
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-037
A Seventy-Six-Year-Old Man Undergoing Coronary Intervention With Intravascular Lithotripsy Balloon Rupture
By Yi-Hong Tseng, Po-Chih Lin
Presenter
Yi-Hong Tseng
Authors
Yi-Hong Tseng1, Po-Chih Lin1
Affiliation
National Taiwan University Hospital, Taiwan1,
View Study Report
TCTAP C-037
Coronary - Adjunctive Procedures (Thrombectomy, Atherectomy, Special Balloons)
A Seventy-Six-Year-Old Man Undergoing Coronary Intervention With Intravascular Lithotripsy Balloon Rupture
Yi-Hong Tseng1, Po-Chih Lin1
National Taiwan University Hospital, Taiwan1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A 76-year-old retired professor with underlying hypertension, dyslipidemia and coronary artery disease for which he had experienced coronary interventions several times from 2002 to 2022. However, he started to feel intermittent chest tightness after walking for 3 - 5 minutes in recent months along the follow-up at the outpatient clinic. He did not present orthopnea or pitting edema physically.

Relevant Test Results Prior to Catheterization
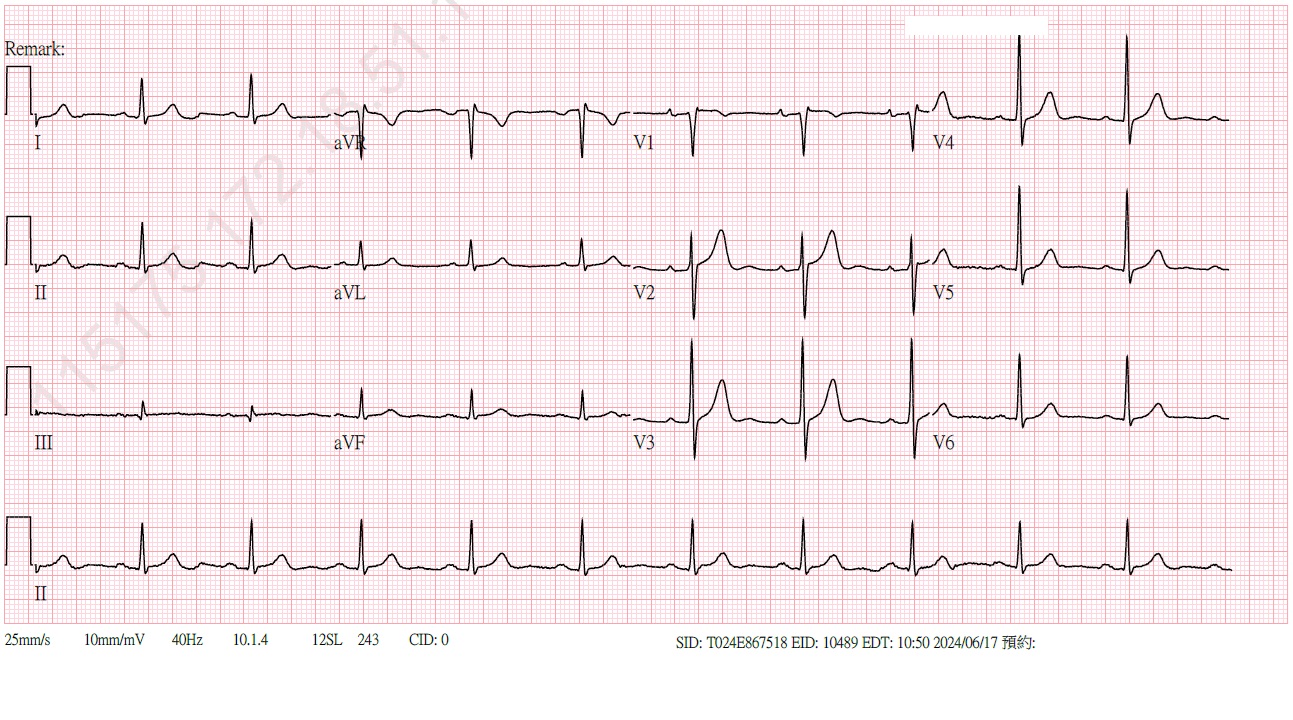
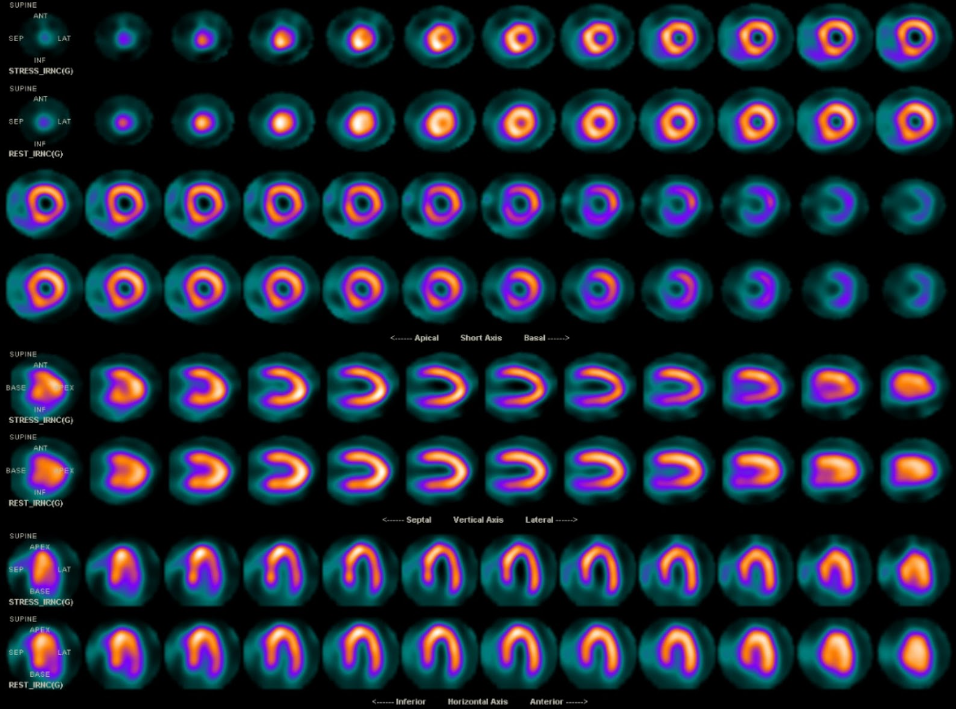
The ECG displayed normal sinus rhythm. The thallium scan presented mild stress-induced ischemia in the apical lateral and middle inferolateral walls. The laboratory data showed hemogram within normal range, normal liver and kidney function.
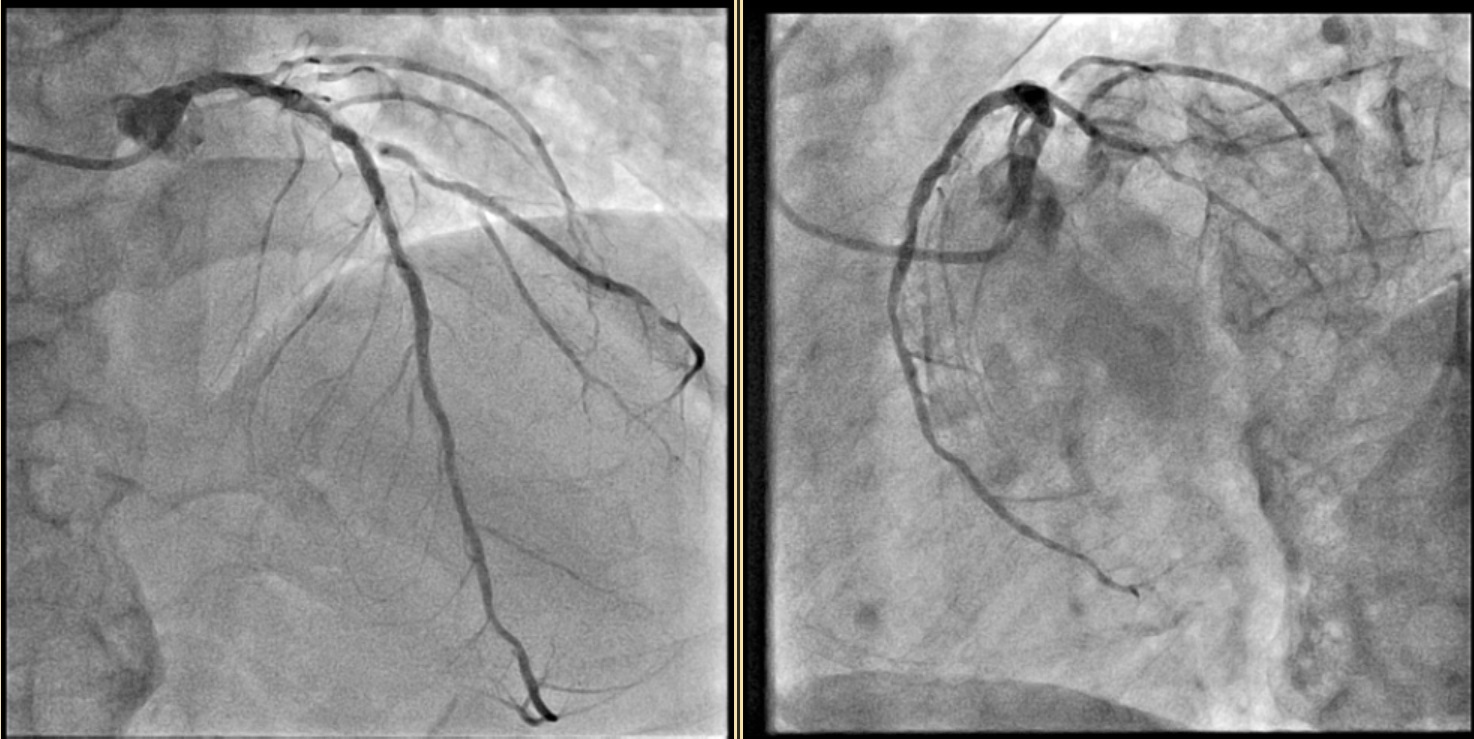
Relevant Catheterization Findings
LM: shaft stenosis 50 %; LAD: D1 ISR 90 %, proximal diffuse ISR 70 %, middle ISR 60 %; LCX: ostial stenosis 80 %, hypoplasia; RCA: ostial-proximal ISR 70 %, middle ISR 70 %, distal stenosis 30 %, PDA stenosis 80 %


Interventional Management
Procedural Step
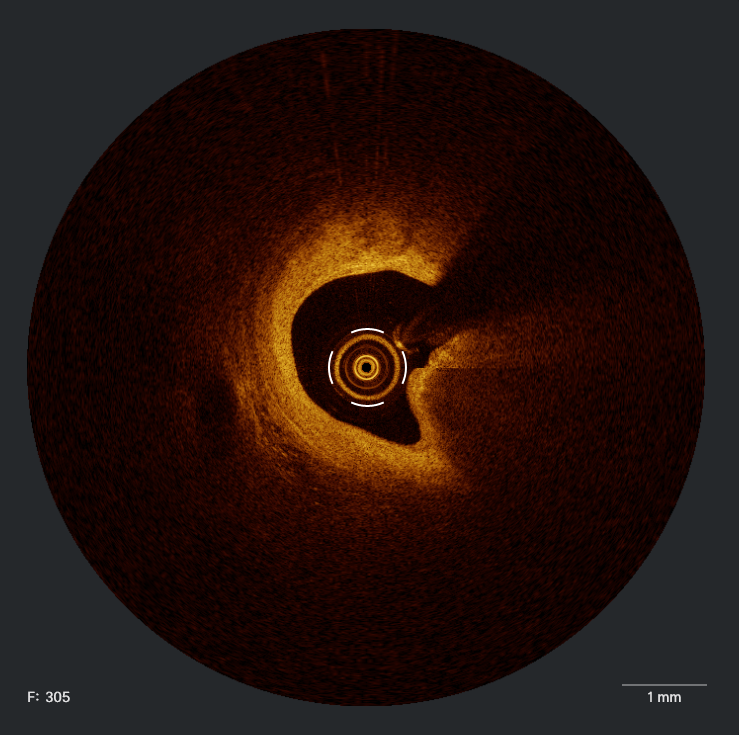
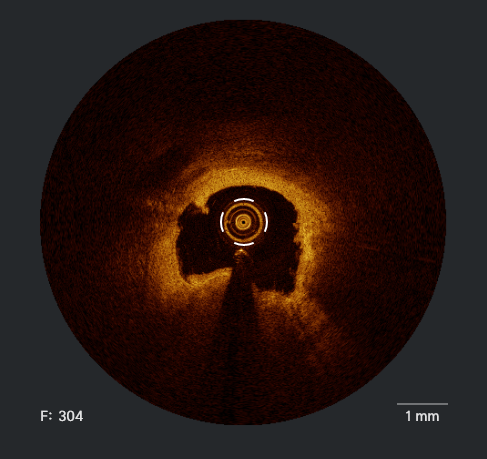
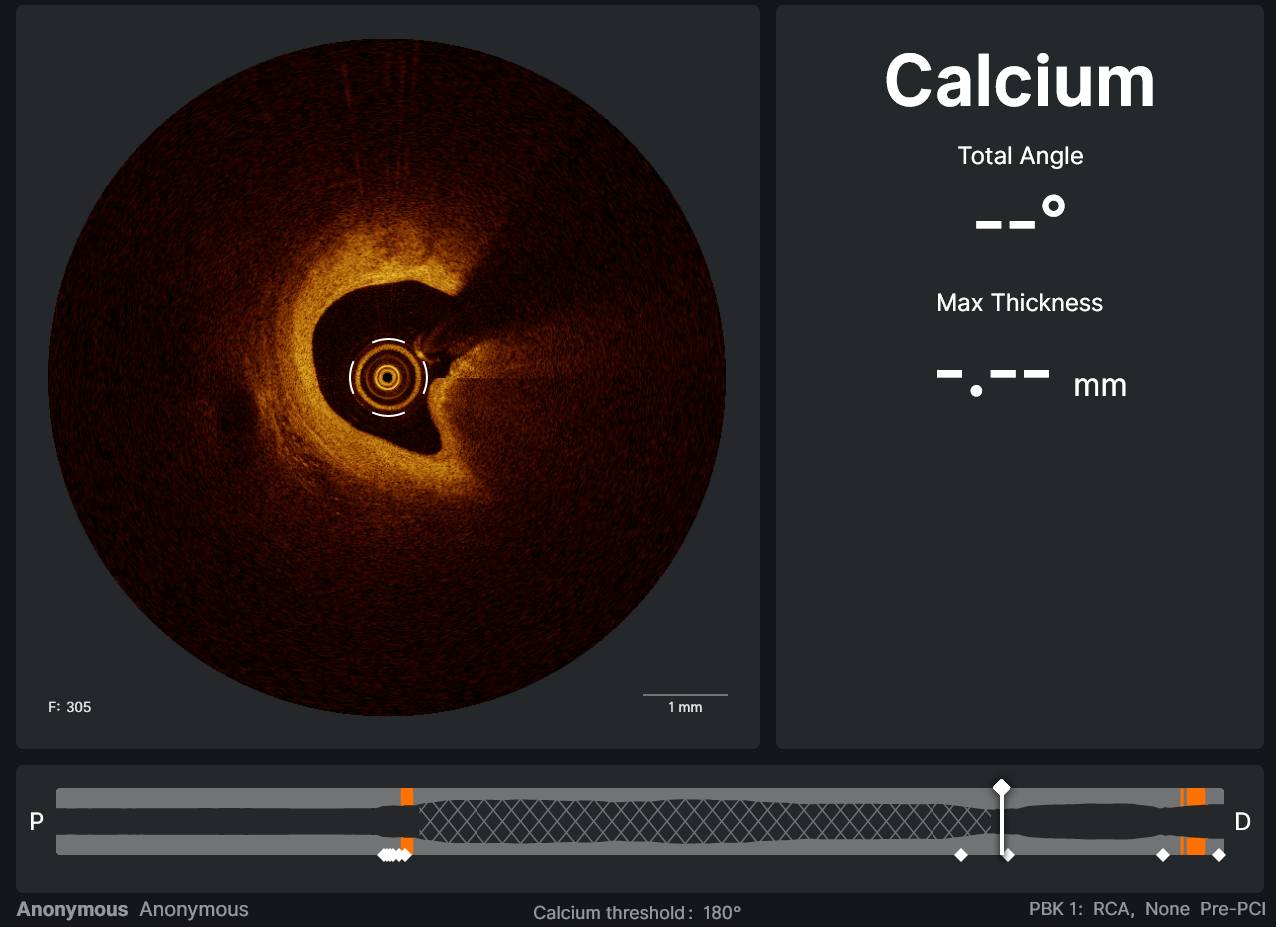
