
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-163
Rescue Stenting of Acute Severe Iatrogenic Flow-Limiting Dissection of Left Main Coronary Artery During Percutaneous Coronary Intervention of Left Anterior Descending Artery
By Quek Ao Xiang, Cheng Jin Kiang, Lau Waye Young, Sim Jian Hao, Ng Wee Pang, Wong Wen Sheng, Kim Heng Shee
Presenter
Quek Ao Xiang
Authors
Quek Ao Xiang1, Cheng Jin Kiang1, Lau Waye Young1, Sim Jian Hao1, Ng Wee Pang1, Wong Wen Sheng1, Kim Heng Shee1
Affiliation
Sultanah Aminah Hospital, Malaysia1,
View Study Report
TCTAP C-163
Coronary - Complication Management
Rescue Stenting of Acute Severe Iatrogenic Flow-Limiting Dissection of Left Main Coronary Artery During Percutaneous Coronary Intervention of Left Anterior Descending Artery
Quek Ao Xiang1, Cheng Jin Kiang1, Lau Waye Young1, Sim Jian Hao1, Ng Wee Pang1, Wong Wen Sheng1, Kim Heng Shee1
Sultanah Aminah Hospital, Malaysia1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
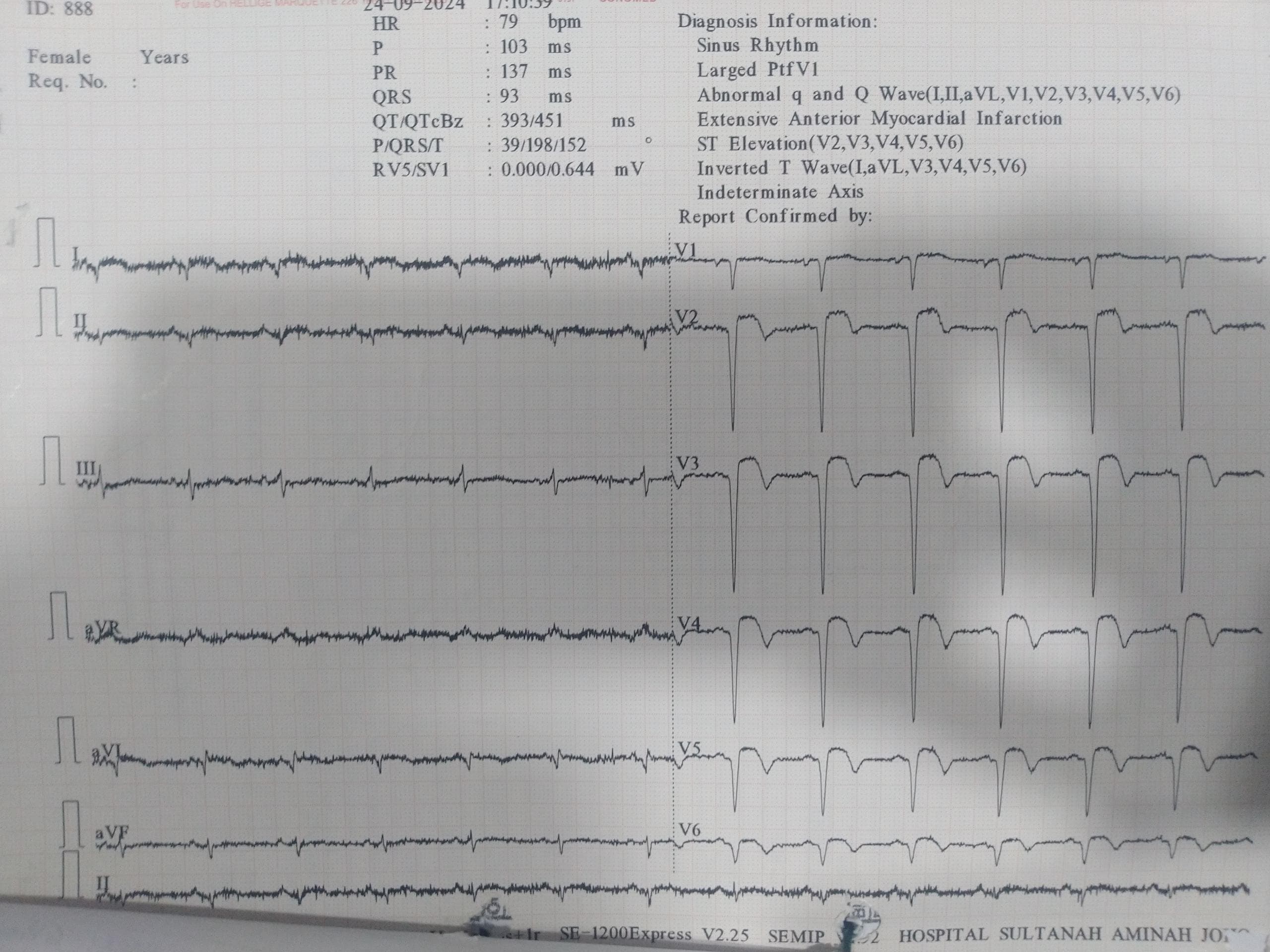
