
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-114
A Challenging Case Report: Primary PCI to Left Main Coronary Artery Stenosis in a Patient With Acute Coronary Syndrome [qRBBB] Post Cardiac Arrest Caused by Extrinsic Mediastinal Mass [Synovial Sarcoma] Compression
By Dasarath Boppana, Gopalakrishna K, Raghuram P, Chowdary Pss, Purnachandrarao K, Somasekhar G, Venkata R S Subrahmanya Sarma, Mounika Boppana, Ramkishore Y, Sasidhar Y, Prasad M
Presenter
Dasarath Boppana
Authors
Dasarath Boppana1, Gopalakrishna K1, Raghuram P1, Chowdary Pss1, Purnachandrarao K1, Somasekhar G1, Venkata R S Subrahmanya Sarma1, Mounika Boppana2, Ramkishore Y3, Sasidhar Y1, Prasad M1
Affiliation
Aayush Hospitals, India1, KIMS Hospitals, India2, DVC Hospitals, India3,
View Study Report
TCTAP C-114
Coronary - Complex PCI - Left Main
A Challenging Case Report: Primary PCI to Left Main Coronary Artery Stenosis in a Patient With Acute Coronary Syndrome [qRBBB] Post Cardiac Arrest Caused by Extrinsic Mediastinal Mass [Synovial Sarcoma] Compression
