
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-127
Between a Rock and a Hard Place: Case of a Stuck and Broken Intravascular Ultrasound Catheter
By Zhengfeng Jason Chen, Huay Cheem Tan
Presenter
Zhengfeng Jason Chen
Authors
Zhengfeng Jason Chen1, Huay Cheem Tan1
Affiliation
National University Heart Centre, Singapore1,
View Study Report
TCTAP C-127
Coronary - Complication Management
Between a Rock and a Hard Place: Case of a Stuck and Broken Intravascular Ultrasound Catheter
Zhengfeng Jason Chen1, Huay Cheem Tan1
National University Heart Centre, Singapore1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
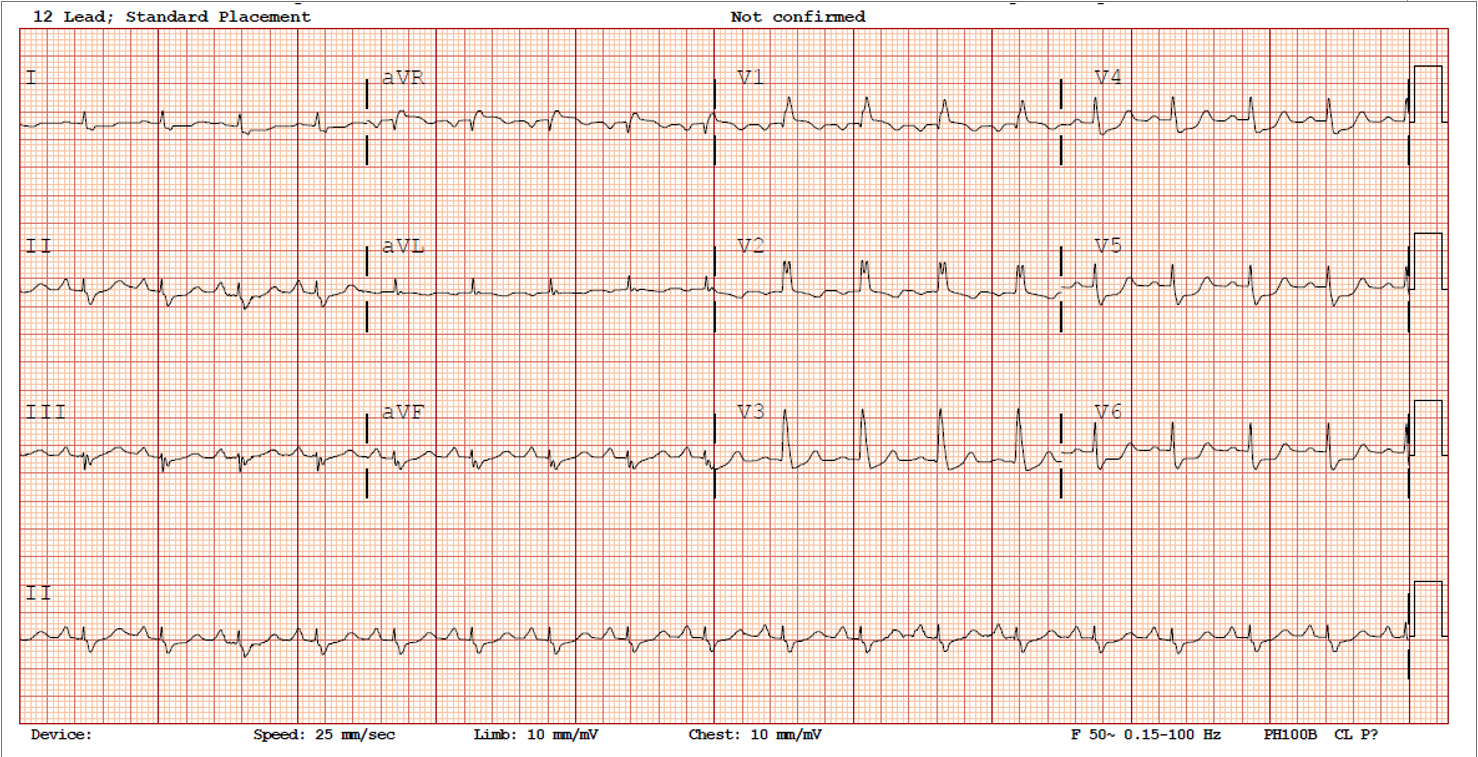
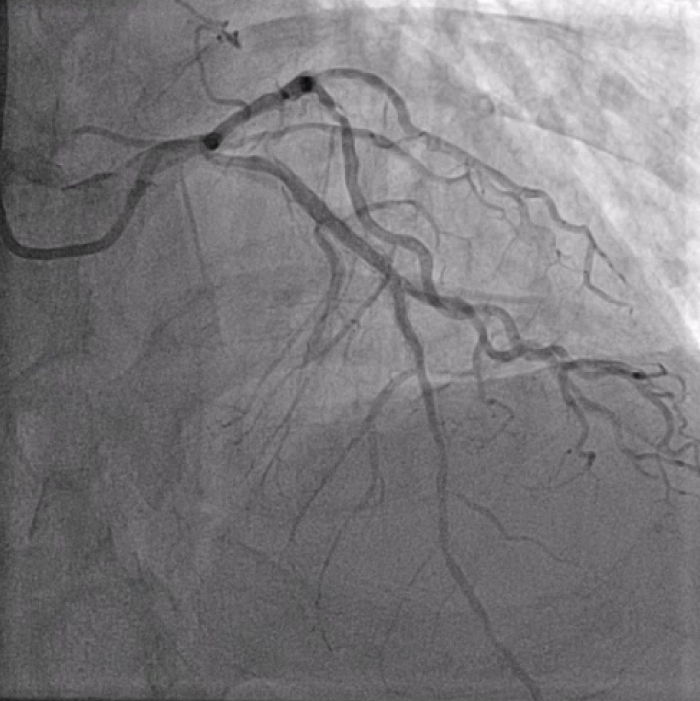
82 year old Chinese gentleman. Past medical history of Diabetes Mellitus, Hypertension, Hyperlipidemia, and Ischemic Heart Disease. He had prior PCI to LAD 20 years ago. He now presents with an Anterior STEMI and underwent emergent balloon angioplasty to the mid LAD Very Late Stent Thrombosis (VLST). There was residual triple vessel disease and was referred to the cardiac surgeons for bypass surgery (CABG). However, he developed worsening angina and deemed too high risk for CABG.
