
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-242
Retrieval of Dislodged Central Vein Stent at Right Ventricle
By Chien Hsien Lo
Presenter
Chien Hsien Lo
Authors
Chien Hsien Lo1
Affiliation
Da-Chien General Hospital, Taiwan1,
View Study Report
TCTAP C-242
Endovascular - Venous Disease Intervention
Retrieval of Dislodged Central Vein Stent at Right Ventricle
Chien Hsien Lo1
Da-Chien General Hospital, Taiwan1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
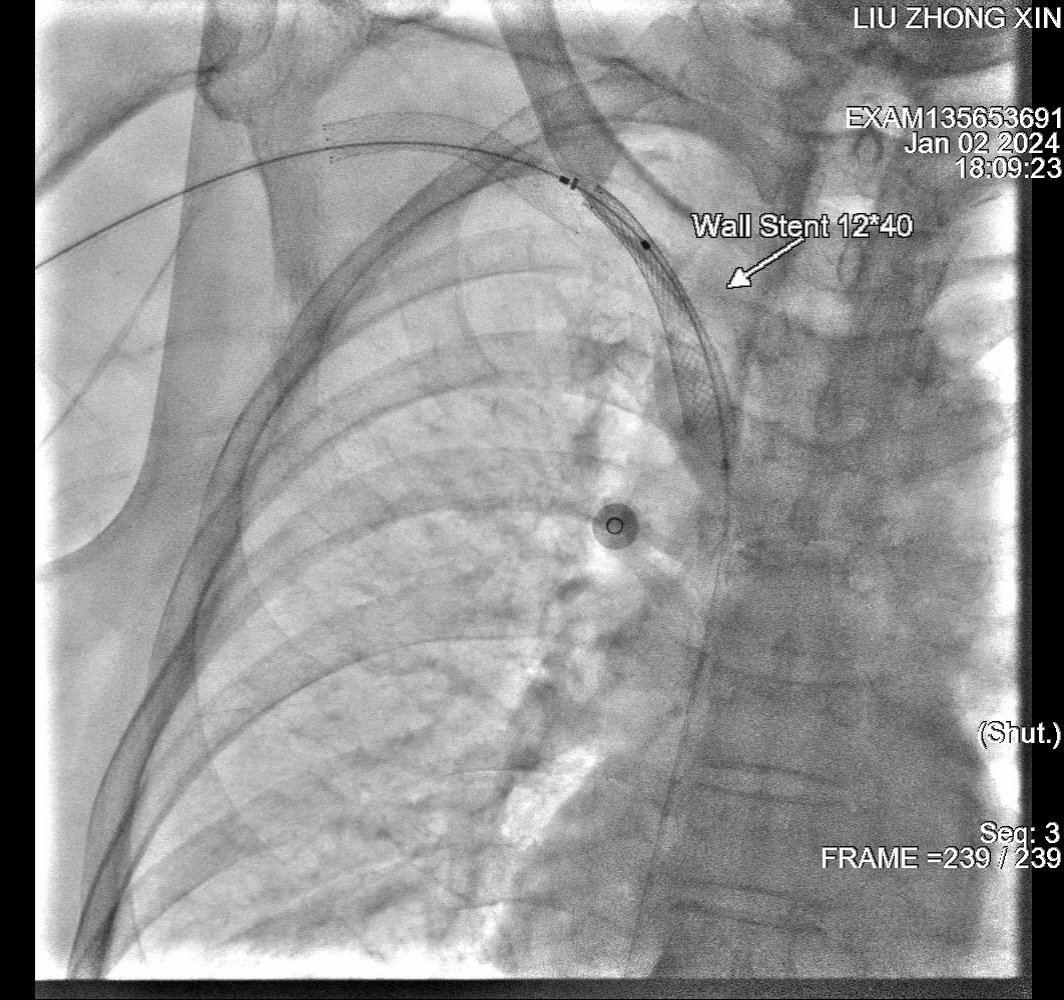
A 76-years-old man, has past history of T2DM with nephropathy and retinopathy, HCVD CAD, double vessel disease, s/p DES to LAD, BMS to D-LCX, ESRD with regular dialysis via right upper arm AVF. He had intermittent right arm swelling due to right subclavian-brachiocephalic vein CTO, balloon angioplasty was done. Due to recurrent occlusion, BMS Boston 12*40mm stent was deployed at right brachiocephalic vein. This time, he suffered from worsening dyspnea on exertion.
