
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-081
A Case of Three Chronic Total Occlusions, One in Every Epicardial Artery: What to Do and How to Do?
By Hsiao-Tse Tu
Presenter
Hsiao-Tse Tu
Authors
Hsiao-Tse Tu1
Affiliation
Taichung Veterans General Hospital, Taiwan1,
View Study Report
TCTAP C-081
Coronary - Complex PCI - CTO
A Case of Three Chronic Total Occlusions, One in Every Epicardial Artery: What to Do and How to Do?
Hsiao-Tse Tu1
Taichung Veterans General Hospital, Taiwan1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
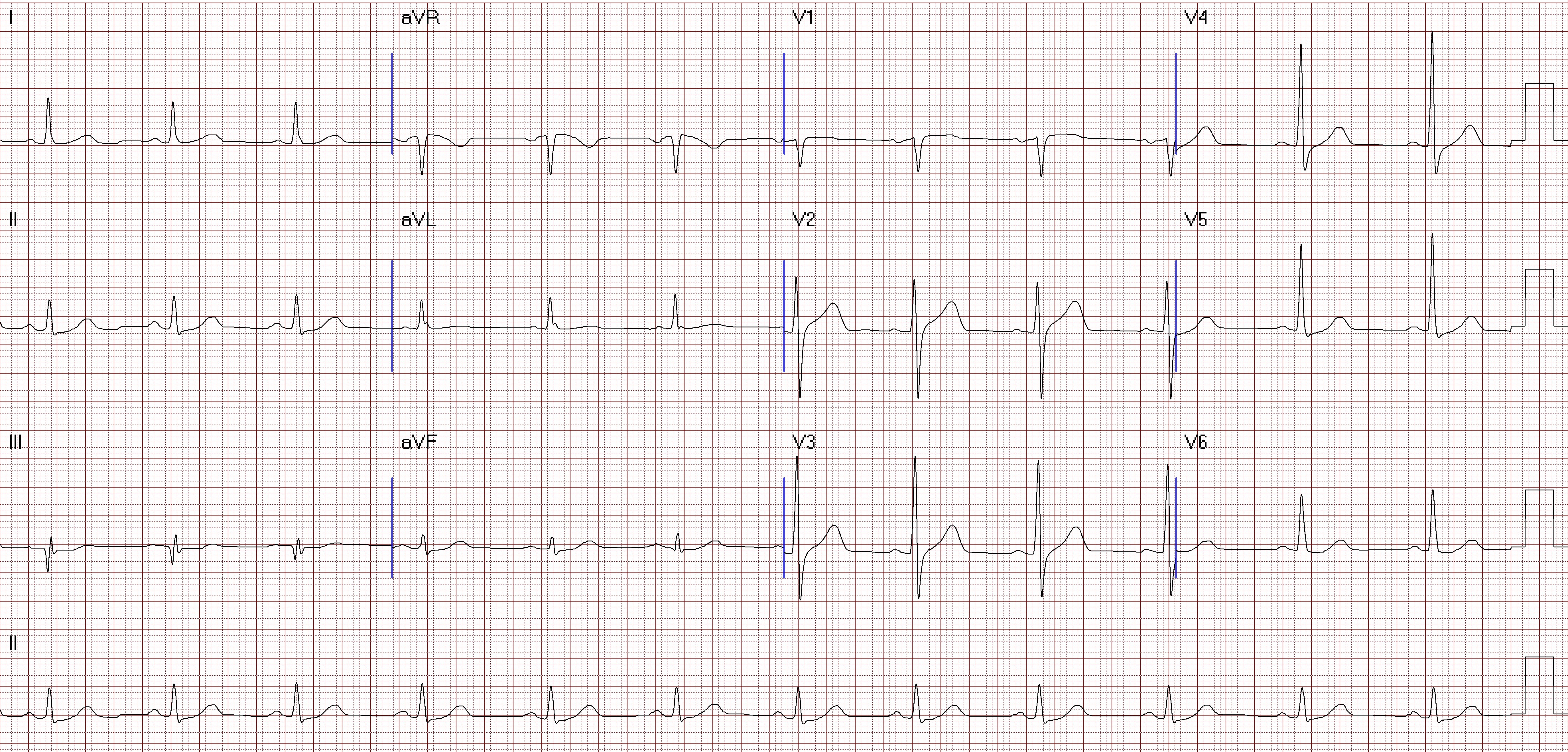
A 55-year-old man who has medical history of hyperlipidemia and personal history of cigarette smoking for decades came to our outpatient clinic for intermittent chest tightness for about 10 years, which got worsened when exercise. Also, short of breath after walking or taking little exercise was stated by the patient. On review, physical examination had no significant finding. An ECG showed sinus rhythm with Q wave over lead III.