Relevant Test Results Prior to Catheterization
Full blood count, renal function tests were normal. High-sensitivity Troponin I was elevated. Echocardiography showed LVEF 25%.
Relevant Catheterization Findings
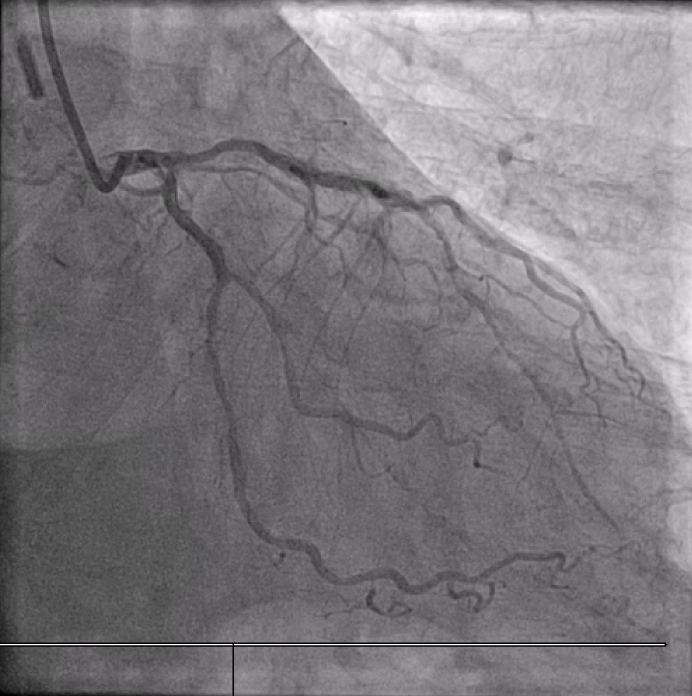
Distal LM intermediate disease, significant proximal LAD ISR, significant mid LCx stenosis. Diffuse high-grade RCA disease (proximal to distal into RPDA). Calcific and angulated proximal RPDA.
Interventional Management
Procedural Step
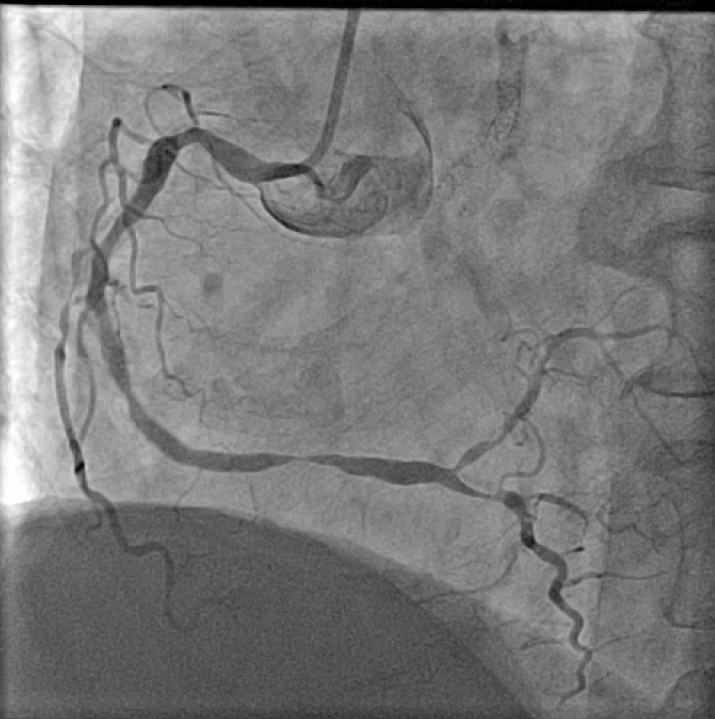
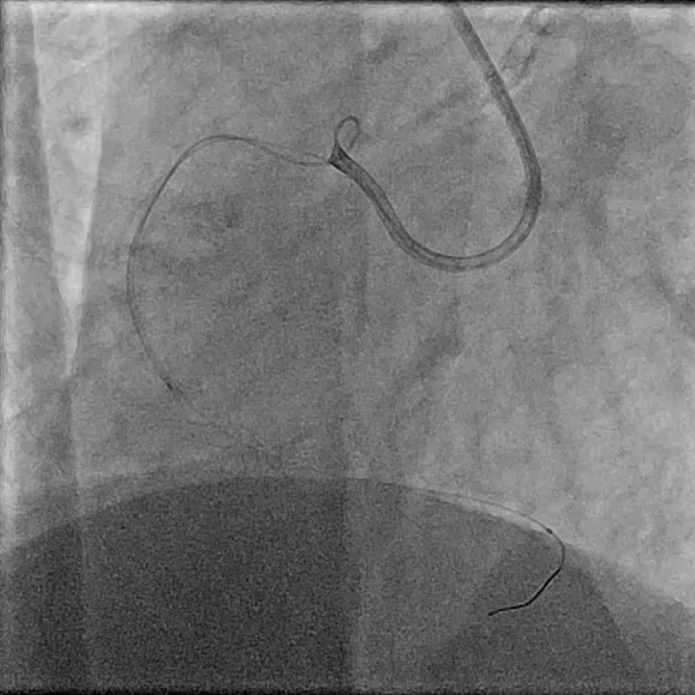
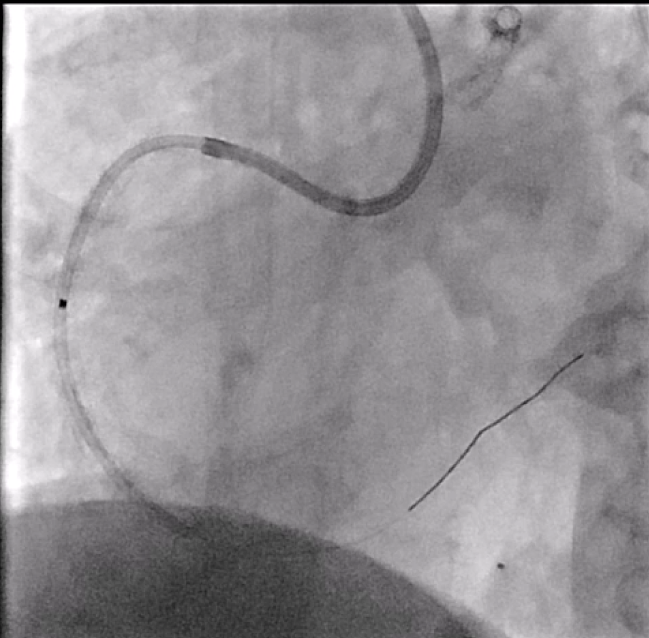
In view of severe left ventricular dysfunction, a 40cc IABP was inserted via the right common femoral artery for mechanical circulatory support during PCI. A 6Fr AL1 guide catheter was advanced via the right radial artery to selectively cannulate the right coronary artery (RCA). A Runthrough NS coronary guidewire was advanced into the distal R-PDA. Balloon angioplasty was performed from RPDA back to proximal RCA using a 2.5x15mm Sapphire3 NC balloon to 12atm. A Boston Scientific Opticross HD 60MHz IVUS catheter was advanced into the distal RPDA and intravascular imaging performed. Unfortunately, upon completion of the pullback run, the IVUS catheter could not be withdrawn. The IVUS catheter was stuck on the calcific and angulated segment in the proximal RPDA. Despite use of focused force technique, parallel ballooning, the IVUS catheter could not be withdrawn. During the attempts, the IVUS catheter inadvertently broke, leaving a short segment of the catheter in the RPDA. Check angiography showed no flow impairment. Thus, proximal to mid RCA was stented using a 3.0x38mm DES and a 3.5x48mm DES. Due to long procedural time, decision made to stage further PCI to the next day. The following day, PCI to LAD was performed uneventfully. The RCA was cannulated using a 7Fr AL2 guide catheter via right radial artery. A Sion Blue ES guidewire was advanced into the RPDA. A 6Fr Liquid guide extension catheter was advanced across the stented segments. A 3.2Fr EnSnare used to withdraw IVUS.

Case Summary
IVUS entrapment usually occurs on stent struts (distal edge, tortuous vessels, calcified lesions, small stent diameter). However, it can still happen in calcified and tortuous vessels. Follow the troubleshooting algorithm, do not forcibly pull. If the catheter breaks, can consider using such a snaring technique to retrieve. If all else fails, can perform CABG and removal of device.