
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-047
Double Lumen Catheter Facilitated Reverse Wire Technique for Bifurcation Lesion
By Kuan-Chieh Tu, Yu-Chieh Weng
Presenter
Yu-Chieh Weng
Authors
Kuan-Chieh Tu1, Yu-Chieh Weng1
Affiliation
Chi-Mei Medical Center, Taiwan1,
View Study Report
TCTAP C-047
Coronary - Complex PCI - Bifurcation
Double Lumen Catheter Facilitated Reverse Wire Technique for Bifurcation Lesion
Kuan-Chieh Tu1, Yu-Chieh Weng1
Chi-Mei Medical Center, Taiwan1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
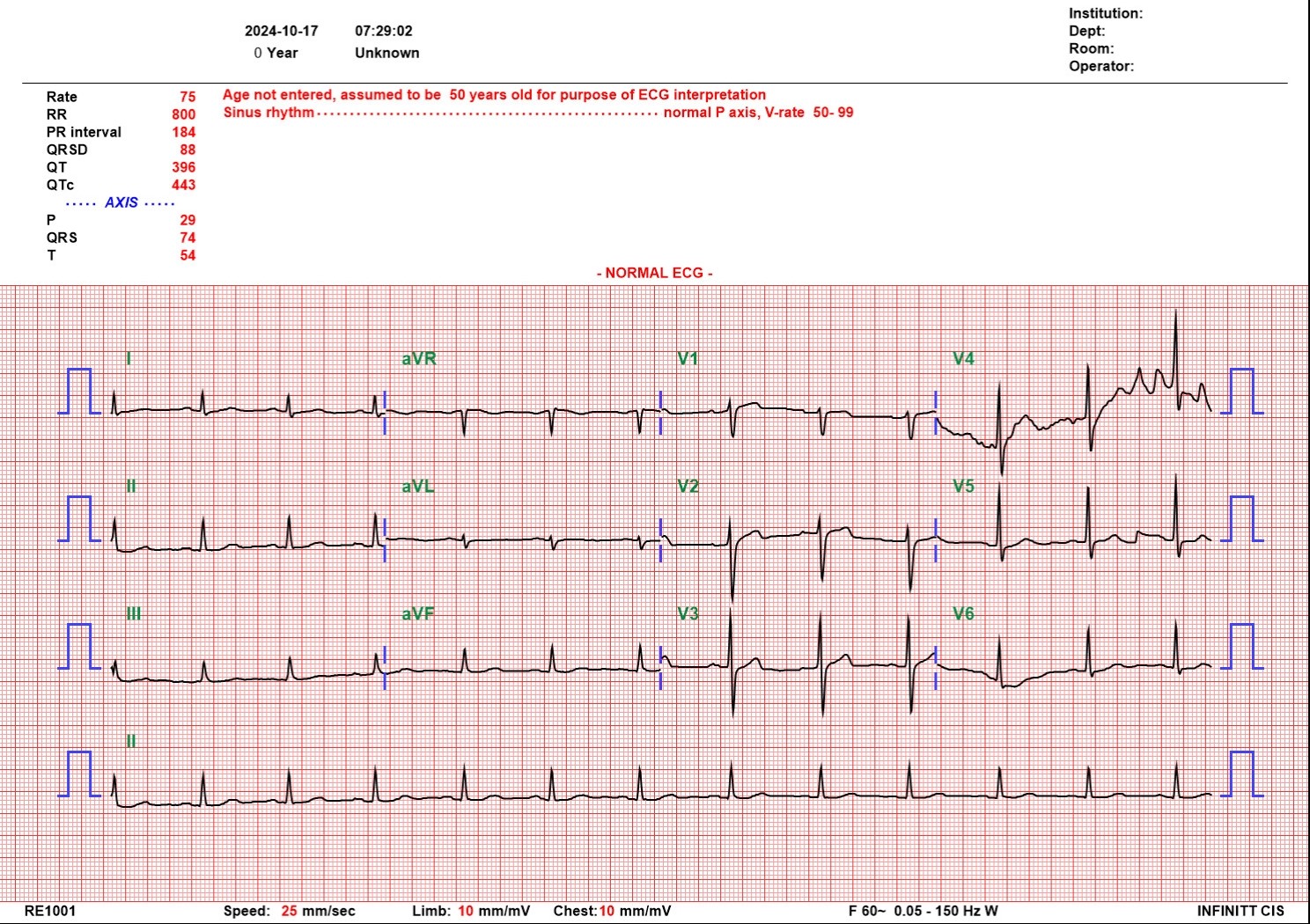
41-year-old male without underlying diseases except smoking presented with intermittent chest pain. Initial vital sign was stable. Physical examination showed no audible murmur and warm extremities. EKG showed no specific ST segment change. Cardiac enzyme was mildly elevation. NSTEMI was diagnosed with GRACE score 51 points.
