
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-102
A Difficult CTO Case: Intravascular Ultrasound-Guided Wiring via Antegrade Approach in Right Coronary Artery
By Chi Wing Yam, Wai Lun Mak, Tsz Ho Chan, Lap Shing Chan, Shung Yee Wong, Chi Wing Wong
Presenter
Chi Wing Yam
Authors
Chi Wing Yam1, Wai Lun Mak1, Tsz Ho Chan1, Lap Shing Chan1, Shung Yee Wong1, Chi Wing Wong1
Affiliation
Pok Oi Hospital, Hong Kong, China1,
View Study Report
TCTAP C-102
Coronary - Complex PCI - CTO
A Difficult CTO Case: Intravascular Ultrasound-Guided Wiring via Antegrade Approach in Right Coronary Artery
Chi Wing Yam1, Wai Lun Mak1, Tsz Ho Chan1, Lap Shing Chan1, Shung Yee Wong1, Chi Wing Wong1
Pok Oi Hospital, Hong Kong, China1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
Mr. Mok, 63-year-old gentleman, who is a chronic smoker and drinker and had past medical history of hypertension and hyperlipidemia, presented to medical department for unstable angina, characterised by increased exertional chest pain for months and improved with rest. Physical examination reviewed stable hemodynamics (BP 131/83 mmHg), unremarkable chest and abdominal examinations. No heart murmur is heard and there is no lower limb edema.