The procedure was initiated via LRA puncture and significant pressure gradient was measured while performing diagnostic CAG at RCA. Therefore we engage the RCA with “ Medtronic JR4 SH 7F ” and wired to dRCA with “ ASAHI Sion ”. Then we acquired the intracoronary image with “ LightLab / St.Jude OCT imaging catheter ” which revealed fibrocalcific plaque both inside and outside the stent with prominent neo-intimal hyperplasia. Lesion at the distal stent edge mRCA was cracked after 20 shots of “ Abbott SHOCKWAVE C2 Coronary Intravascular Lithotripsy (IVL) Catheter 3.5 mm x 12 mm ” so we pulled back the balloon to the ostial-proximal ISR. Somehow the balloon failed to be inflated at the proximal RCA and there was blood within the balloon catheter which suggested balloon rupture. While reviewing the intracoronary image, there was a protruding calcified nodule at the distal edge of mRCA stent which we assumed to cause the rupture. Consequently, rotational atherectomy with “ Boston Scientific ROTAPRO Burr Catheter and Advancing Device 2.00 mm “ was performed at RCA in order to “ polish ” the lesion and prevent further balloon rupture. Eventually, the patient tolerated IVL, stent deployment and post-dilation well. The intracoronary image also suggested well apposition and expansion of the stent when angiography yielded TIMI III blood flow. Intervention was also delivered at LCA without significanadverse events. The patient was discharged on the next day of the procedure.
Case Summary
This case demonstrated a 76-year-old man with repeated in-stent restenosis of complexed pathology which required coordination of different devices. Sharp or protruding calcified lesions might create concentrated force on the surface of the balloon and result in laceration or unexpected rupture of the balloon. Intracoronary image remains crucial to reduce the procedural risk and analyze the possible mechanism for further study.