Relevant Test Results Prior to Catheterization
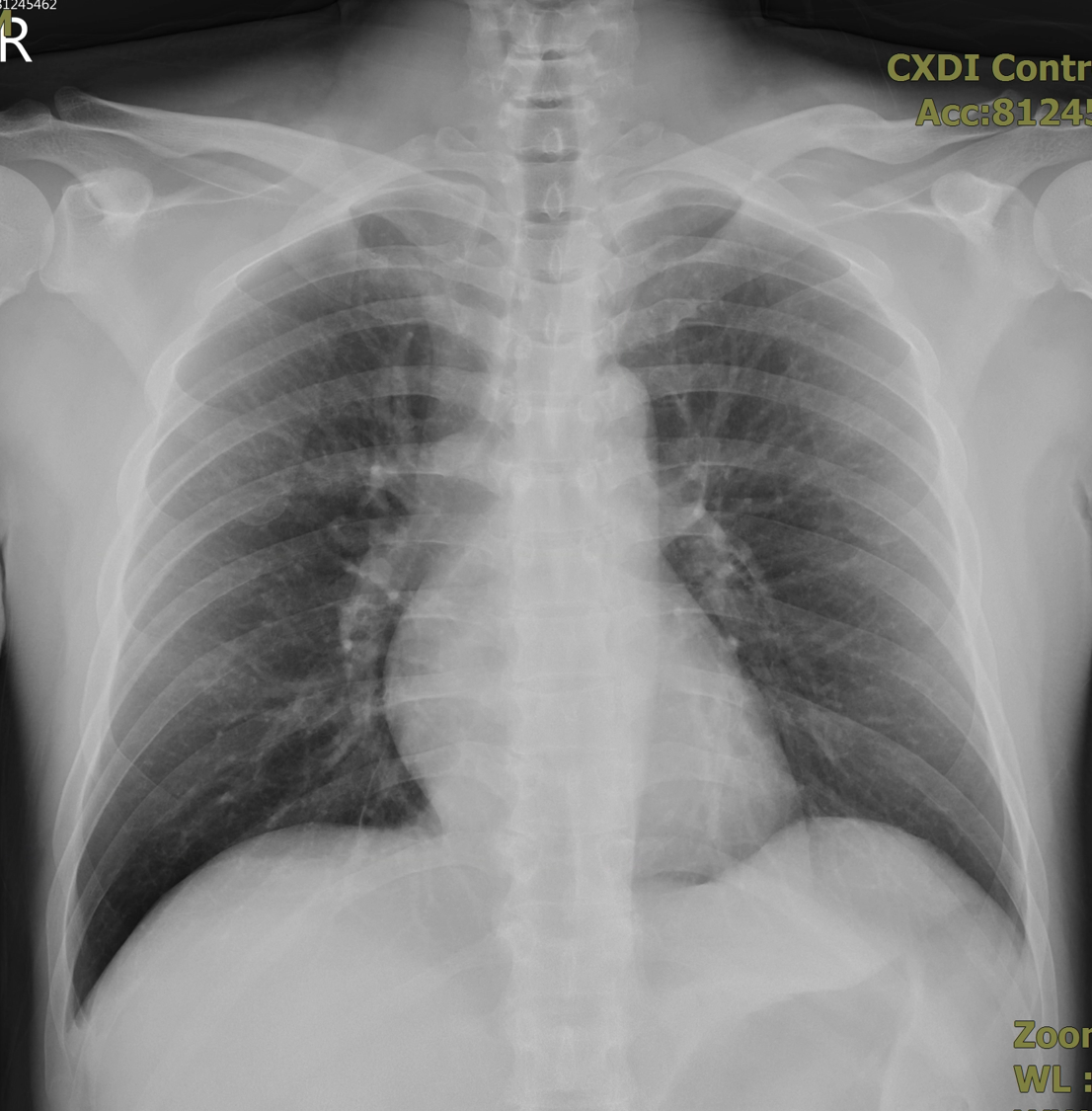
EKG showed no specific ST segment change. Cardiac enzyme was mildly elevation. Chest X ray showed no cardiomegaly or pulmonary edema.
