
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-005
Impella-Assisted Complete Revascularization in Cardiogenic Shock Due to STEMI With Three-Vessel Occlusion: A Case Report
By Akimune Kuwayama, Hidetaka Nishina, Takayuki Yamaguchi, Takumi Sato
Presenter
Akimune Kuwayama
Authors
Akimune Kuwayama1, Hidetaka Nishina1, Takayuki Yamaguchi1, Takumi Sato1
Affiliation
Tsukuba Medical Center Hospital, Japan1,
View Study Report
TCTAP C-005
Coronary - ACS/AMI
Impella-Assisted Complete Revascularization in Cardiogenic Shock Due to STEMI With Three-Vessel Occlusion: A Case Report
Akimune Kuwayama1, Hidetaka Nishina1, Takayuki Yamaguchi1, Takumi Sato1
Tsukuba Medical Center Hospital, Japan1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
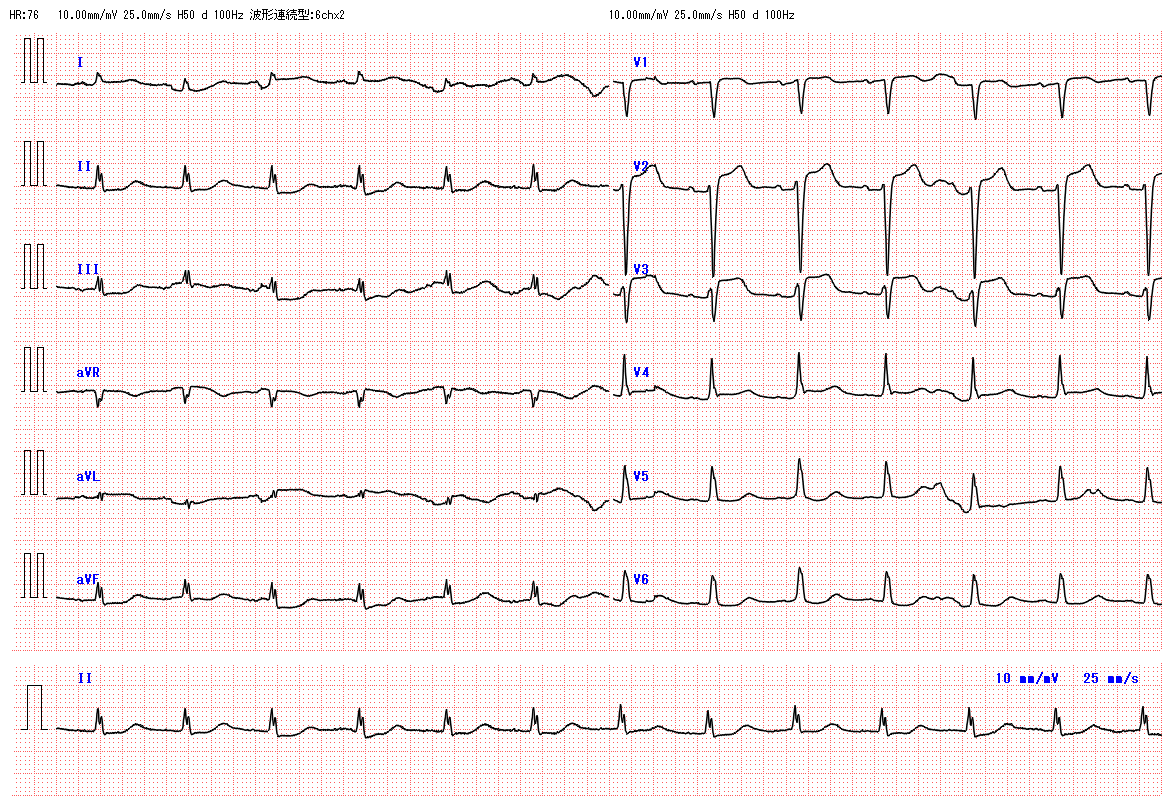
A 67-year-old woman was transferred to our institution for progressive chest discomfort and dyspnea. Blood pressure and SpO₂ were unmeasurable, heart rate was 52 bpm, respiratory rate was 27 breaths per minute. She was in decreased consciousness, marked cold sweats, and crackles were auscultated bilaterally. Initial ECG showed ST elevation in the leads aVR, V1-V3, with reciprocal ST depression in the inferior leads.