Relevant Test Results Prior to Catheterization
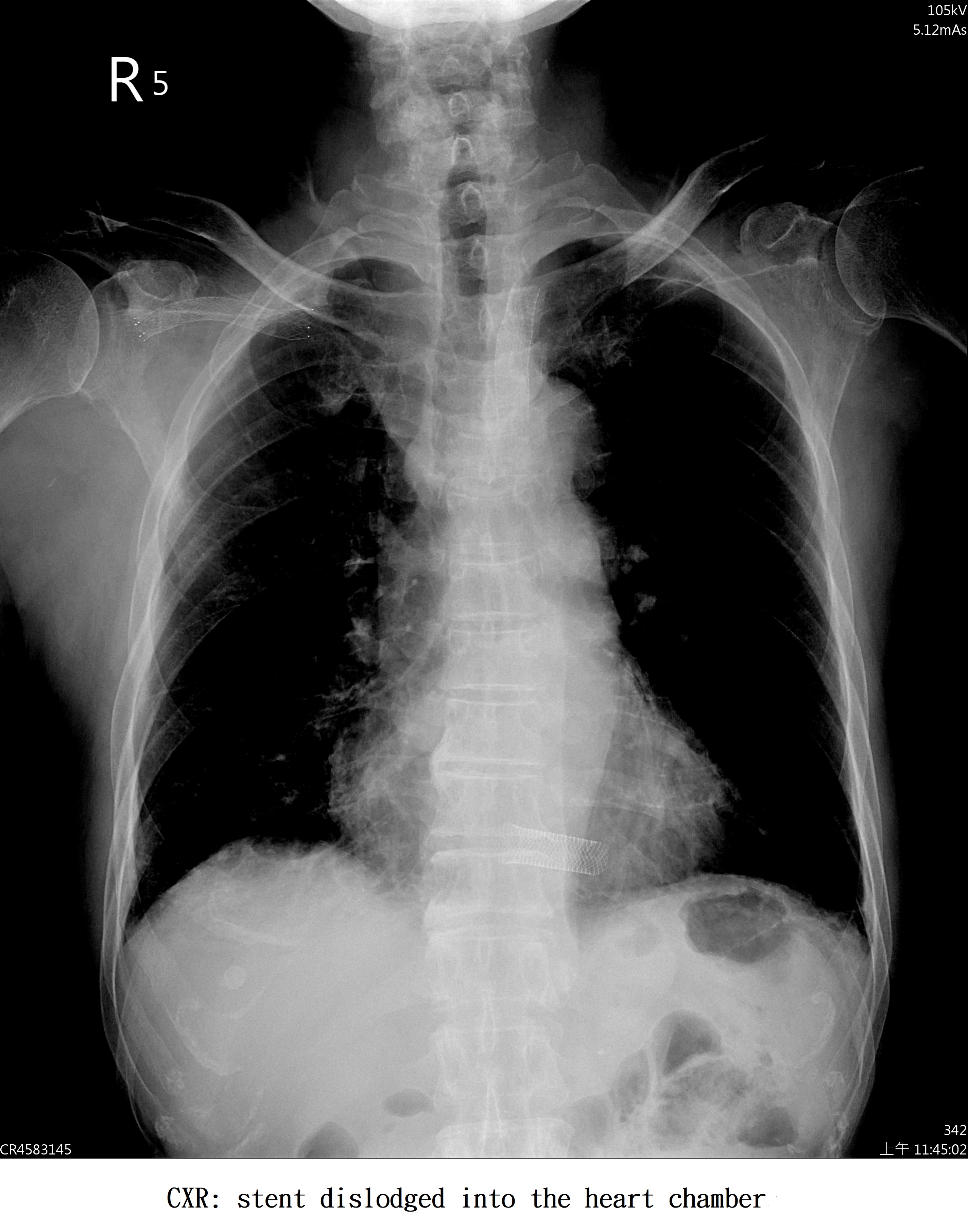
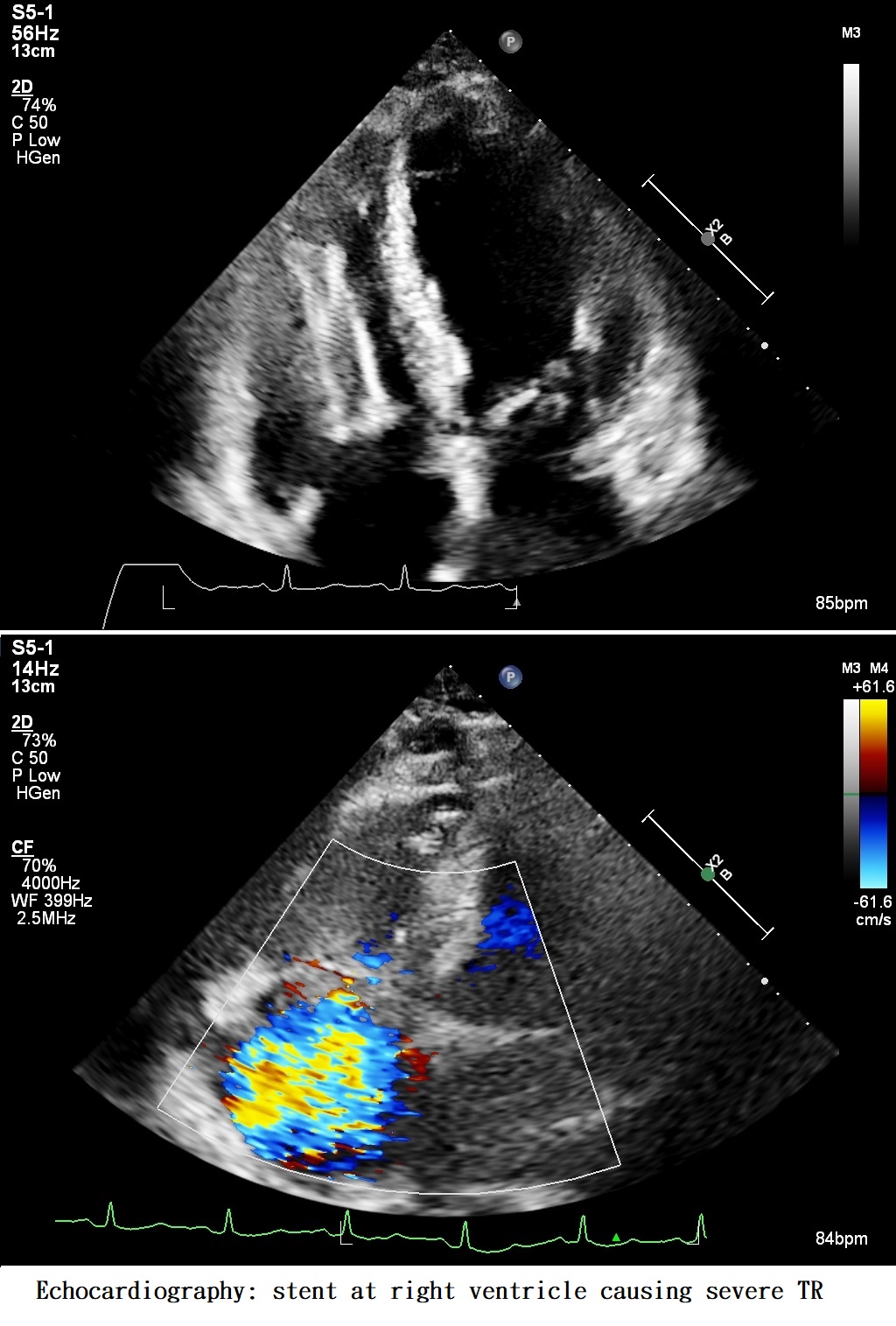
