
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-025
Recurrent Acute Total Occlusion of the Right Coronary Artery Managed With Thrombus Aspiration and Stenting: A Case Report With Discussion on Revascularization Strategies
By Mohd Aizuddin Mohd Zulastri, Muhammad Azlan Aseri, Syed Saleh Syed Sheikh, Ahmad Syadi Mahmood Zuhdi, Imran Zainal Abidin
Presenter
Mohd Aizuddin Mohd Zulastri
Authors
Mohd Aizuddin Mohd Zulastri1, Muhammad Azlan Aseri1, Syed Saleh Syed Sheikh2, Ahmad Syadi Mahmood Zuhdi1, Imran Zainal Abidin1
Affiliation
University Malaya Medical Centre, Malaysia1, International Islamic University Malaysia, Malaysia2,
View Study Report
TCTAP C-025
Coronary - ACS/AMI
Recurrent Acute Total Occlusion of the Right Coronary Artery Managed With Thrombus Aspiration and Stenting: A Case Report With Discussion on Revascularization Strategies
Mohd Aizuddin Mohd Zulastri1, Muhammad Azlan Aseri1, Syed Saleh Syed Sheikh2, Ahmad Syadi Mahmood Zuhdi1, Imran Zainal Abidin1
University Malaya Medical Centre, Malaysia1, International Islamic University Malaysia, Malaysia2,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
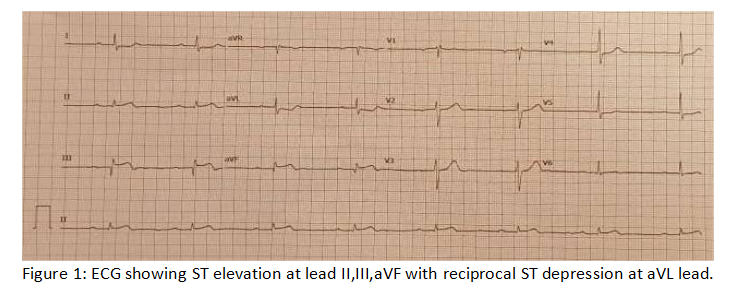
An 81-year-old man was diagnosed with acute inferior STEMI(Figure 1) with stable vital sign. Angiogram showed RCA occlusion(TIMI 0 flow) and 80% LAD stenosis. Balloon angioplasty and thrombectomy restored TIMI III flow to RCA and angina settled. Relook angiogram was planned after 7 days due to high residual thrombus. However, angina recur 2 days later and angiogram showed reocclusion of RCA. Thrombectomy repeated and a stent was placed with good result. Staged PCI was planned for the LAD lesion.
Relevant Test Results Prior to Catheterization
Blood tests showed normal full blood count, stable renal function, balanced electrolytes, and normal liver/coagulation profiles. High-sensitivity troponin I was elevated at 5248.1 ng/L, indicating significant myocardial injury. ECG showed inferior ST-elevation with no right side and posterior involvement. Echocardiogram confirmed inferior wall hypokinesia with preserved ejection fraction, normal valves, and no pericardial effusion.
Relevant Catheterization Findings
1st angiogram showed acute RCA occlusion (TIMI 0) and 80% LAD stenosis. A temporary pacemaker was inserted prior to the angioplasty. Serial predilations of RCA and aspiration thrombectomy improved flow to TIMI III, but residual thrombus remained, hence procedure stopped and anticoagulation was initiated. The urgent 2nd angiogram 2 days later showed total reocclusion of RCA, which further serial predilations and aspiration thrombectomy were done. A stent was placed at the RCA with good result.
Interventional Management
Procedural Step
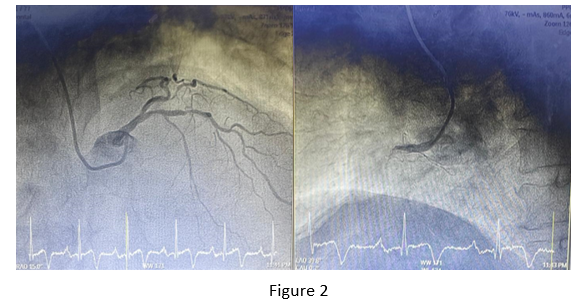
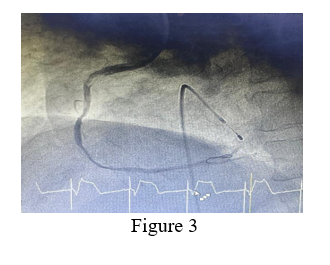
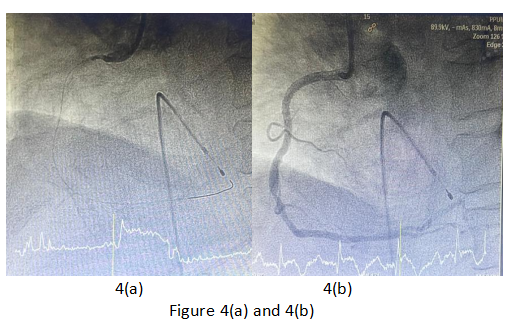
An initial diagnostic angiogram using a 5F Terumo Optitorque catheter via the right radial artery revealed an acute total occlusion (ATO) of the proximal RCA (TIMI 0 flow) and 80% stenosis in the proximal LAD (Figure 2). Due to transient heart block, temporary transvenous pacemaker (TVP) was inserted. Angioplasty began with a 6F Judkins Right(JR) 3.5 guiding catheter, using workhorse wire (Runthrough) to cross the RCA occlusion. Predilatations with semi-compliant balloons (Sapphire 1.5 x 10 mm and Sapphire 2.5 x 15 mm) only achieved TIMI I flow. Following aspiration thrombectomy (Thrombuster II), flow improved to TIMI III, although moderate thrombus (TIMI Thrombus Grade 3) persisted (Figure 3). Given the patient’s stable condition, further intervention was deferred, and he was transferred to the CCU for anticoagulation and dual antiplatelet therapy, with a follow-up angiogram planned after seven days.On the second day, he developed recurrent chest pain, with repeated ECG showing recurrent inferior ST-elevation. Relook angiogram using 6F JR 3 guiding catheter showed re-occlusion of the RCA (TIMI 0 flow) (Figure 4a). Re-crossing, further serial predilatations and aspirations restored TIMI III flow, this time without any significant residual thrombus. Finally, a DES (Combo Plus 3.5 x 28 mm) was deployed with optimal TIMI III flow (Figure 4b). QFR analysis showed a non-significant value (0.85) at the moderate lesion at distal RCA. LAD lesion was decided for early staged PCI.
Case Summary
This case illustrates key interventional strategies: thrombus aspiration was pivotal in restoring flow in ATO, aligning with TASTE and TOTAL trials that support selective use in high thrombus burden. For culprit-only vs. full revascularization in STEMI, ESC (2018) and ACC/AHA (2021) guidelines favor culprit-only PCI in the index procedure, reserving staged revascularization for non-culprit lesions, especially in cardiogenic shock patients. Lastly, adjunct such as GP IIb/IIIa inhibitors(tirofiban) are valuable in cases of high thrombus burden and no-reflow, per ESC STEMI guidelines (2018), though now its role is mostly reserved as bailout therapy.