
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-036
Double-Kissing Nano-Crush for Bifurcation PCI Facilitated by Orbital Atherectomy and Shockwave Lithotripsy
By Gavin Ng, Andie Djohan
Presenter
Andie Djohan
Authors
Gavin Ng1, Andie Djohan1
Affiliation
National University Heart Centre, Singapore1,
View Study Report
TCTAP C-036
Coronary - Adjunctive Procedures (Thrombectomy, Atherectomy, Special Balloons)
Double-Kissing Nano-Crush for Bifurcation PCI Facilitated by Orbital Atherectomy and Shockwave Lithotripsy
Gavin Ng1, Andie Djohan1
National University Heart Centre, Singapore1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
Mr. KJ is a 72-year-old male with a background history of end stage renal disease on haemodialysis, diabetes, hypertension, and hyperlipidaemia. He presented with myocardial infarction in August 2023 and underwent coronary angiography which demonstrated left main and triple vessel disease. He was referred to the cardiothoracic surgery team for consideration of coronary artery bypass surgery but declined surgery. He therefore underwent percutaneous coronary intervention.

Relevant Test Results Prior to Catheterization
An echocardiogram demonstrated a left ventricular ejection fraction of 60% and mild aortic regurgitation. Laboratory investigations showed a normal haemoglobin of 13.5 g/dL and end stage renal disease.