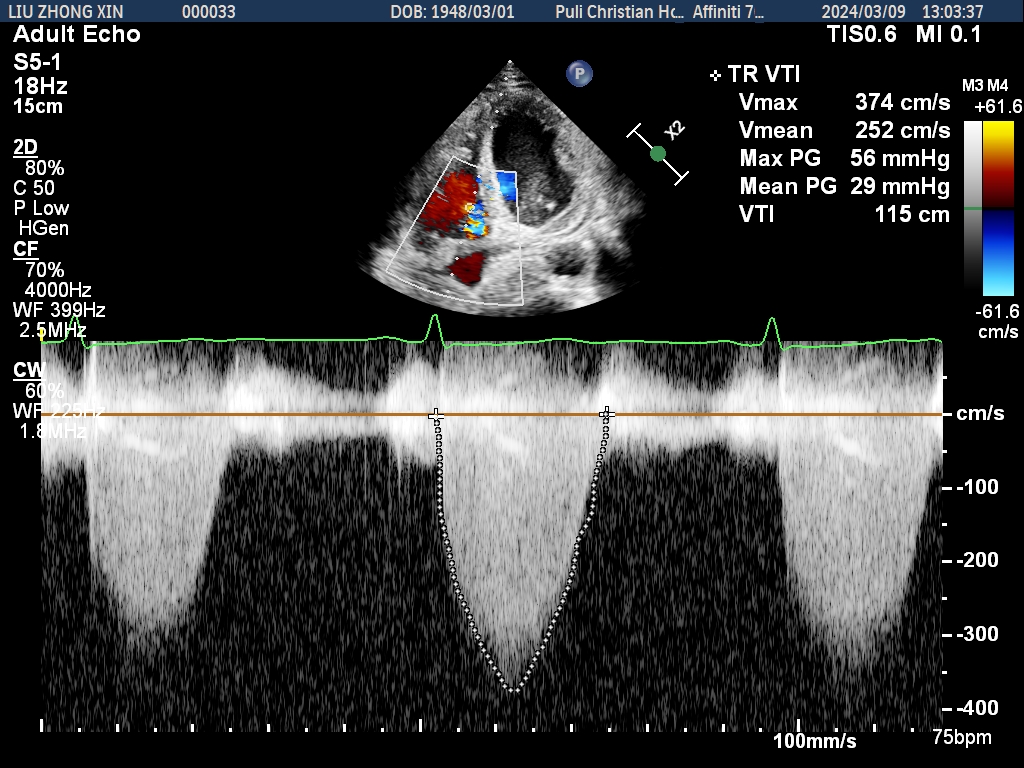
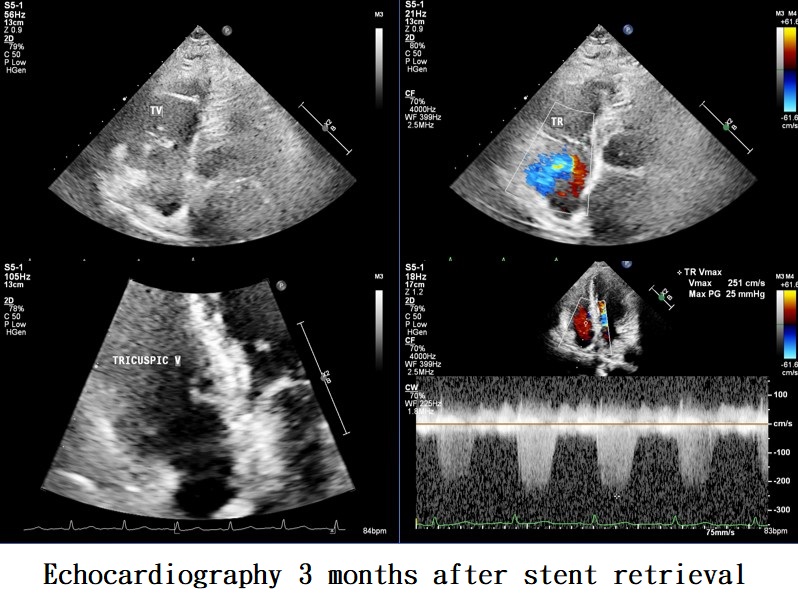
Lab data showed anemia and chronic elevated Cr level. CXR showed stent placed at RV. Echocardiography revealed dislodged stent attached at tricuspid valve, into the RV, causing severe TR and pulmonary hypertension.