Relevant Test Results Prior to Catheterization
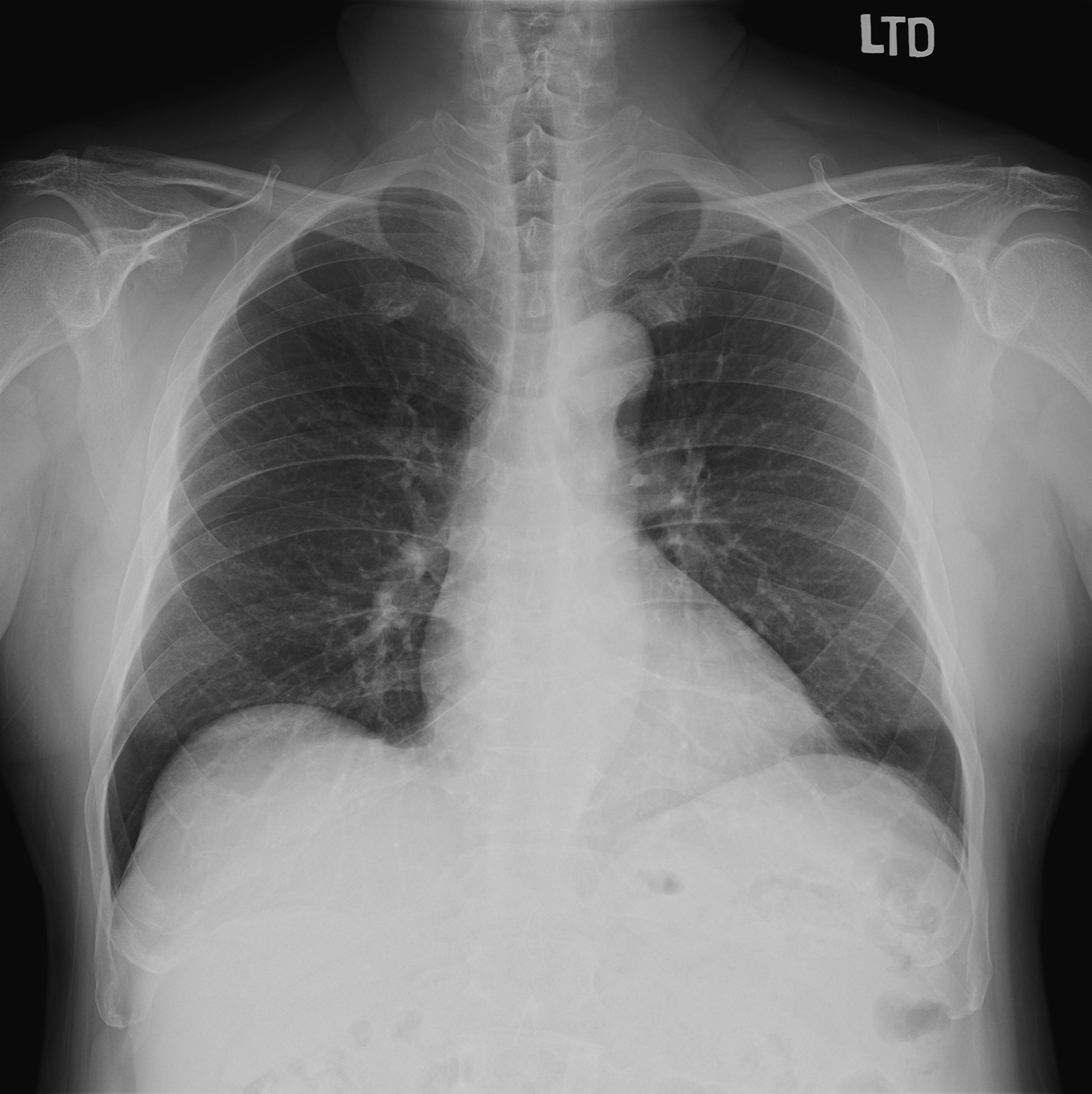
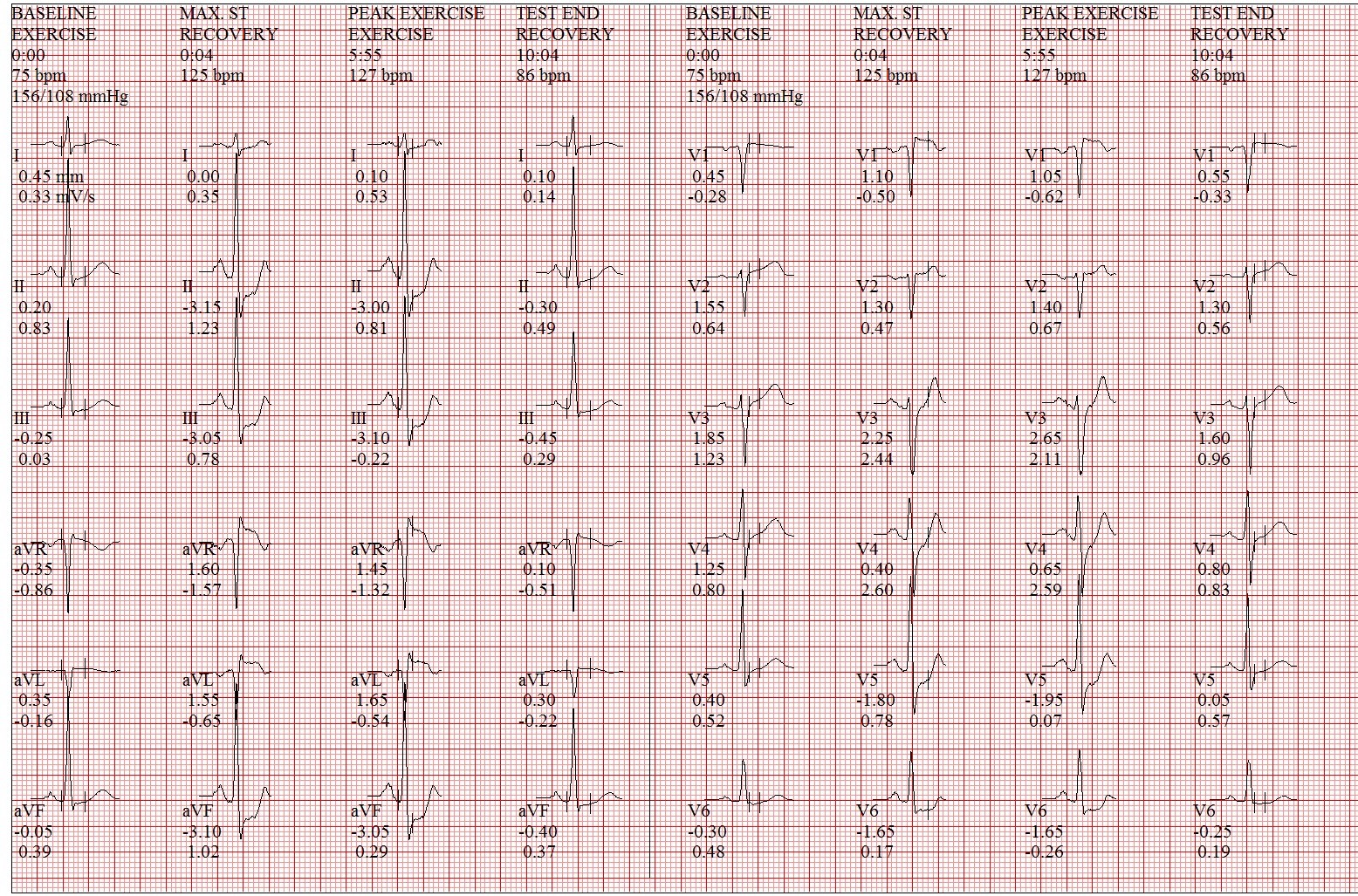
Treadmill's exercise ECG was performed, and showed ST depression over inferior and lateral leads. The exam was terminated before 90% predicted heart rate achieved(Bruce stage 2) due to dyspnea and the patient cannot follow up. Echocardiogram was also arranged, and showed mild AR, TR, mild to moderate MR and normal LV systolic wall motion with LVEF 55%. Chest X ray found no definite evidence of significant active lung lesion or cardiomegaly.