Relevant Catheterization Findings
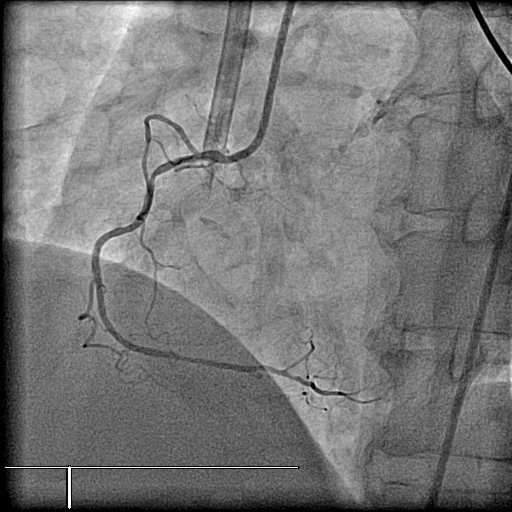
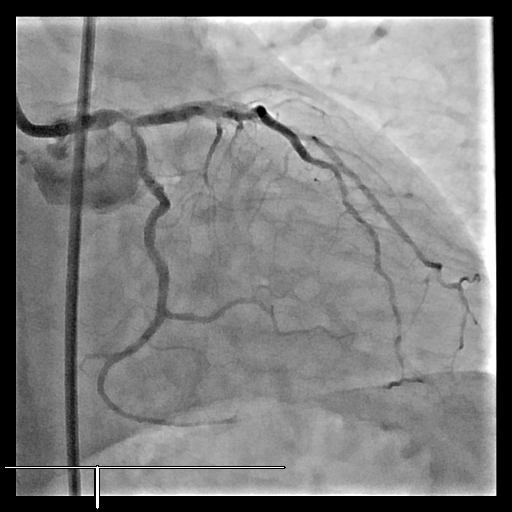
Coronary angiogram performed demonstrated a co-dominant circulation. There was a diffusely diseased right coronary artery with no focal high-grade stenosis. The left coronary arteries were significantly calcified and had a Medina 1,1,1 bifurcating disease involving the distal left main (LM) and ostial left anterior descending (LAD) and left circumflex arteries(LCx).
Interventional Management
Procedural Step
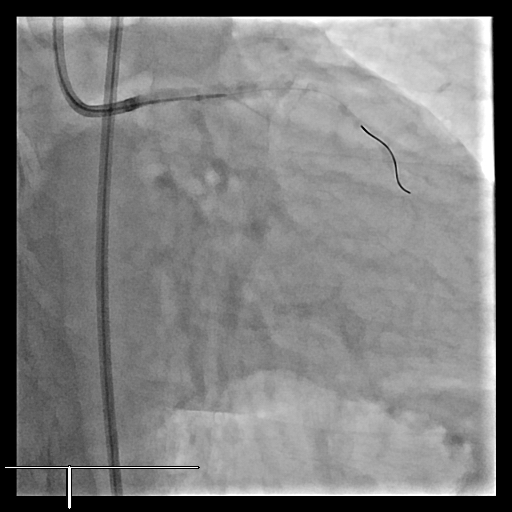
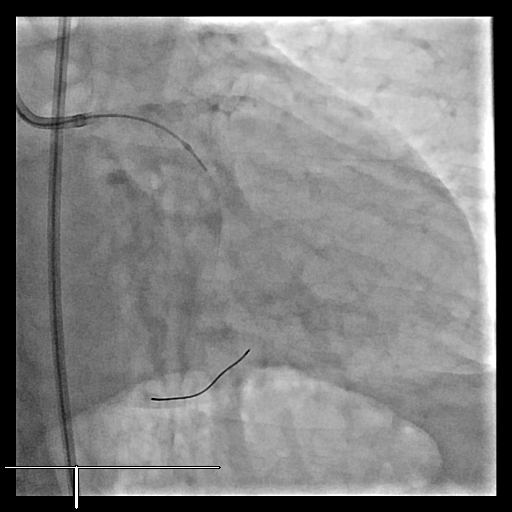
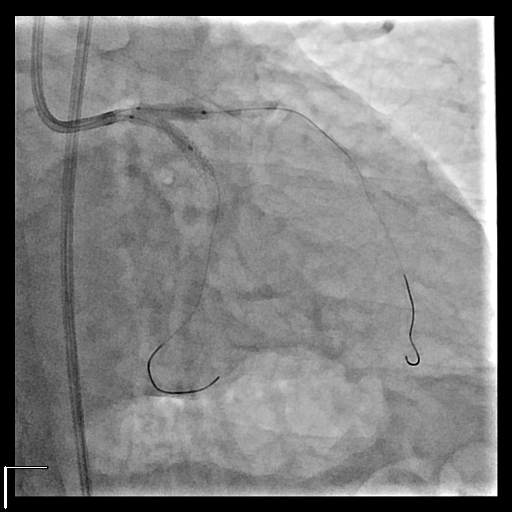
The left coronary ostium was cannulated with a 7 Fr EBU 3.5 guide catheter. A 0.014” Viperwire was advanced to the distal LCx and four runs of orbital atherectomy was performed at 80-120k rpm. This was repeated for the LAD. Thereafter, the Viperwire was exchanged out for workhorse wires. Intravascular ultrasound (IVUS) was performed with a 60 MHz Opticross HD catheter. This demonstrated minimal lumen area (MLA) in the distal LM, ostial LCx and ostial LAD at 3.4 mm2, 2.7 mm2 and 2.6 mm2 respectively. Lesion preparation was done with a 3.0 x 15 mm NC balloon. A 3.0 x 16 mm Drug Eluting Stent (DES) was used to stent from the LM to LCx. IVUS confirmed only 1 stent strut covering the ostial LCx and therefore a Double-Kissing Nano-crush technique was employed. Simultaneous kissing balloon dilation done in the LAD and LCx using two 3.0 x 15 mm NC balloons. Next, a 3.0 x 20 mm DES was used to stent from the ostial LM to mid LAD. Proximal optimization technique (POT) was done with a 4.0 x 6 mm NC balloon. Another 2.75 x 38 mm DES was used to stent distal to and in overlap with the first LAD stent, to the mid LAD. The LCx was re-wired and second kissing balloon dilation and final POT was done. IVUS demonstrated a focal area of restricted stent in the mid LAD and therefore shockwave lithotripsy was performed with a 3.0 x 12 mm Shockwave IVL balloon. Final IVUS demonstrated good result with MLA in the distal LM, ostial LCx and ostial LAD at 12.9 mm2, 6.5 mm2 and 7.8 mm2 respectively.


Case Summary
This case report demonstrated the safety of orbital atherectomy and shockwave lithotripsy in facilitating a Double-Kissing Nano-Crush technique for the treatment of a left main bifurcation lesion. Intravascular ultrasound was crucial in guiding the procedure and allowed for the optimization of the result. At a 4-month review, the patient remains clinically well and asymptomatic. There is increasing complexity in contemporary PCI procedures and it will be required for interventionists to be well versed in imaging and calcium modification techniques.