
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-061
Laser Atherectomy for Calcified Uncrossable Lesion
By Alvin Hon Yeung Ko, Jake Yin Kei Yeung, Alan Ka Chun Chan, Micheal Kang Yin Lee
Presenter
Alvin Hon Yeung KO
Authors
Alvin Hon Yeung Ko1, Jake Yin Kei Yeung1, Alan Ka Chun Chan1, Micheal Kang Yin Lee1
Affiliation
Queen Elizabeth Hospital, Hong Kong, China1,
View Study Report
TCTAP C-061
Coronary - Complex PCI - Calcified Lesion
Laser Atherectomy for Calcified Uncrossable Lesion
Alvin Hon Yeung Ko1, Jake Yin Kei Yeung1, Alan Ka Chun Chan1, Micheal Kang Yin Lee1
Queen Elizabeth Hospital, Hong Kong, China1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
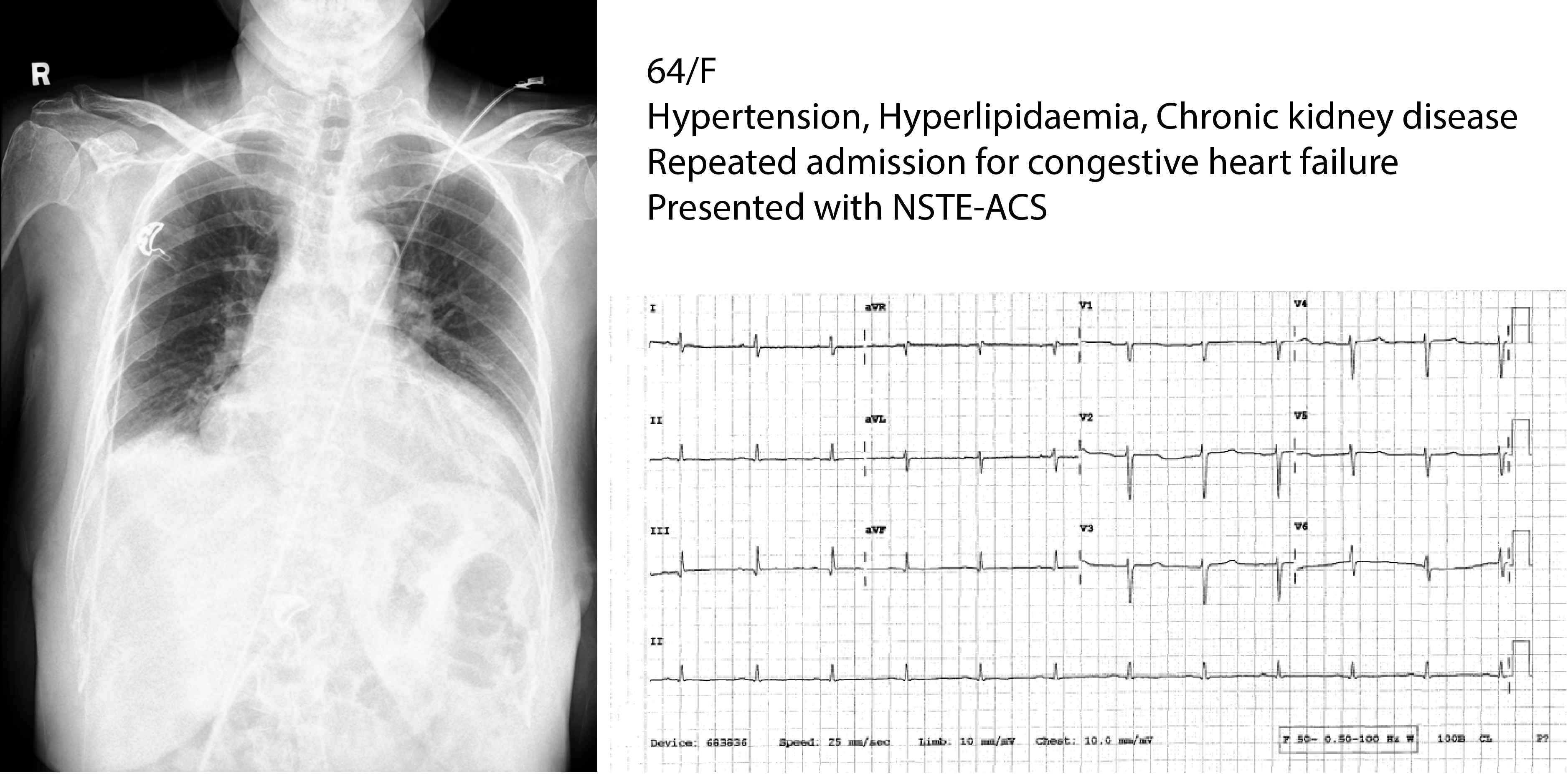
A 64-year-old woman with diabetes, hypertension, hyperlipidaemia and chronic kidney disease presented with non-ST segment elevation myocardial infarction and repeated admission for congestive heart failure.