Relevant Catheterization Findings
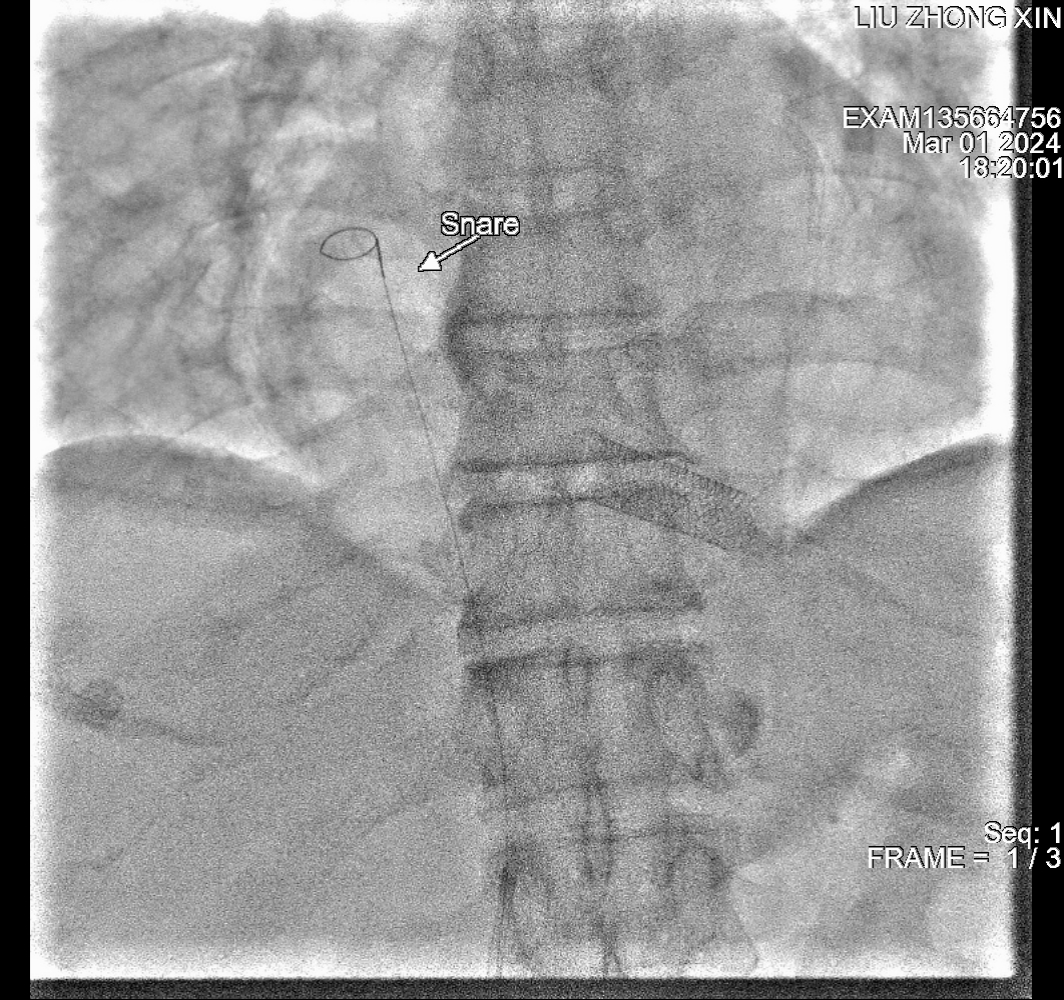
First endovascular management: use single loop snare, self made loop snare, Tried about 1.5 hour but failed to retrieval of stent. Next step? Surgical removal which need open heart. Consider try endovascular retrieval again. Choice of route: AVF, transjugular or transfemoral? Equipment: sheath size? what snare? need balloon?