Relevant Test Results Prior to Catheterization
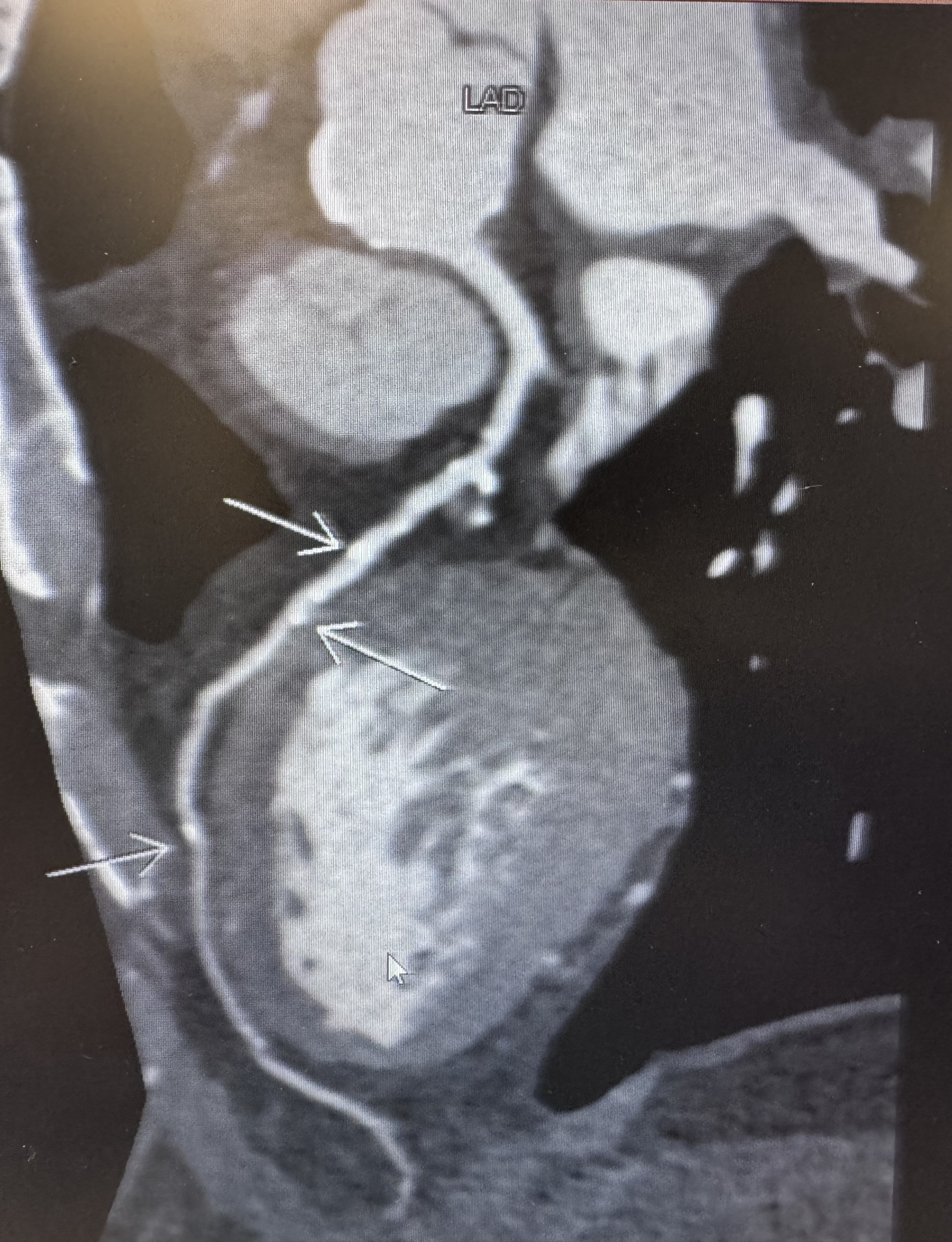
Serum hemoglobin level was 12.9 g/dL with high MCV. LDL-c was 1.3 mmol/L and A1c was 4.9%. Liver and renal function tests were normal; Iron profile was unremarkable while ferritin was elevated (4596pmol/ L). Electrocardiogram showed sinus rhythm with first degree heart block. Chest X ray showed clear lung without congestion. CT coronary angiogram showed severe proximal, mid and distal RCA, moderate proximal and mid-LAD, severe proximal and distal LCx stenoses.

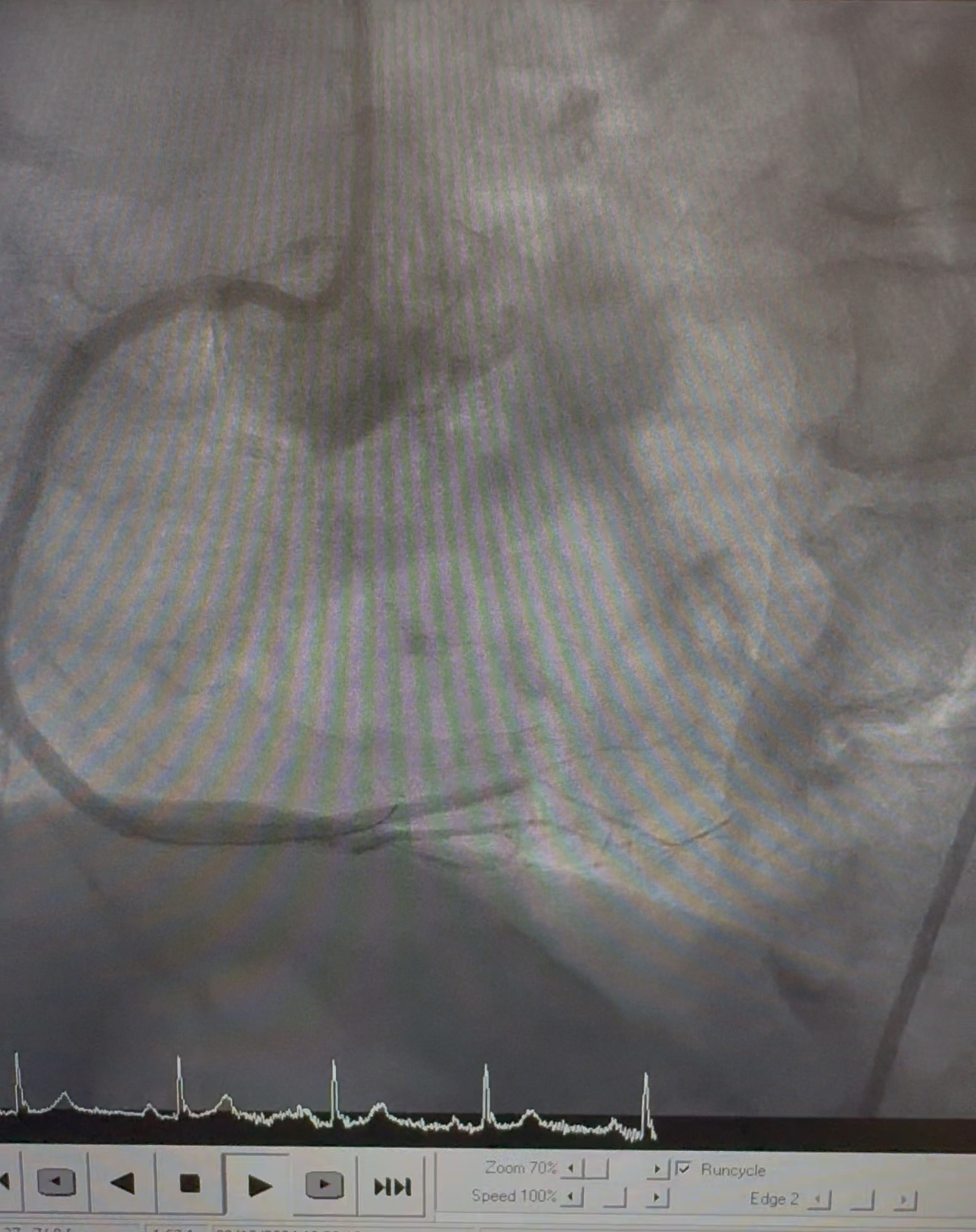
Relevant Catheterization Findings
Coronary angiography reviewed right dominant system; normal left main coronary artery, mild to moderate LAD stenosis, mild LCx stenosis and distal RCA CTO with collaterals supplying from left system.
Interventional Management
Procedural Step
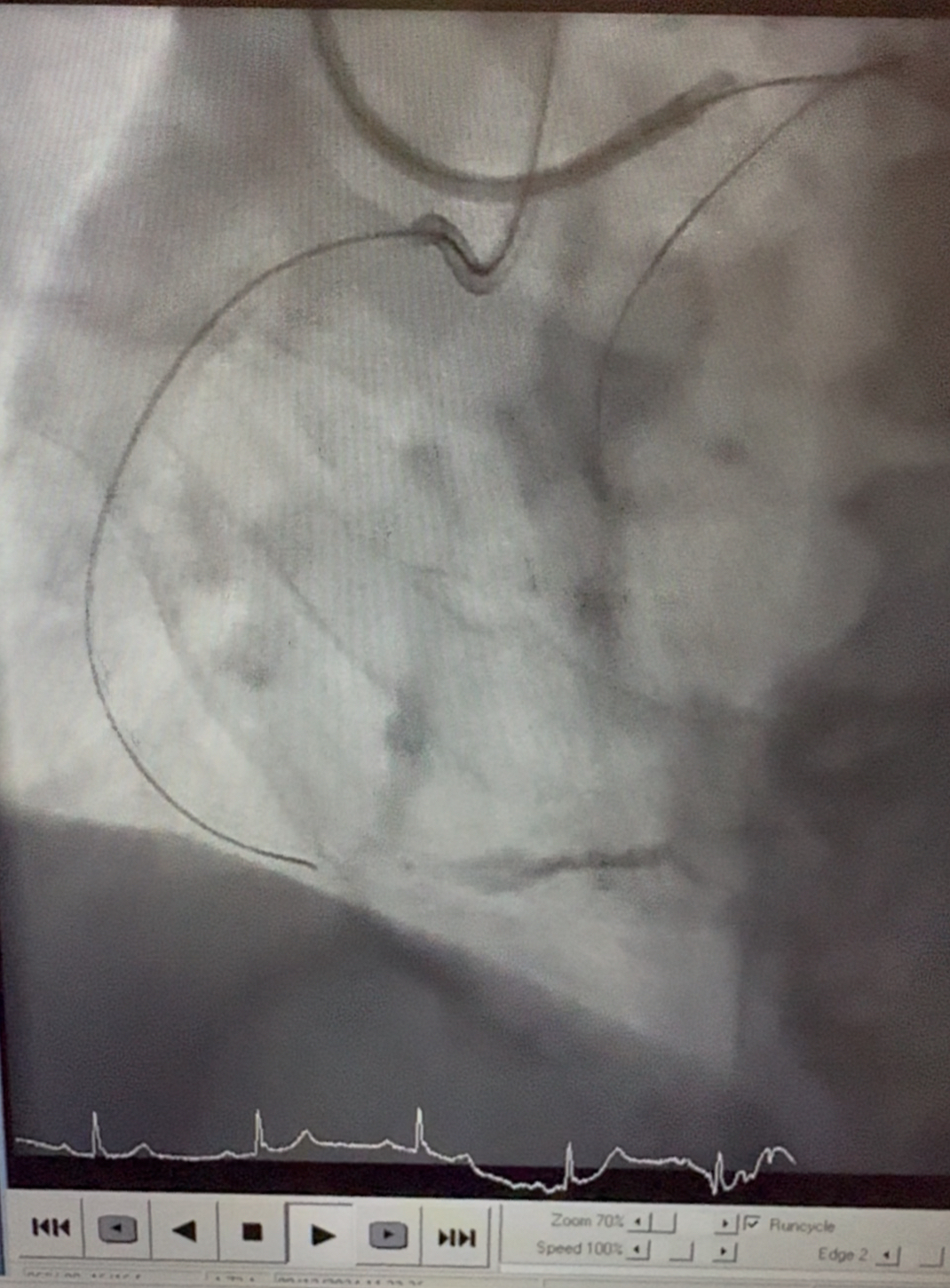