Relevant Test Results Prior to Catheterization
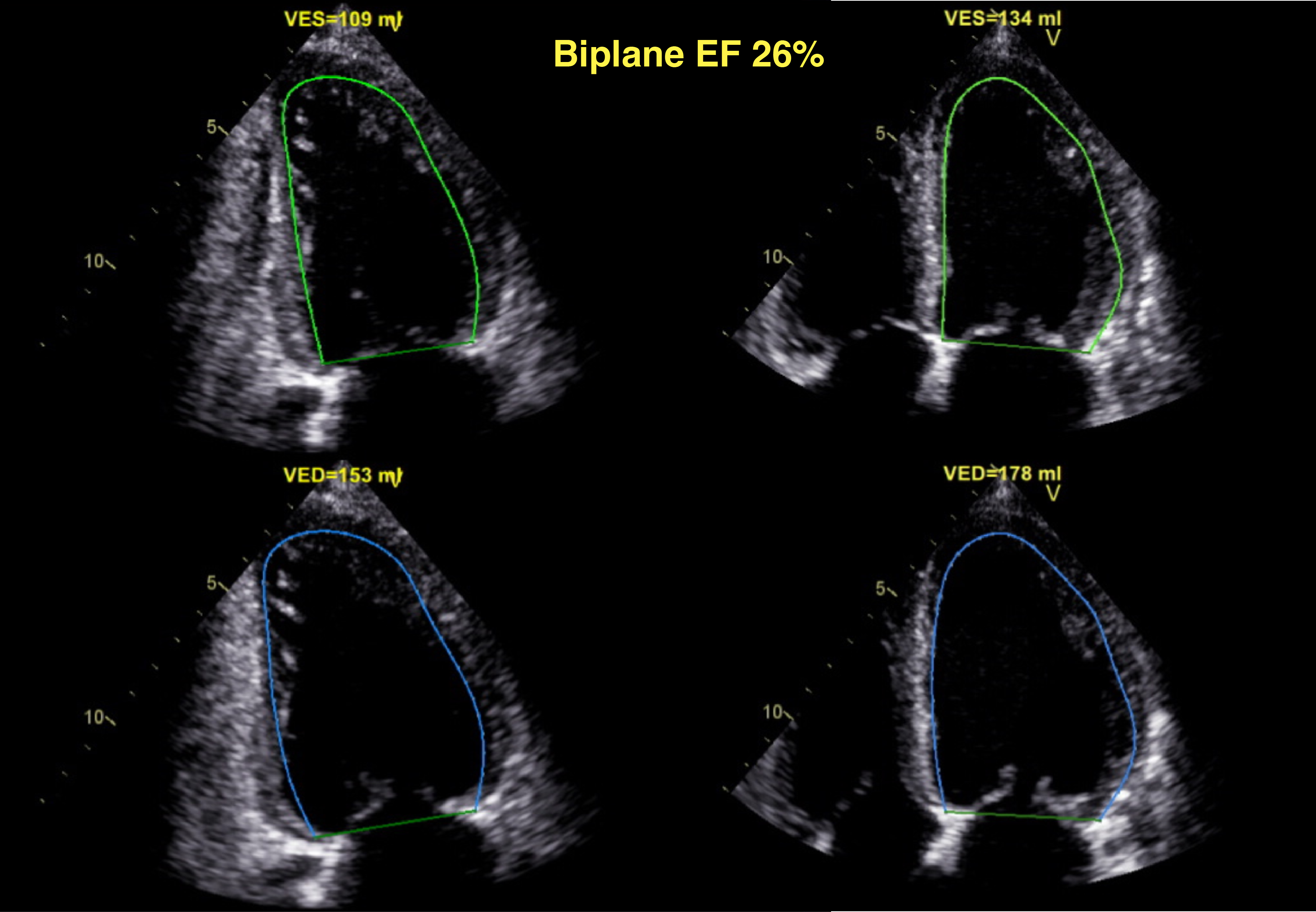
Echocardiogram revealed impaired LVEF ~25% with global hypokinesia, moderate to severe function MR, and moderate TR. Cardiac MRI showed evidence of RCA and suspected LAD territories infarct. Degree of LV dysfunction is disproportionate to the extent of LV infarct, suggestive of possible hibernating myocardium. The case was discussed in multidisciplinary team and decided for high risk supported PCI.