Relevant Test Results Prior to Catheterization
Echocardiography revealed severe hypokinesis except for the basal to mid segments of the inferior and posterior walls, with an estimated visual EF of approximately 15%, and no valvular abnormalities were observed. After initiating tracheal intubation and mechanical ventilation, blood tests showed troponin T 0.179 ng/ml, BNP 469.4 pg/ml, pH 6.961, pCO₂ 50.6 mmHg, pO₂ 174.4 mmHg, lactate 12.59 mmol/L, and HCO₃⁻ 11.2 mmol/L.
Relevant Catheterization Findings
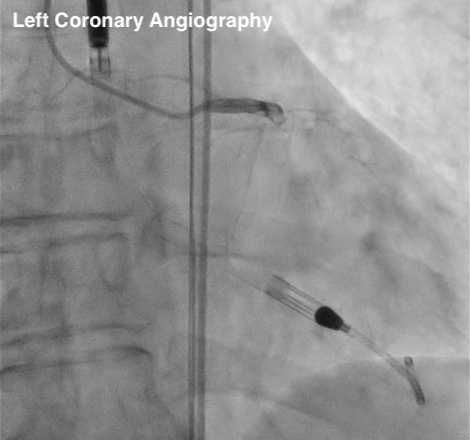
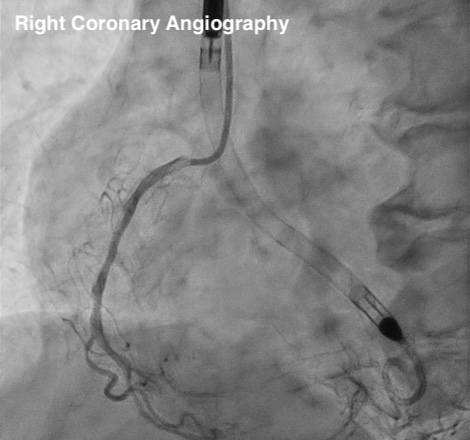
An Impella CP was inserted to support circulation. Coronary angiography revealed occlusions in the proximal LAD, proximal LCX, and distal RCA.
