
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-135
Managing Complications and Nightmare - SVG Perforation
By Raghav Sharma
Presenter
Raghav Sharma
Authors
Raghav Sharma1
Affiliation
RKM Hospitals, India1,
View Study Report
TCTAP C-135
Coronary - Complication Management
Managing Complications and Nightmare - SVG Perforation
Raghav Sharma1
RKM Hospitals, India1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
50year / Male with Hypertension LVEF 55%ACS USAS/P CABG/ 2013Triple vessel Disease - Diffused disease- LAD, LCX & RCALIMA TO LAD PATENTSVG TO Distal RCA patent consent taken for CAG and further procedure
Relevant Test Results Prior to Catheterization
Relevant Catheterization Findings
· TVD-Diffused disease- LAD, LCX& RCA
- SVG TO OM DLCX MID SEGMENT 90% Distally Near ANASTOMOSIS 80%
Interventional Management
Procedural Step
Patient was post CABG
LIMA to LAD graft was patent
SVG RCA was also Patent
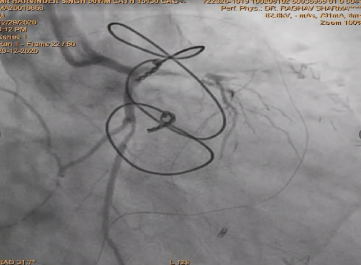
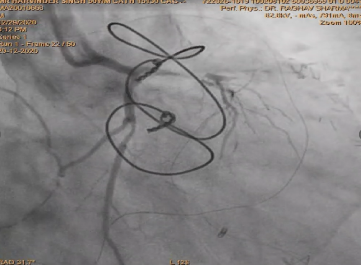
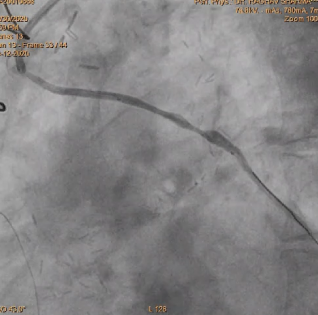
Planned SVG Stenting -OM and Distal LCX ,
stent was deployed in OM and LCX
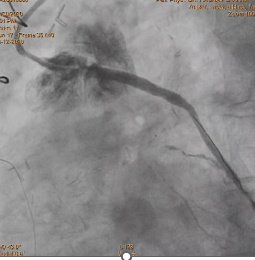
After deployment observed Perforation of SVG-OM Distal LCX post Stenting.
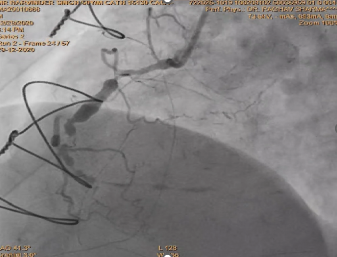
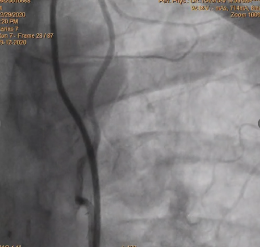
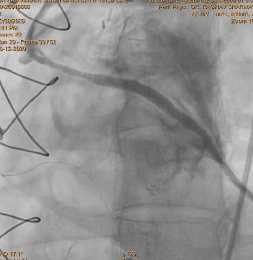
Used two covered stent to cover perforation OM and LCX .
After using covered stent perforation was sealed and TIMI 3 flow achieved
Patient was stable and all parameter was normal and discharge after two days from hospital
Case Summary
PCI to SVGs is a challenge for an interventional cardiologist and needs adequate experience and expertise. SVG perforation is a cardiac emergency and needs immediate intervention. Use of undersized stent and balloons may prevent this fatal complication without compromising short- and long-term results.