Relevant Catheterization Findings
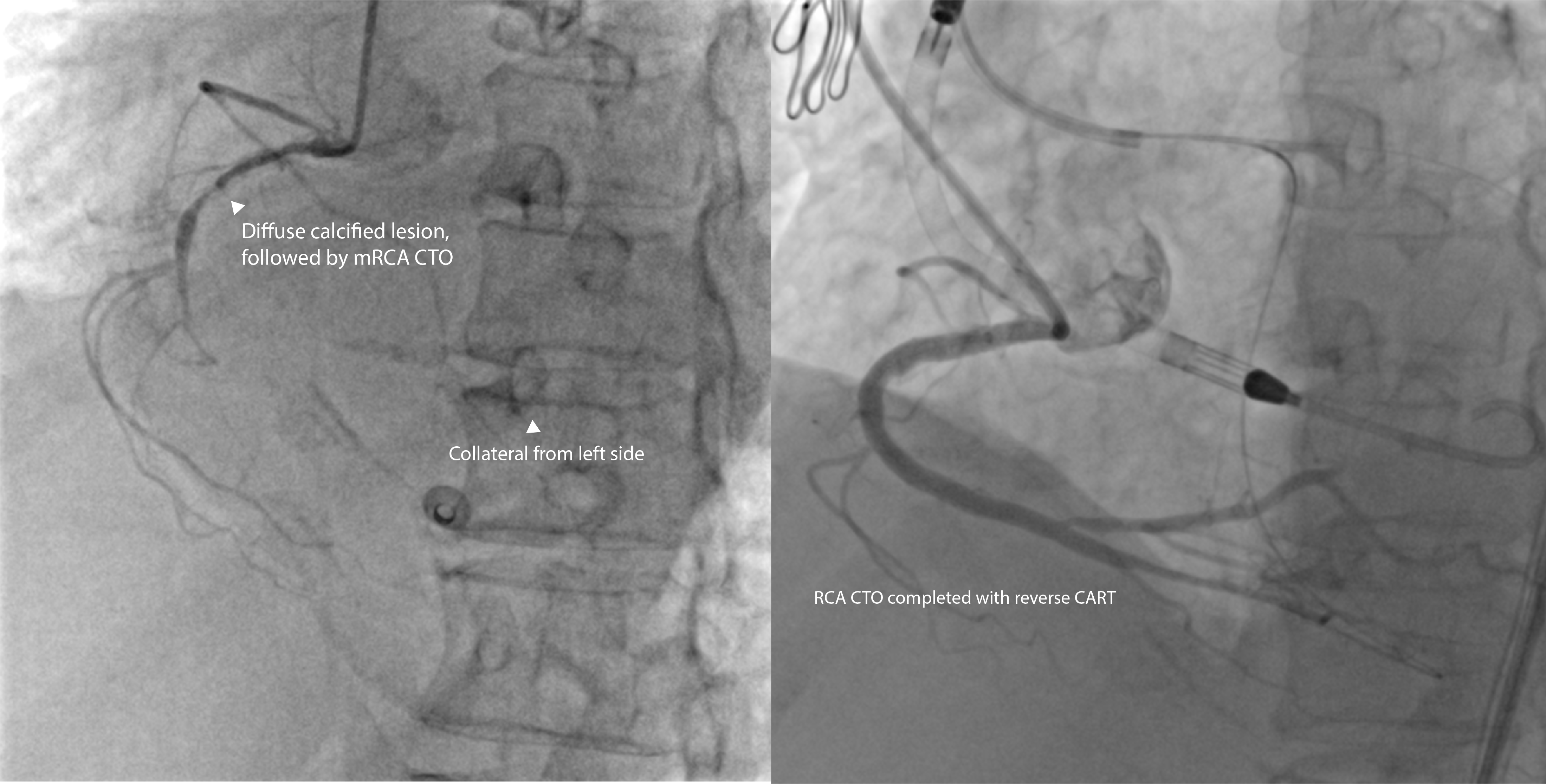
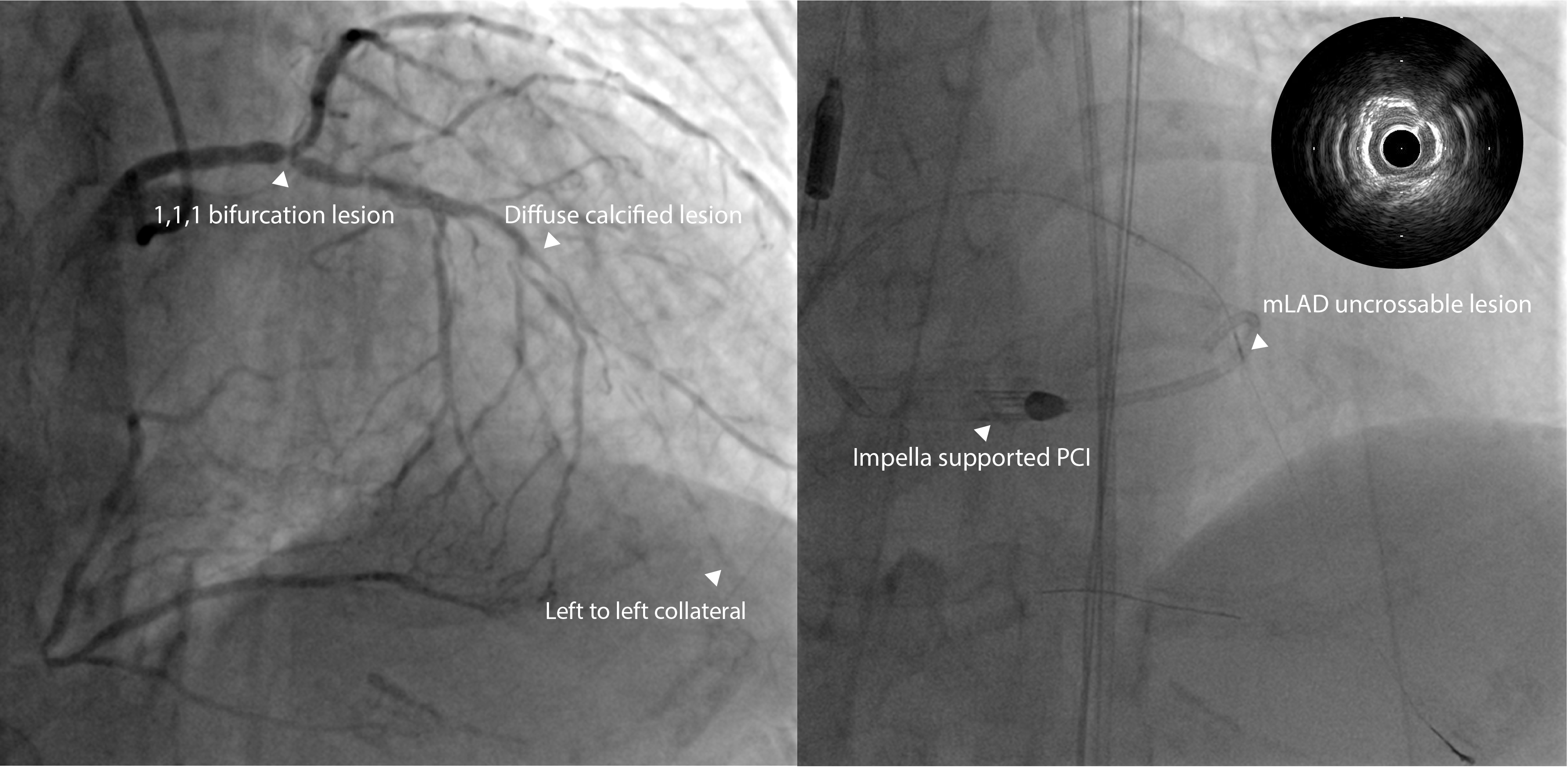
Coronary angiogram showed triple vessel disease with diffuse calcified lesion & left main bifurcation medina 1,1,1 lesion, together with chronic total occlusion over mRCA and mLAD.