Relevant Catheterization Findings
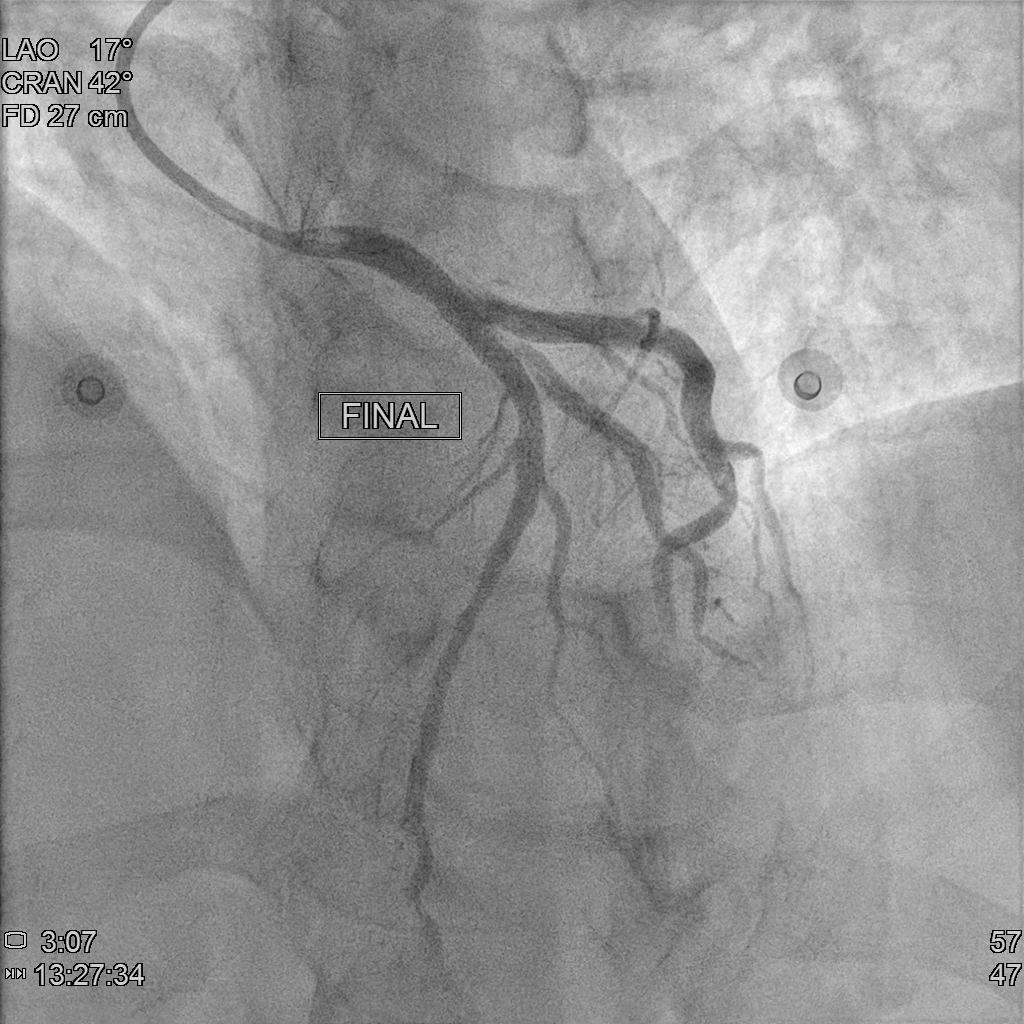
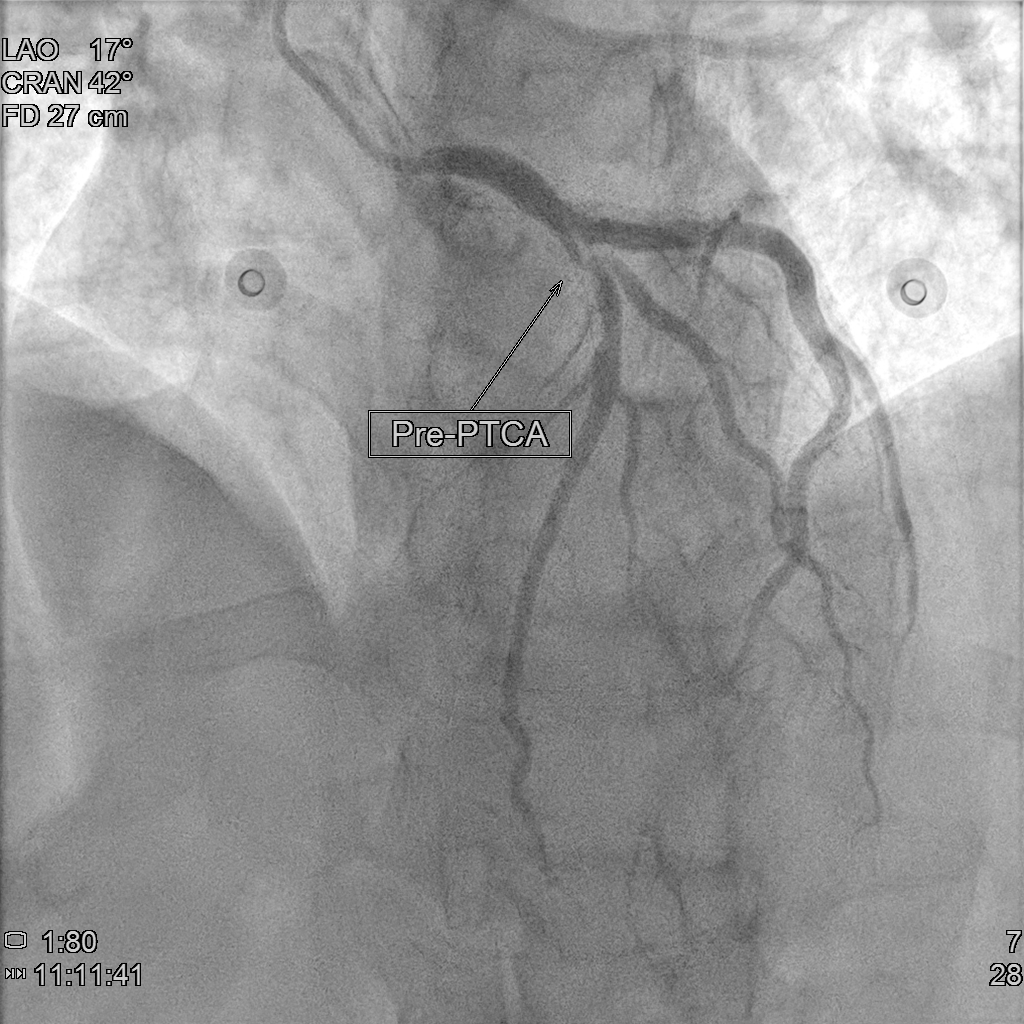
Coronary angiography showed CAD(1-V-D), with medina 1.1.1 bifurcation lesion at LAD-P and LAD-D1. We decided to performed provisional stenting strategy. We accidentally retracted the jailed wire after MV pre-dilation and TIMI flow of SB decreased to TIMI 1. It was difficult to rewire to SB due to acute take off angle after MV pre-dilation, so we performed DLC facilitated RWT. After that, we performed DK crush technique for the bifurcation lesion. The final angiography looks good.
Interventional Management
Procedural Step
Under support of Boston JL3.5,6Fr via Left Radial Artery approach, we introduced Floopy wire to LAD-D and Pilot 50 wire to LAD-D1. We dilated the 99% stenosis of LAD-M and LAD-P with Trek 2.5x20mm to 10 ATM. We checked the the intracoronary artery condition with IVUS and revealed severe stenosis and massive plaque burden in LAD-P to M and the lesion lenght of LAD-D1 orifice was 4.31mm with severe stenosis. After image evaluation, we used NC Trek 3.5x20mm to 12 ATM for predilatation, however, we incidentally retracted the LAD-D1 wire and we found that the flow of LAD-D1 became worse due to carina and plaque shift. It is challenging for direct wire