Dasarath Boppana1, Gopalakrishna K1, Raghuram P1, Chowdary Pss1, Purnachandrarao K1, Somasekhar G1, Venkata R S Subrahmanya Sarma1, Mounika Boppana2, Ramkishore Y3, Sasidhar Y1, Prasad M1
Aayush Hospitals, India1, KIMS Hospitals, India2, DVC Hospitals, India3,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
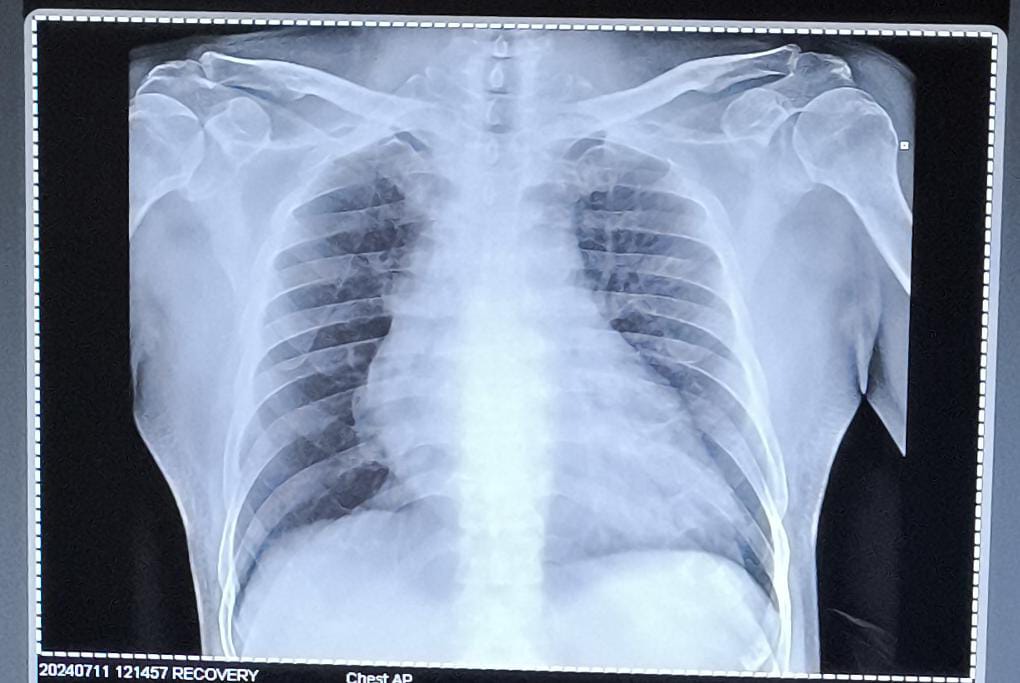
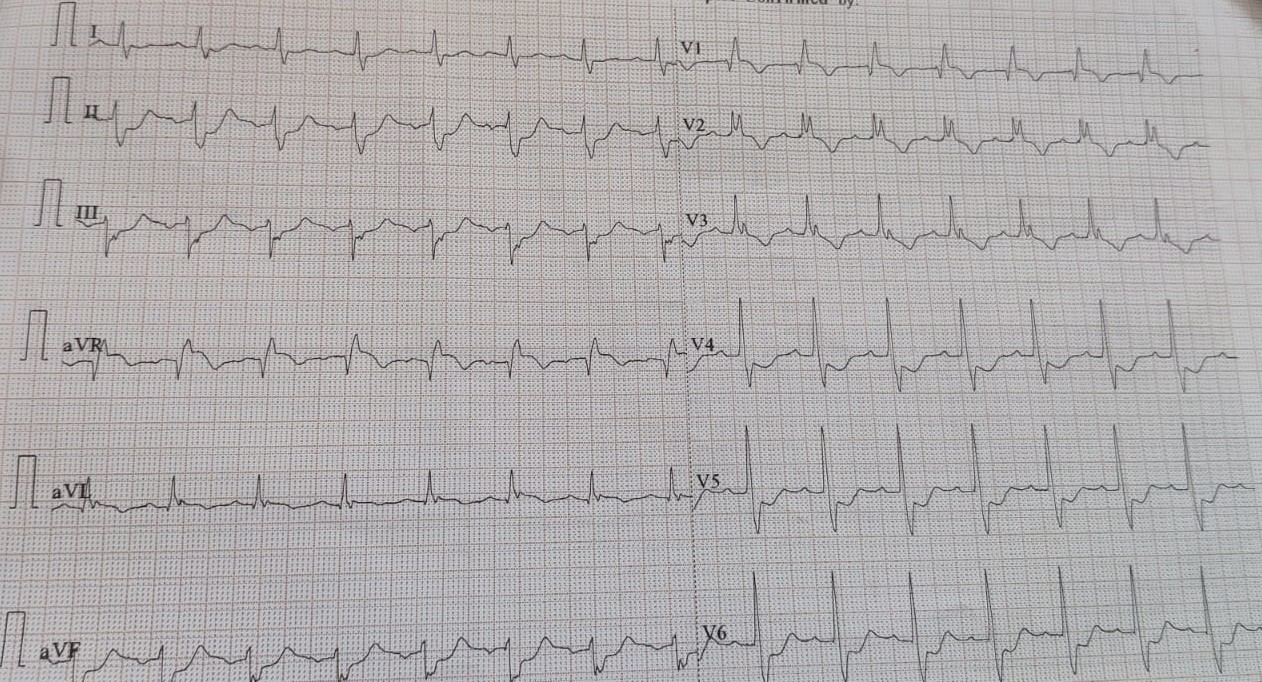
A 53 year old male patient presented to us with on and off chest pain since 1 week aggravated since 1 hour.Patient is known diabetic,hypertensive and CAD ,chronic stable angina post PTCA to mid LAD ,distal RCA and DCB to distal LAD ,PDA and PLVB 3 months back. Patient presented in cardiogenic shock and had a cardiac arrest and ROSC was attained after resuscitation and patient was shifted to cath lab for further management.ECG revealed QRBBB.X ray chest revealed mediastinal widening.