Relevant Catheterization Findings
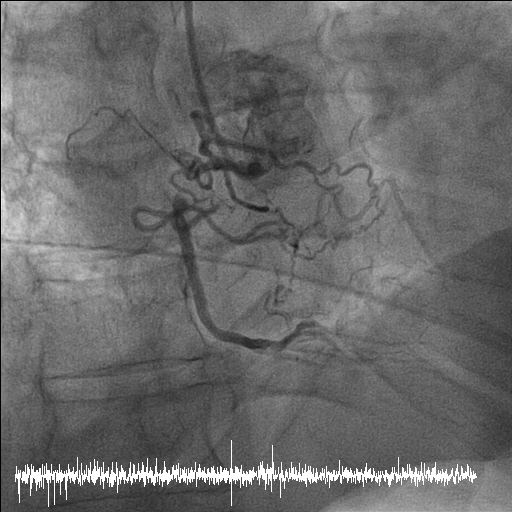
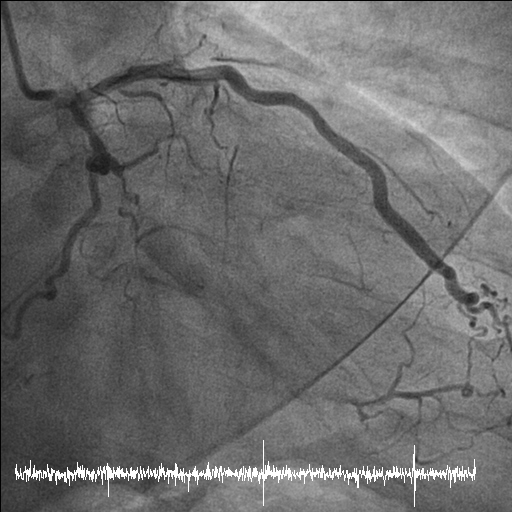
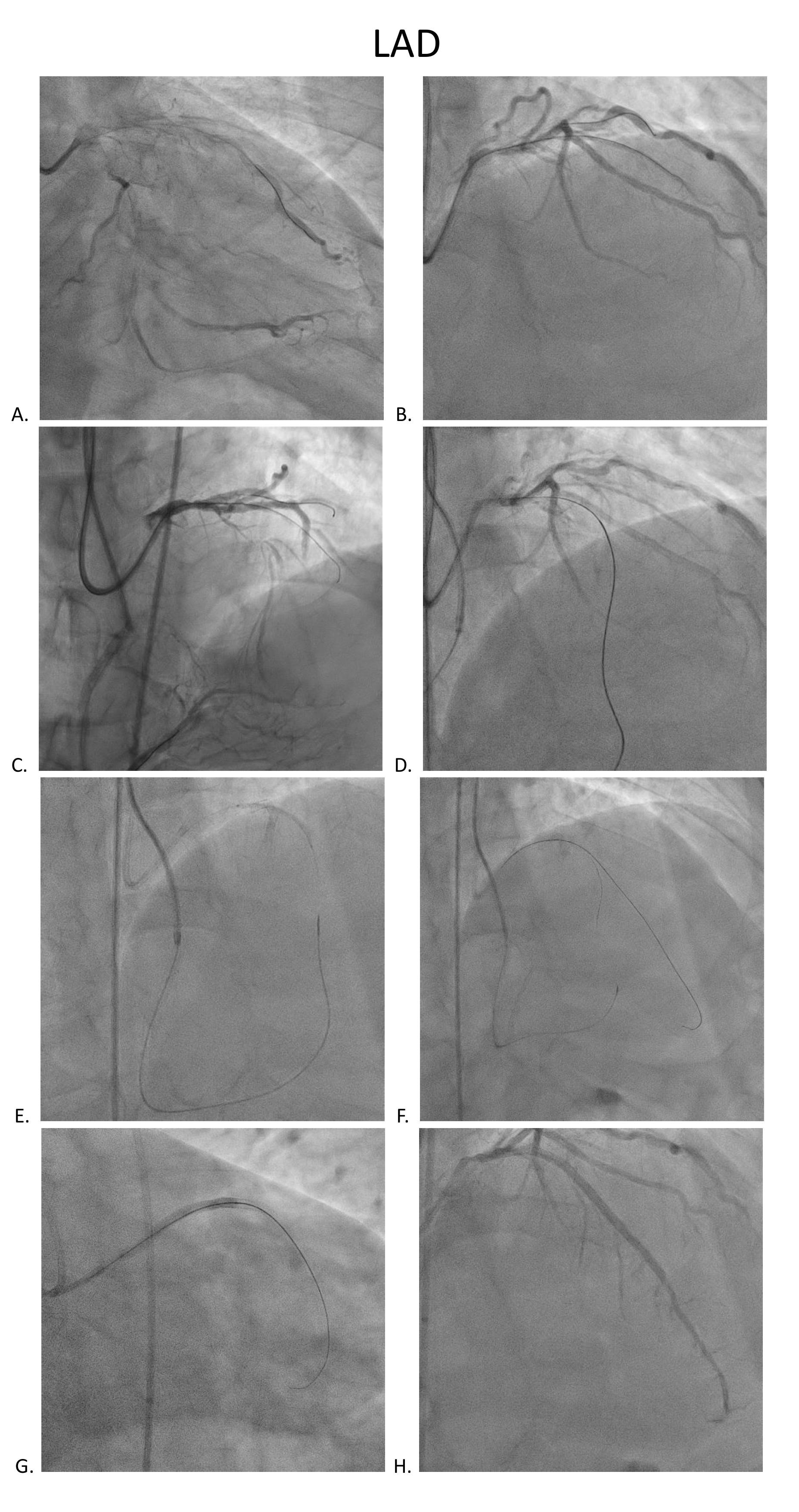
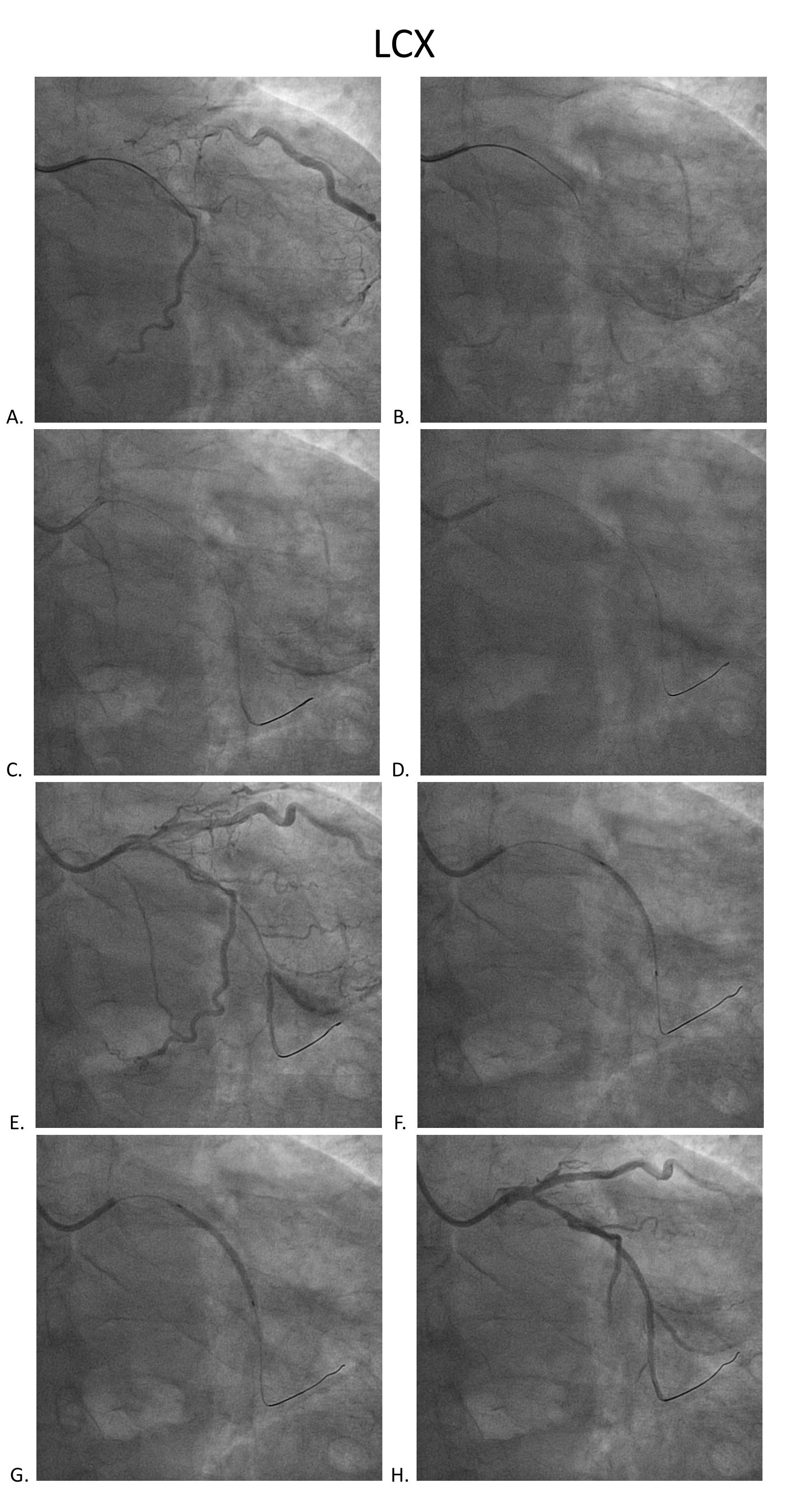
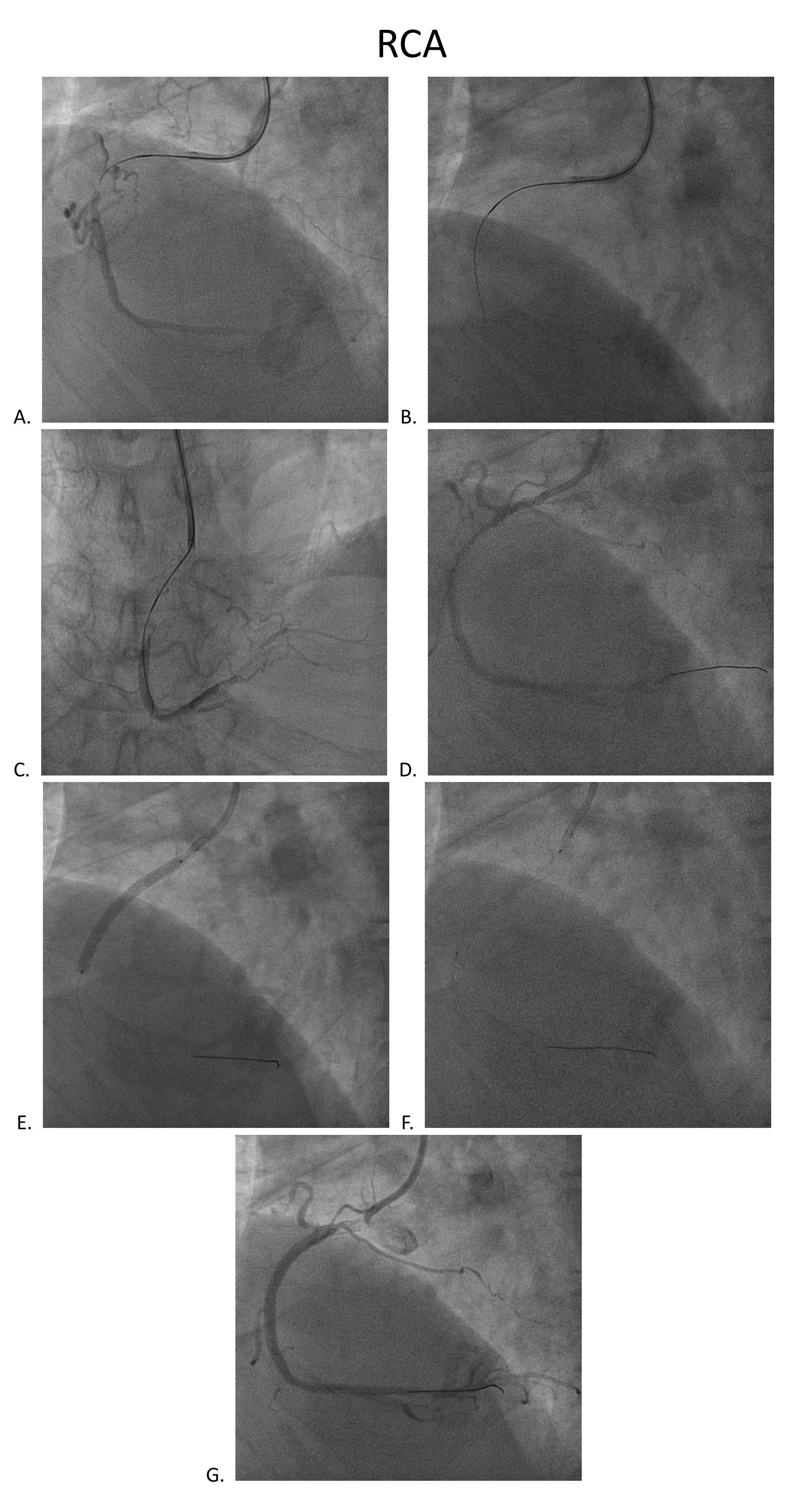
Coronary angiography disclosed orifice total occlusion with TIMI grade 0 antegrade flow at LAD, middle total occlusion at LCX, and RCA proximal total occlusion with auto-collateral to RCA distal.

Interventional Management
Procedural Step
SCR guiding cath was used to engage RCA. Runthrough wire, Conquest pro, and Conquest 860 wire were used to get cross the CTO lesion. Resolute 2.75x38mm stent was inflated after predilatation with different size BC. XB 3.0x6fr guiding cath was used to engage LCX. Sion blue, Conquest pro, and Fielder XT-A wire were used to get cross the LCX lesion. Predilatation was done with 1.5x20mm BC, followed by Sierra 2.0x38mm stenting and 2.0x30mm B. Braun DEB.