and thus we perfomred reverse wiring technique with double lumen catheter (Crusade R). After that, we perfomred two stent strategy with DK crushing technique. We predilated the LAD-D1 with Trek 3.0 x15mm to 12 ATM. Then we deployed (NEW)SYNERGY XD 3.0 x20mm to LAD-D1, and crushed it with NC Trek 3.5x20mm to 12 ATM. Then we used CONQUEROR康克爾 4.0 x20mm to 20 ATM for POT followed by first kissing ballon technique with NC Trek 3.5x20mm to LAD and Trek3.0 x15mm to LAD-D1 to 8 ATM. After that, we deployed (NEW)SYNERGY XD 3.5x48mm to 12 ATM at LM to LAD-M. We performed POT with NC Trek 4.5x 8mm to 12 ATM followed by second KBT with the same balloones used during first KBT. We check the IVUS and performed the final POT with Trek 5.0 x12mm to 20 ATM due to malapposition noted at proximal site of stent. The final angiography looks good.
Case Summary
We used the Definition criteria to define the complexity of bifurcation lesion. Provisional stenting strategy is suitable for simple bifurcation lesion, in contrast, complex bifurcation lesion should be treated with two stent strategy, especially DK crush technique. On the other hand, when we encountered bifurcation lesion with acute take off angle, double lumen catheter facilitated reverse wire technique should be take into consideration.