Relevant Test Results Prior to Catheterization
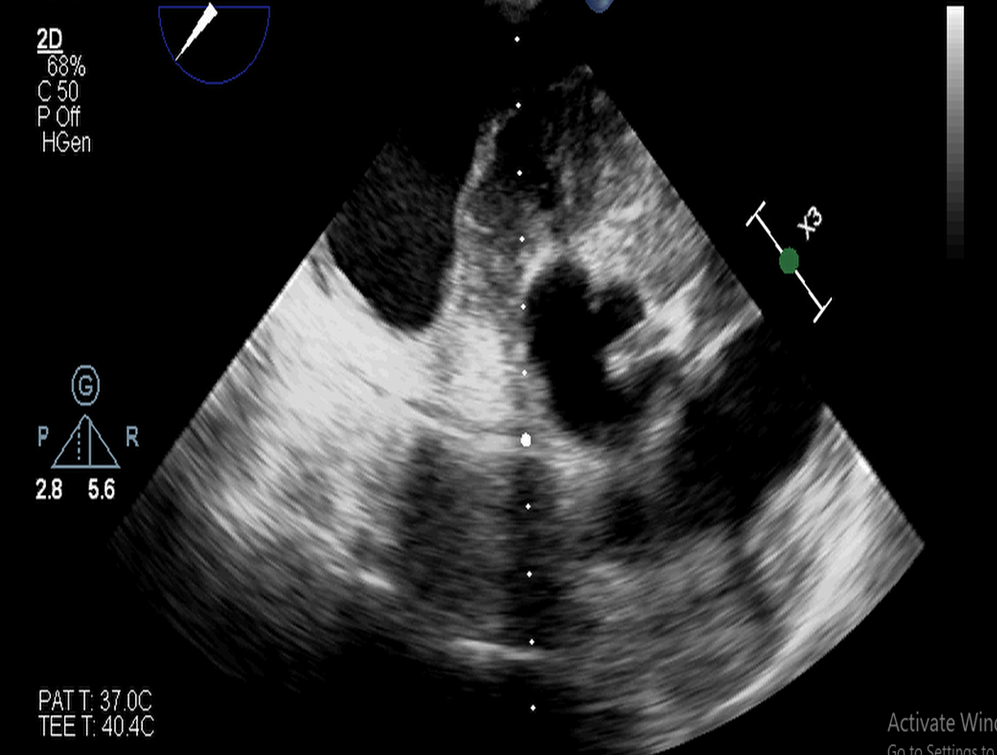
ECG revealed QRBBB.Echo revealed RWMA in LAD territory with mild LV dysfunction with moderate tricuspid reguirgitation and moderate pulmonary arterial hypertension.A mass was noted in modified views in ? left atrium in parasternal long axis view and short axis view compressing the aortic root in transthoracic echocardiogram.

Relevant Catheterization Findings
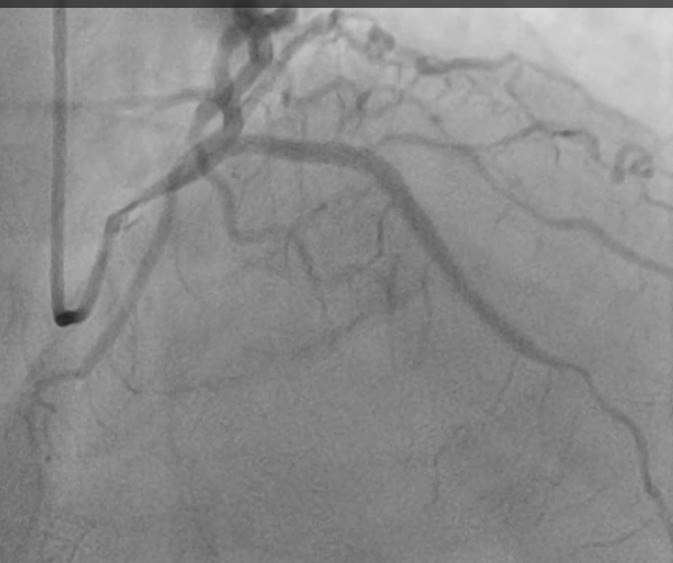
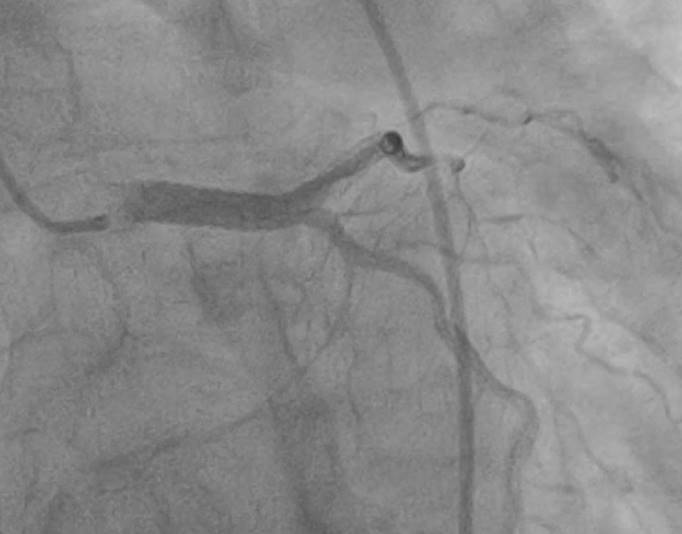
Coronary angiogram done revealed critical ostial left main coronary artery stenosis [left main disease not present during left coronary intervention done 5 months back].LAD and LCX wired and ostial LM predilated with 3x 15 mm NC balloon @ 16 atms. Later LM TO LAD stented with 3.5 x 38 mm drug eluting stent @ 10atms, ostial flaring done with same stent balloon @ 12 atms. Pot done with 4.5x 10 mm NC balloon @ 18-20 atms.LAD postdialated with 3.5X15 NC balloon@14-18atm.TIMI III flow noted.