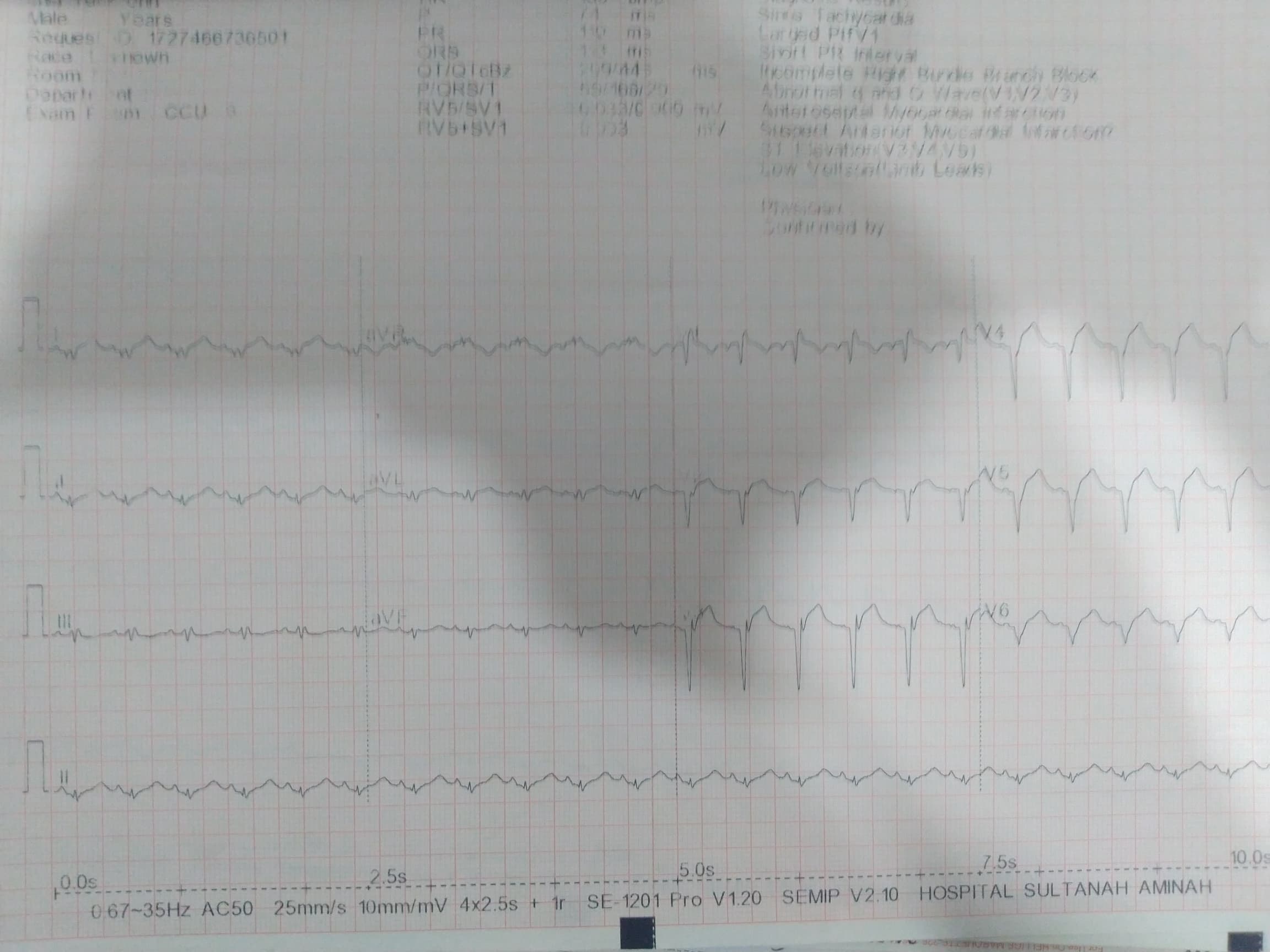
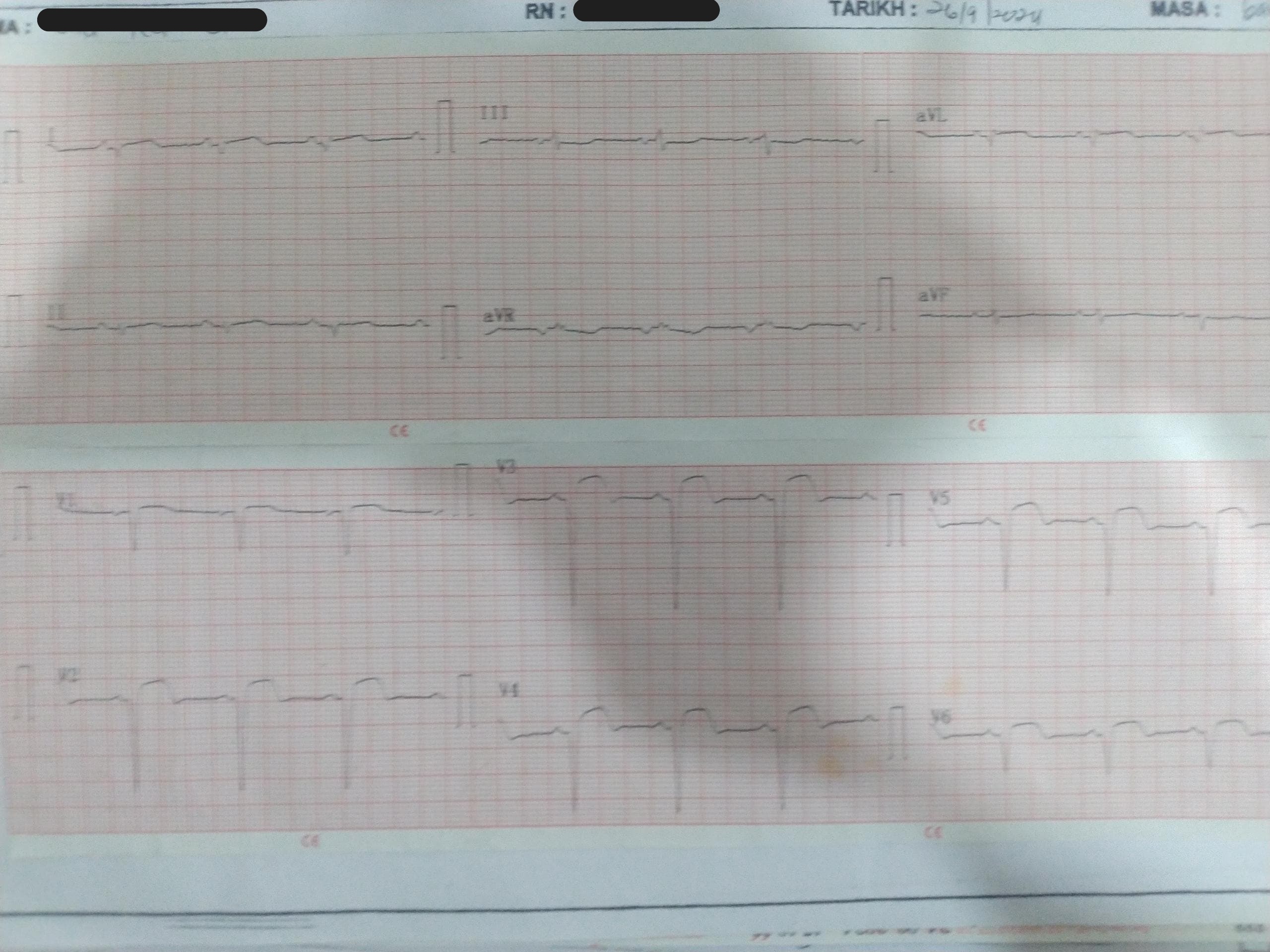
A 67-year-old man, a chronic smoker who was initially admitted in a hospital in Indonesia for extensive anterior myocardial infarction presented to our hospital 1 day after discharge with persistent chest pain associated with jaw numbness, diaphoresis and vomiting. On admission, his blood pressure was 106/74 mmHg and heart rate was 81 beats per minute. Otherwise, the respiratory and cardiovascular systems examination were normal.