Right radial access approach was used for retrograde and right femoral access approach was used for antegrade approach. RCA was engaged with 7-Fr AL1 guiding catheter and left main coronary artery (LMCA) was engaged with 7-Fr EBU 3.5 guiding catheter. RCA CTO was failed to be crossed despite multiple wiring attempts with Gaia Next 2, UB3, Giadius MG14 and Gaia Next 3 guide wires. Retrograde flow deterioration was noted due to hematoma on angiography. Retrograde wiring attempt via septal branches was decided. Fielder XT-A and SUOH3 were used for retrograde wiring but septal branch failed to be crossed due to excessive tortuosity. Afterwards, under IVUS-guided wiring, Gaia Next 2 was successfully wired to distal PL. Gaia Next 2 was exchanged with Runthrough NS followed by predilatation with Sapphire 3 balloon (0.85mm/ 10mm) and Ryurei balloon (1.5mm /15mm). IVUS-guided wiring eventually confirmed true lumen and evidence of intramural hematoma. Further predilatation were performed Lacrosse Aperta NSE scoring balloon (2.25mm /13mm). Orsiro Mission stent (2.25mm/ 40mm) was deployed over posterolateral (PL) branch and distal RCA. Another Orsiro Mission stent (3.0mm/ 40mm) was deployed over mid-to-distal RCA; followed by deployment of another Orsiro Mission stent (3.5mm/ 40mm) over proximal RCA. High-pressure post-dilatation were done with NC Sapphire 24 balloon (3.0mm/ 15mm) and NC Trek NEO balloon (3.5mm/ 15mm). Final IVUS and angiographic result satisfactory with TIMI3 flow.
Case Summary
IVUS-guided wiring identified the presence of intramural hematoma and confirmed entrance of guidewire into true lumen after crossing CTO body in this case; which eventually aided the CTO PCI and avoid deterioration of intramural hematoma. Despite several possible drawbacks identified, including increased risk of perforation due to expansion of subintimal space by balloon dilatation; difficulty to correlate between the relative position of guidewire and true lumen and the corresponding angiography; and difficulty to manipulate extra guidewire, IVUS-guided wiring still serves as important alternative approach for tackling CTO lesions and avoiding conversion of revascularization to CABG.