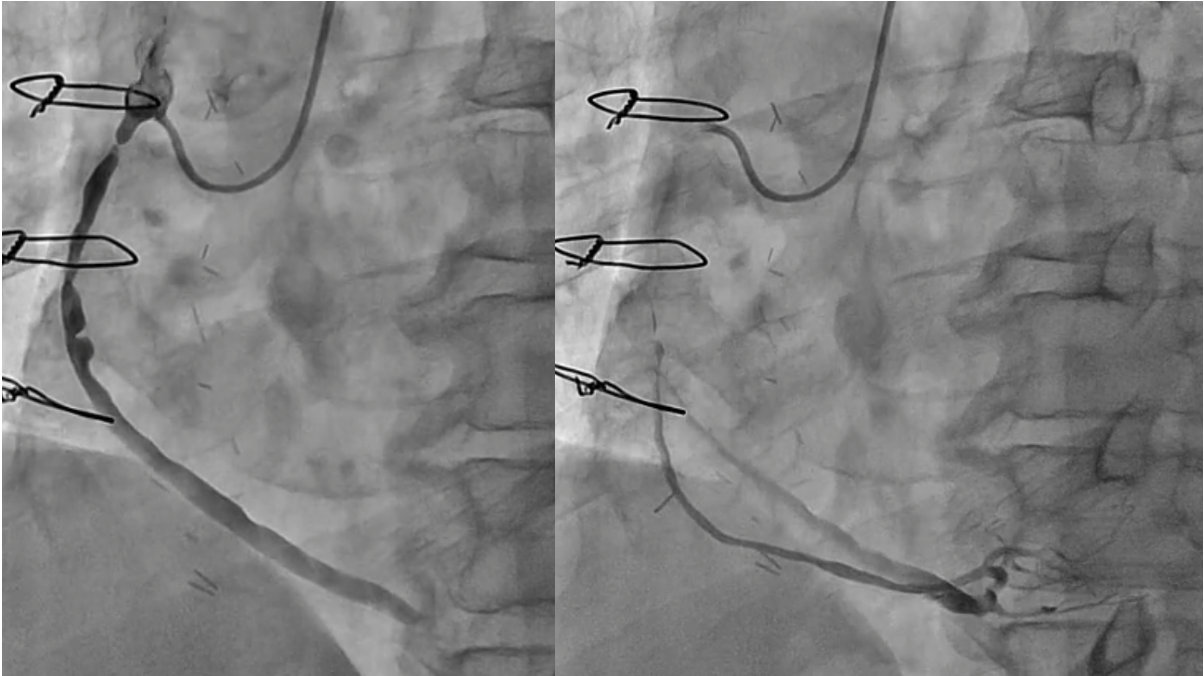
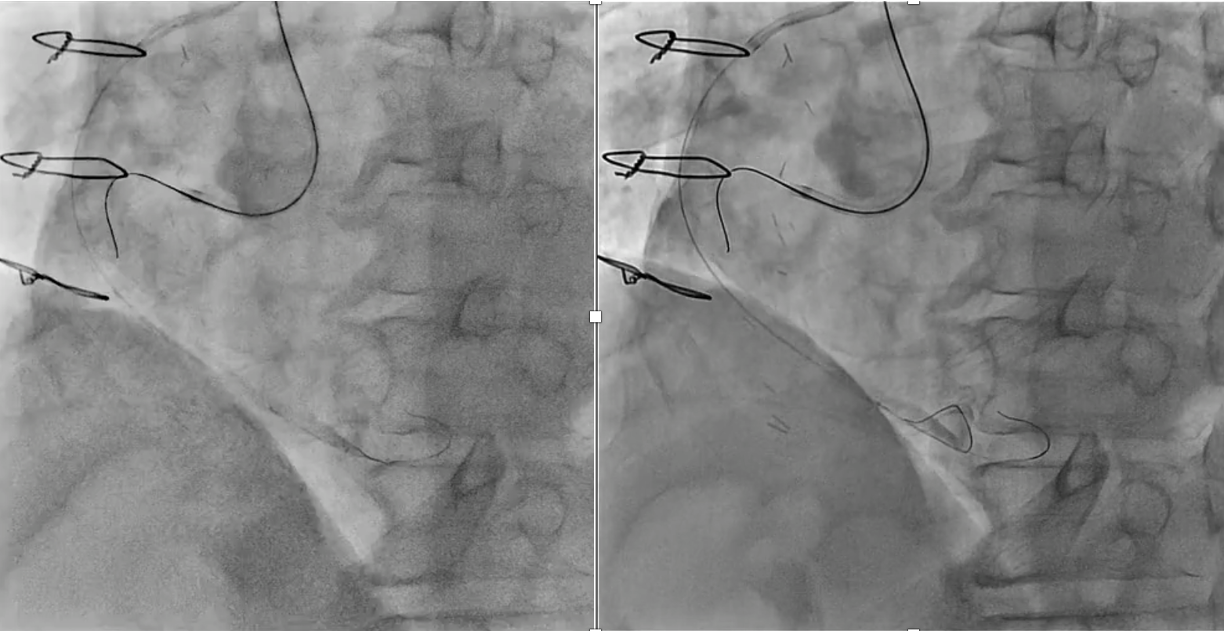
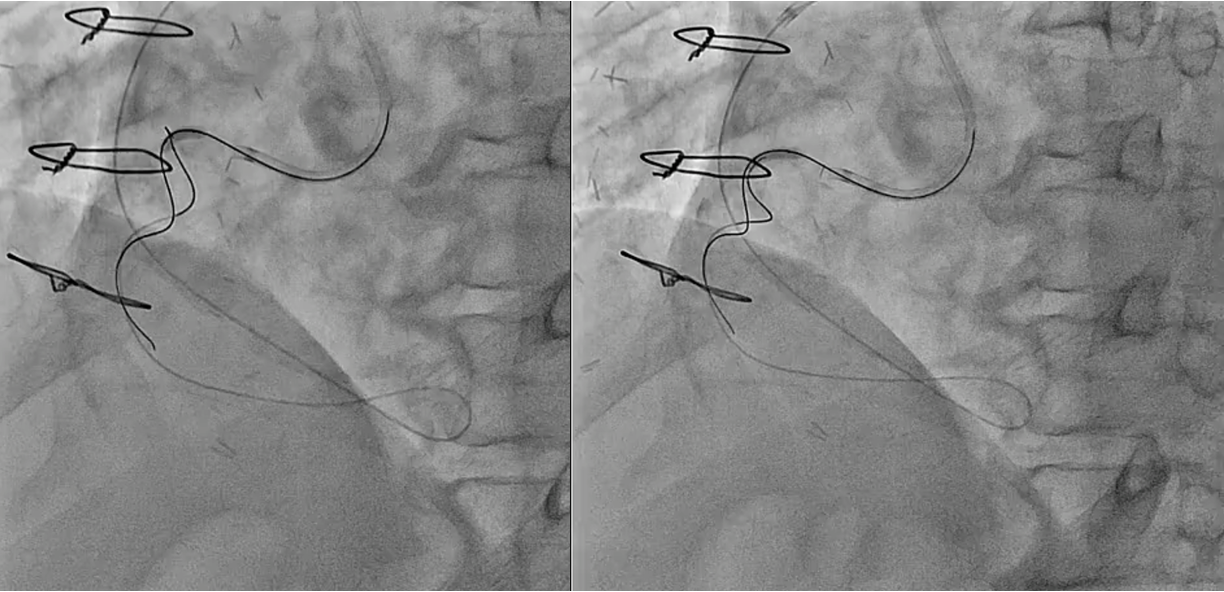
PCI for the degenerated SVG was determined to be at high risk of distal embolism so we planned to perform PCI for native RCA. Antegrade wire crossing was thought to be difficult (J-CTO score was 3 : calcification, bending and lesion length), therefore we planned retrograde approach via SVG. To avoid ischemia during the retrograde procedure, we dilated the severe stenotic lesion in SVG with small balloon and then micro catheter was advanced. It was very difficult to pass the graft anastomosis, but reverse wire technique at distal RCA was effective. Even after the advancement of both antegrade and retrograde wires, it was also difficult to pass the CTO lesion due to strong bending. Finally, retrograde wire was passed with Reverse CART technique and externalization was achieved. After DES implantation, native RCA was nicely revascularized.
Case Summary
This case was a case of angina pectoris associated with severe stenosis of an SVG-RCA bypass graft.We report this educational case including some tips (retrograde approach via SVG, reverse wire technique for anastomosis passage, etc..) with some discussion.