Relevant Test Results Prior to Catheterization
His electrocardiogram on admission showed sinus rhythm with deep Q wave over lead V1 to V6 with ST elevation of 3mm. His Trop T was 78454 ng/L and creatinine kinase was 692 U/L. His lactate dehydrogenase was 1256 U/L. He had mild acute kidney injury with creatinine level of 114 micromoles/L. His total cholesterol was 4.5mmol/L and low density lipoprotein was 2.8 mmol/L. The fasting blood glucose level was 3 mmol/L. Otherwise, the liver function test and electrolytes levels were unremarkable.
Relevant Catheterization Findings
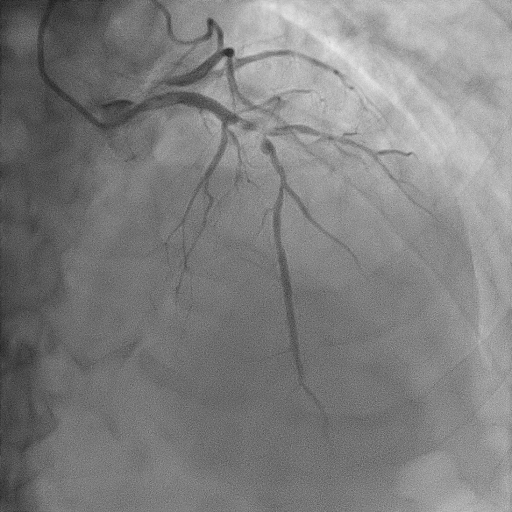
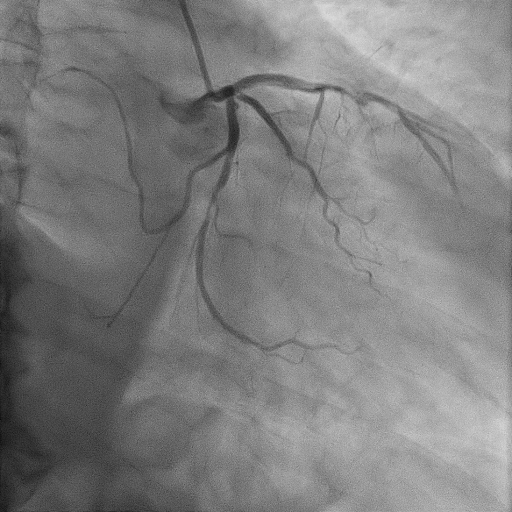
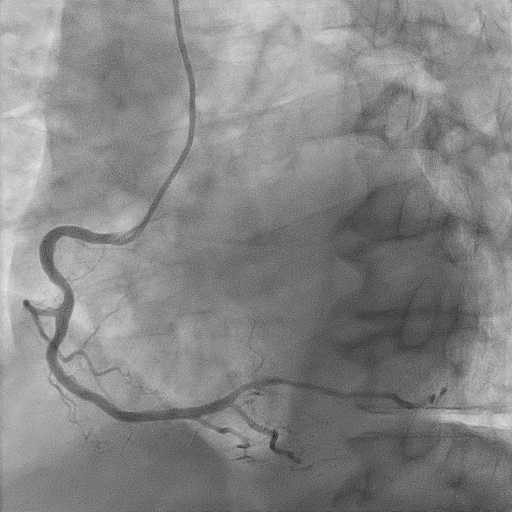
The coronary angiography revealed normal and short left main coronary artery. The proximal to mid left anterior descending artery had severe stenosis of 90% with thrombus. The proximal segment of diagonal 1 had 80% stenosis. The proximal and distal left circumflex artery showed 50% and 80% stenosis respectively. The right coronary artery showed mild lesion of 20-30% at mid segment. The posterior left ventricular artery showed moderate stenosis of 50% at mid segment.