Interventional Management
Procedural Step
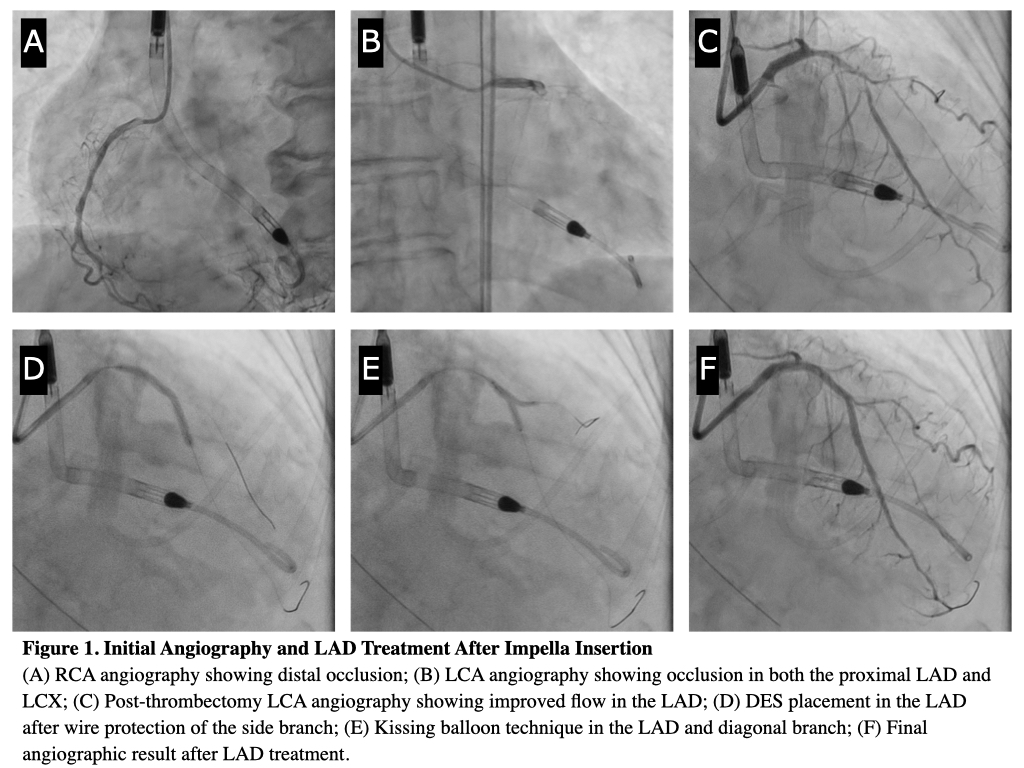
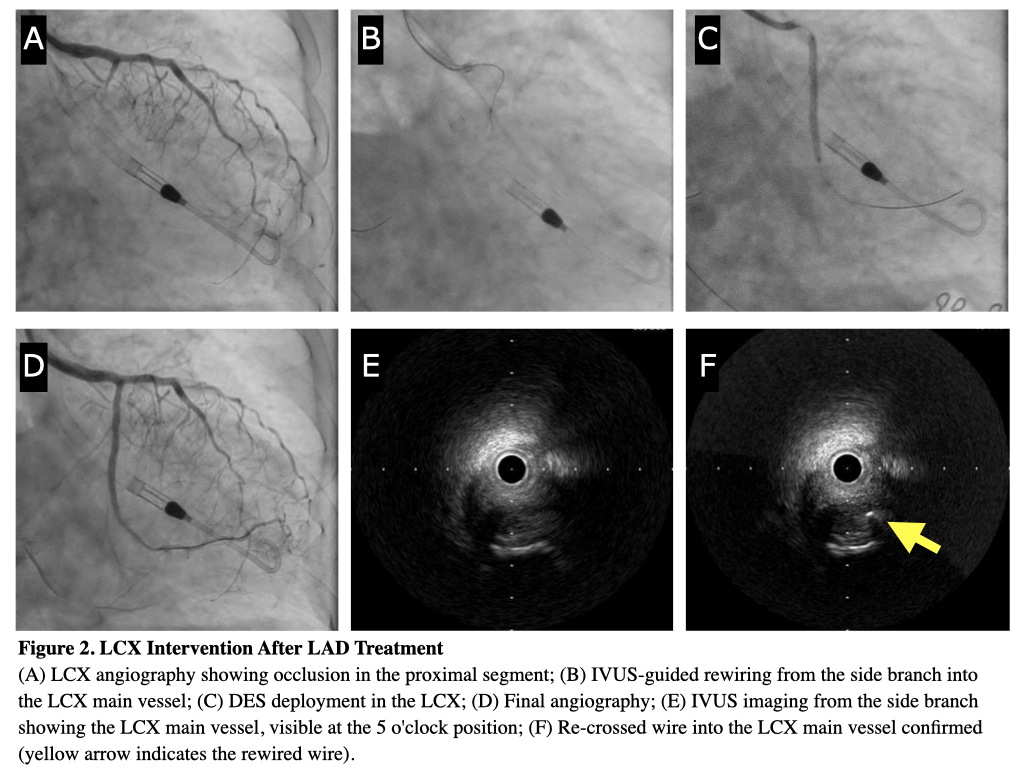
LAD treatment was initiated as it was considered the culprit lesion based on ECG and echocardiography. Following successful reperfusion with manual thrombectomy, a DES was deployed, followed by kissing balloon technique with the diagonal branch (Figure 1). Subsequently, LCX was treated in the same session to enhance cardiac function recovery. After confirmation of the CTO entry site with IVUS from the side branch, a tapered wire entered the CTO and proceeded through the microchannel to the distal true lumen; a DES was then deployed, completing the first stage of treatment (Figure 2).