Interventional Management
Procedural Step
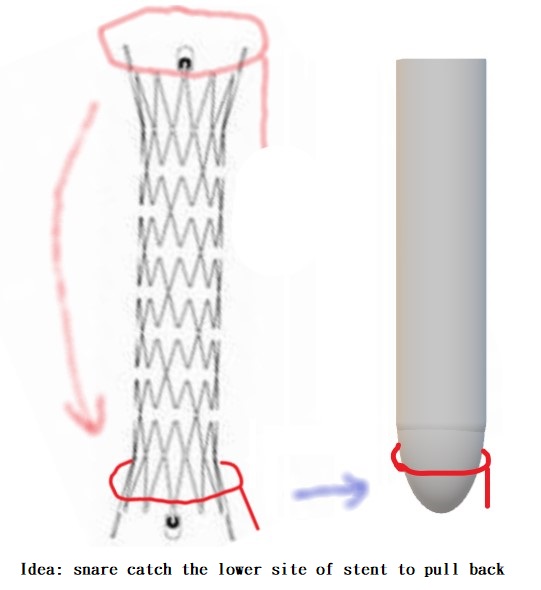
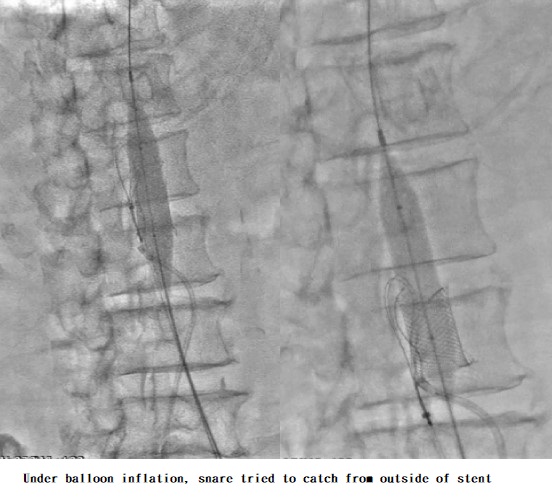
-From right transfemoral approach and 8Fr sheath, used 0.035" Terumo wire tried to pull back the stent but failed.-Used guiding catheter 7Fr SAL1 with 3-loops snare, tried for 15-20 mins but failed.-Used 0.014”Sion wire and 0.014" 4.0*15mm SC balloon cross to stent strut and inflate 8 atm, pull back the stent with slow tractionPull -> VT -> Release -> Pull again that successfully pull back the stent to IVC.-Bilateral approach: left transfemoral puncture with 26Fr long sheath however failed inserted to IVC due to tortuousand angulation of iliac vein so sheath tip placed at external iliac vein.-Right femoral sheath: SAL1 catheter with 4.0*15mm balloon inflation the catch the stent-Left femoral sheath: JR4 catheter cross outside of stent to upper IVC, tried the snare to catch up upper stent strut but failed due to poor alignment of stent.-14*40mm balloon inflation into stent for good alignment, Snare try to loop up stent body from outside changed to self-made snare with 0.035" Terumo wire which catch the lower site of stent and pulled down the stent.-However failed to pull back into the sheath and stent dislodged at common iliac vein angulation site.- Stent fixed and immobile. Then low pressure balloon dilation to stabilized the stent. Final angio showed well iliac vein flow to IVC.- Echocardiography after one week showed partial tear of TV with severe TR and high RVSP.- Follow-up echocardiography after 3 months showed reduce the severity of TR and pulmonary hypertension.
Case Summary
- Stent dislodged into right ventricle is rare, that may cause mechanical complications such as arrhythmia, severe TR, dyspnea etc.- This represented the 1st case of largest stent successfully managed by endovascular treatment.- Multiple techniques and equipment are required for endovascular retrieval (small balloon trapping, snare, large balloon etc.,).