Interventional Management
Procedural Step
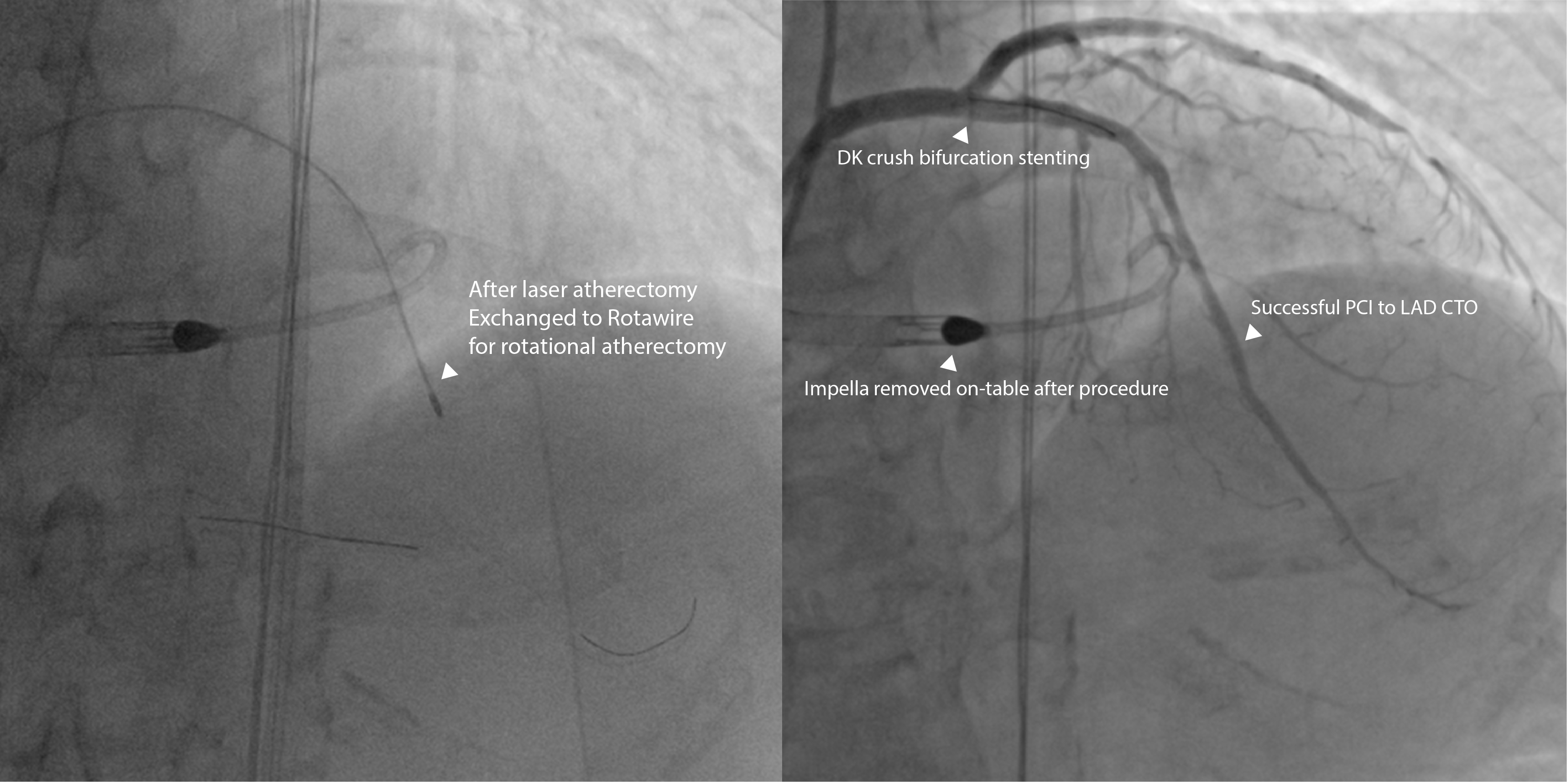
Impella was used to maintain hemodynamic stability during the procedure. PCI to RCA CTO was completely by reverse controlled antegrade and retrograde tracking (CART) technique. For the PCI to LAD CTO, we first successfully wire to distal LAD with Sion guidewire. However, there is an uncrossable mid LAD heavily calcified lesion where no balloon or microcatheter can pass through. As losing wire in distal true lumen is not preferred and difficulties anticipated in bare wiring with Rotawire. We decided for excimer laser coronary atherectomy (ELCA) over a standard 0.014 guidewire. By debulking and modifying the plaque compliance, we were able to pass through the HighTrack microcatheter to dLAD, in exchange for Rotawire. Followed by rotational atherectomy to mLAD. PCI to LM-LAD/LCx was completed with DK crush. Impella was removed on table. Patient was discharged and followed up in clinic without hospitalization for heart failure.
Case Summary
In the case of uncrossable calcified lesion, where losing wire position is unwanted or bare wiring with rotawire is difficult or impossible. Laser atherectomy could be an use tool, which is delivered on a standard 0.014 workhorse guidewire. By debulking and modifying the plaque compliance, it can facilitate the exchange of rotawire and subsequent rotational atherectomy.