
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-084
Double CTO Intervention With Balloon Anchoring and Guide-Plus Inching Techniques
By Saurabh Mehrotra
Presenter
Saurabh Mehrotra
Authors
Saurabh Mehrotra1
Affiliation
Postgraduate Institute of Medical Education and Research, India1,
View Study Report
TCTAP C-084
Coronary - Complex PCI - CTO
Double CTO Intervention With Balloon Anchoring and Guide-Plus Inching Techniques
Saurabh Mehrotra1
Postgraduate Institute of Medical Education and Research, India1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A 60-year-old male with a history of hypertension, reformed smoking and alcohol use, and coronary artery disease presents with unstable angina. His left ventricular ejection fraction (LVEF) is 55%. Previous coronary angiography (P/CAG) reveals chronic total occlusion (CTO) in the left circumflex artery (LCX) and right coronary artery (RCA).

Relevant Test Results Prior to Catheterization
A 60-year-old male with a history of hypertension, reformed smoking and alcohol use, and coronary artery disease presents with unstable angina. His left ventricular ejection fraction (LVEF) is 55%. Previous coronary angiography (P/CAG) reveals chronic total occlusion (CTO) in the left circumflex artery (LCX) and right coronary artery (RCA).
Relevant Catheterization Findings
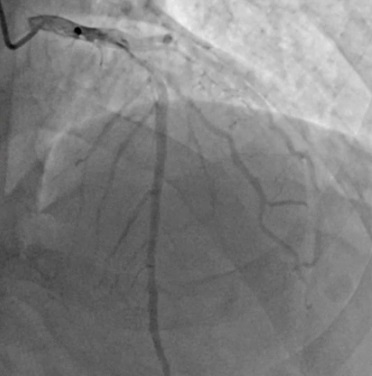
Angiography reveals- Double CTO
Interventional Management
Procedural Step
The left main (LM) artery was engaged using an EBU 3.5 6Fcatheter. Initial attempts to cross the LCX CTO with Fielder XTR and Gia 3wires were unsuccessful, prompting the use of the Balloon Anchoring Techniquewith a 1x5 mm balloon. Pre-dilatation of the lesion was performed with 1.5x10mm and 2.5x20 mm balloons. A 2.5x40 mm drug-eluting stent (DES) was deployed,followed by proximal optimization technique (POT) using a 2.75x15 mm balloon.


Case Summary
Managing double CTOs requires advanced techniques such as BAT and guidewire manipulation, especially in patients with a history of unstable angina and comorbidities. In this case, a combination of the Balloon Anchoring Technique and the Guide-Plus inching technique facilitated successful stent deployment in both the LCX and RCA. OCT imaging could be considered in future cases to enhance precision. The successful final result without complications underscores the importance of using tailored strategies for complex CTO interventions. Lifestyle modification will remain crucial for long-term outcomes, especially given the patient's history of smoking and alcohol use