Stage PCI for stumpless LAD-os-P CTO was arranged two months later. Antegrade strategy was tried initially, but shifted to retrograde approach due to wiring failed because of tiny LAD-M true lumen. We used SAL 1x6F guide via right femoral access. After trying, one septal collateral via PDA could be wired with a Fielder XT-R and Caravel. After switching the Caravel to Corsair Pro XS, it could be advanced to LAD-M. The CTO segment was retrogradely attempted with Conquest Pro, UB and finally reached LM body. Using a Sion blue, the wire could go into the antegrade guide, followed by advancing the Corsair Pro XS into the guide. The lesions were antegradely dilated with BC after RG 3 wire externalization and antegrade flow was established. By using a Crusade, the LAD proper could be successfully wired wtih a Fielder XT-A. LAD-M-D and LAD-os-P-M were predilated with a 2x30mm BC(IVUS confirmed all true lumen wiring) and respectively scaffolded with a 2.75x38mm Onyx and a 3x48mm Synergy. There was no residual stenosis over all 3 vessels.
Stage PCI for stumpless LAD-os-P CTO was arranged two months later. Antegrade strategy was tried initially, but shifted to retrograde approach due to wiring failed because of tiny LAD-M true lumen. We used SAL 1x6F guide via right femoral access. After trying, one septal collateral via PDA could be wired with a Fielder XT-R and Caravel. After switching the Caravel to Corsair Pro XS, it could be advanced to LAD-M. The CTO segment was retrogradely attempted with Conquest Pro, UB and finally reached LM body. Using a Sion blue, the wire could go into the antegrade guide, followed by advancing the Corsair Pro XS into the guide. The lesions were antegradely dilated with BC after RG 3 wire externalization and antegrade flow was established. By using a Crusade, the LAD proper could be successfully wired wtih a Fielder XT-A. LAD-M-D and LAD-os-P-M were predilated with a 2x30mm BC(IVUS confirmed all true lumen wiring) and respectively scaffolded with a 2.75x38mm Onyx and a 3x48mm Synergy. There was no residual stenosis over all 3 vessels.
Case Summary
For treating every CTO lesion, film reading and patience both play an important role . As for treating multiple and complicated CTOs, it depends on not only sharing decision making with the patient but also operator's experiences and skills to make the treatment principle and plans. This case would be an example that combining good antegrade and retrograde PCI skills is extremely important to complete PCIs in cases with multiple and complicated CTOs.