Interventional Management
Procedural Step
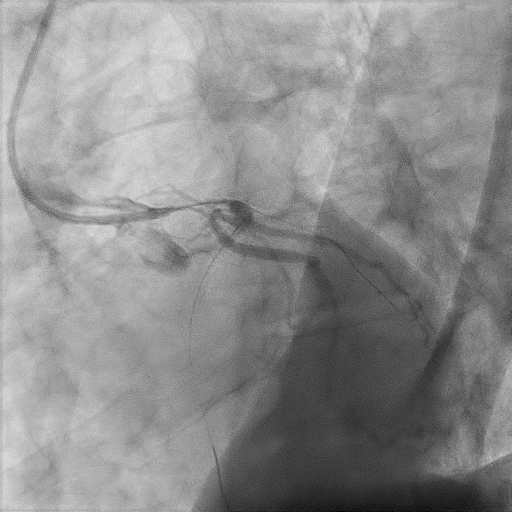
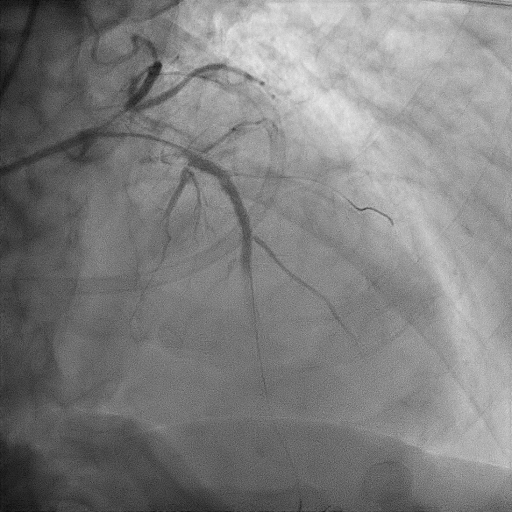
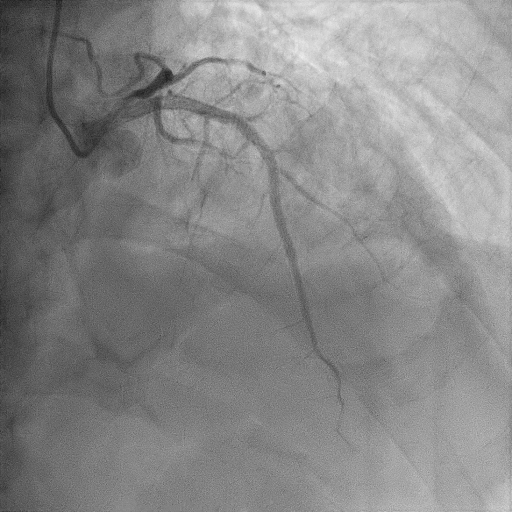
We proceeded with delayed selective PCI to the left anterior descending artery (LAD). The left main coronary artery (LMCA) was engaged with guiding catheter Medtronic Launcher 6FR EBU 3.5. The PTCA guide wire Shun R (SHUNMEI Medical) crossed the lesion with ease. Besides, we wired the diagonal 1 with PT2 (Boston Scientific) to provide side branch protection. The proximal to mid segment of the LAD lesion was pre-dilated with Sapphire NC 24 PTCA balloon 3.0x15mm and inflated to 12 atm. The lesion was stented with Xience Xpedition 3.0x48mm and inflated to 10atm. The stent was post-dilated with NC Trek balloon 3.5x12mm and inflated to 14atm. Noted while retracting the balloon during post-dilatation, the guiding catheter advanced deep into the LMCA several times. Subsequently, patient became progressively hemodynamically unstable. Trial of aspiration with Genoss Extractor but no thrombus was aspirated. Intracoronary Tirofiban bolus was administered. Unfortunately, patient went into cardiorespiratory arrest and intensive resuscitation was commenced. Angiography showed severe flow-limiting type D dissection of the LMCA. We proceeded with rescue stenting of LMCA with Xience Sierra 3.5x38mm with inflation to 12atm. The stent was post-dilated with NC Euphora 4.0x8mm and inflated to 18atm. The final result was TIMI flow 3 but the stent was about 3 to 5 mm proximal to the LMCA ostium. An intra-aortic balloon pump was also inserted and patient required 4 inotropes.
Case Summary
Iatrogenic catheter-induced left main coronary artery dissection is a life-threatening complication. Meticulous manipulation of catheter is of upmost important during percutaneous coronary intervention to prevent such complication. Rescue percutaneous angioplasty of the LMCA dissection is potentially life-saving by restoring coronary flow and prevent further irreversible damage to the myocardium. As the stent was protruded outside the left main ostium and possibly under-expanded, the risk of stent thrombosis and technical difficulty during future PCI are high. Therefore, proper reconstruction and flaring of the stent under IVUS guidance are essential but our patient declined.