Interventional Management
Procedural Step
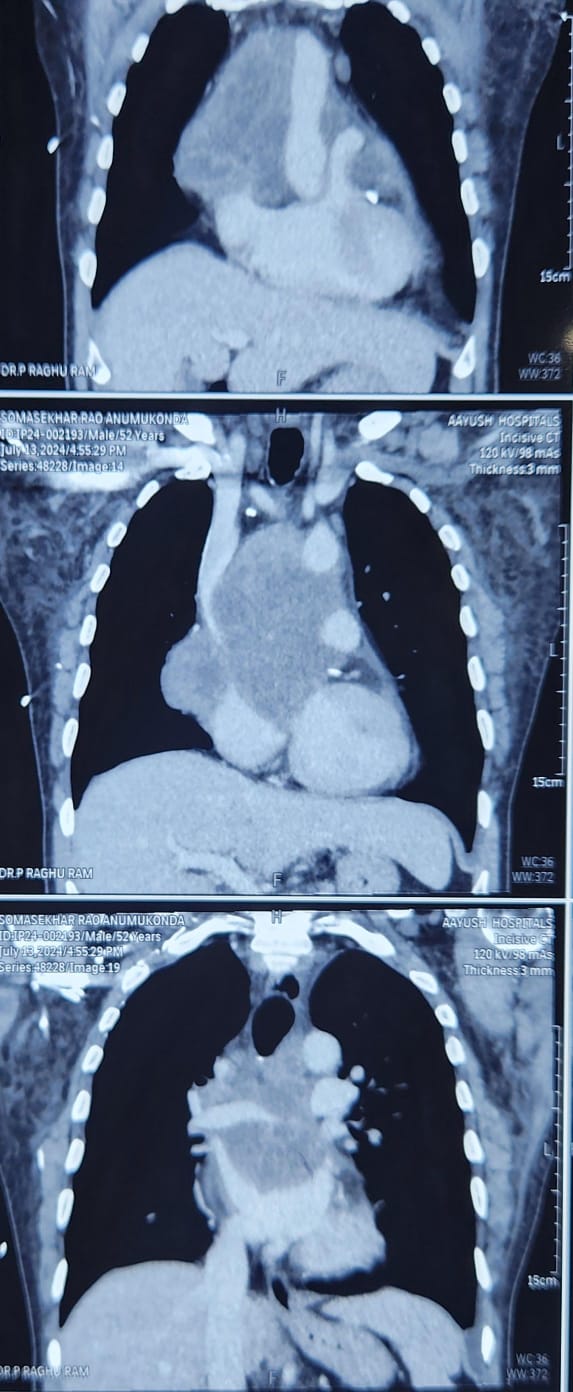
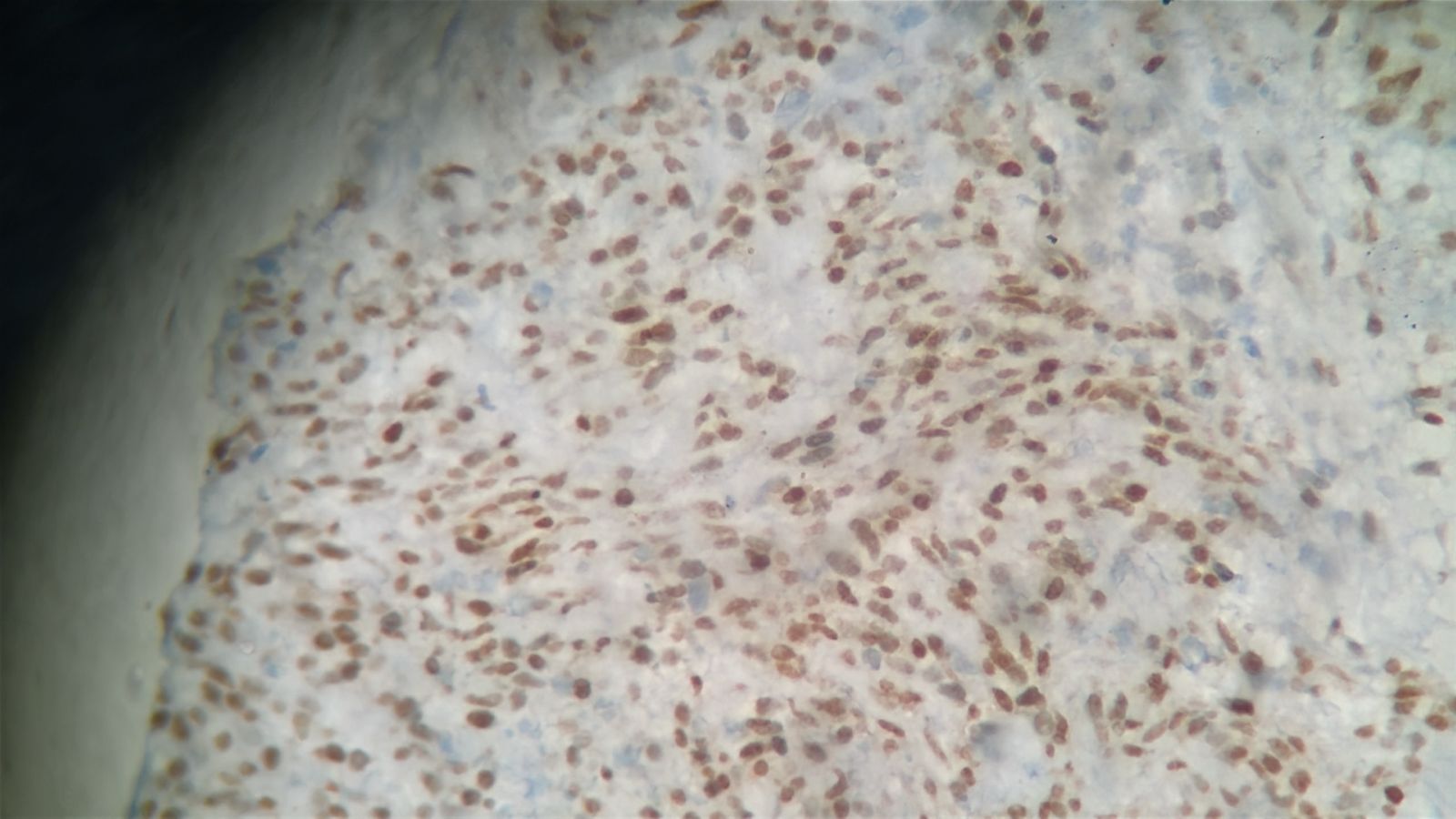
However in view of suspicion of extrinsic mediastinal mass compression of left main coronary artery ,transesophageal echocardiogram was done which revealed large mediastinal mass extending into aortic root compressing the left main coronary artery with left main stent extending in aorta ,preventing the mass from compression .CECT examination of thorax revealed large mediastinal tumour 11.3X9.3cm encasing the ascending thoracic aorta and aortic arch and obstructing the right pulmonary artery and also compressing the left atrium.FDG PET CT scan was done which revealed large multilobulated heterogenous mass in the middle mediastinum probably arising from the pericardium.He was stabilized and after optimising coagulation parametres,high risk CT guided biopsy was done and IHC of the specimen is suggestive of synovial sarcoma[spindle cell tumour].Transesophageal echo and CECT and IHC slides enclosed.
Case Summary
The clinical manifestation of Synovial sarcoma from pericardium are varied with most common being constrictive pericarditis,pulmonary embolism,cardiac tamponade and heart failure caused by myocardial infiltration.Compression of left main coronary artery is extremely rare finding.And also mediastinal tumour causing acute coronary syndrome causing QRBBB and cardiac arrest is extremely rare.To our knowledge this is one of the rare case presentations where primary PCI in left main coronary artery is done in patient with ACS[QRBB] and cardiac arrest caused by mediastinal mass compressing the left main coronary artery as a life saving effort.Currently the patient is undergoing chemotherapy.