Cardiac function improved gradually under initial PCI, allowing for safe Impella weaning. Given the extensive LAD infarction with reduced LVEF, RCA-CTO treatment before Impella removal was considered appropriate.
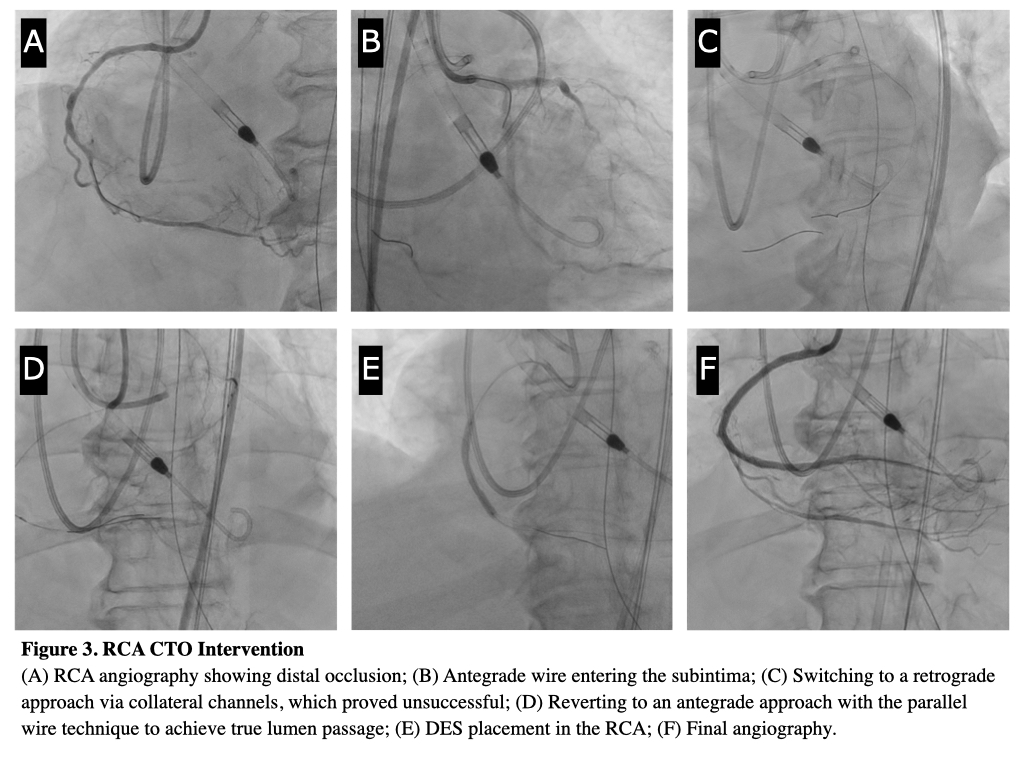
RCA treatment was started with an antegrade approach, but subintimal wire entry necessitated a switch to the retrograde approach. Failure to cross the collateral channel led to reverting to an antegrade approach. Using a parallel wire technique, the lesion was successfully crossed, and three DES were deployed, achieving complete revascularization (Figure 3). The Impella was subsequently removed, with stable hemodynamics and respiratory status. The patient was liberated from mechanical ventilation on Day 10 and discharged from the ICU on Day 11.
Cardiac function improved gradually under initial PCI, allowing for safe Impella weaning. Given the extensive LAD infarction with reduced LVEF, RCA-CTO treatment before Impella removal was considered appropriate.
RCA treatment was started with an antegrade approach, but subintimal wire entry necessitated a switch to the retrograde approach. Failure to cross the collateral channel led to reverting to an antegrade approach. Using a parallel wire technique, the lesion was successfully crossed, and three DES were deployed, achieving complete revascularization (Figure 3). The Impella was subsequently removed, with stable hemodynamics and respiratory status. The patient was liberated from mechanical ventilation on Day 10 and discharged from the ICU on Day 11.
Case Summary
Impella-assisted PCI in this multivessel, high-risk STEMI case with cardiogenic shock resulted in significant hemodynamic improvement and successful revascularization. This case highlights the potential benefits of Impella support in achieving complete revascularization in critically ill patients with extensive coronary disease.