
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-029
Revealing an Unusual Cause of Acute STEMI: Insight From Histopathological Analysis of Aspirated Thromboemboli
By Kittipong Youpaniad, Sukhum Tachasakunjareon, Sakolwat Montrivade, Wasant Soonfuang, Anuruck Jeamanukoolkit
Presenter
Kittipong Youpaniad
Authors
Kittipong Youpaniad1, Sukhum Tachasakunjareon1, Sakolwat Montrivade1, Wasant Soonfuang1, Anuruck Jeamanukoolkit1
Affiliation
Police General Hospital, Thailand1,
View Study Report
TCTAP C-029
Coronary - Adjunctive Procedures (Thrombectomy, Atherectomy, Special Balloons)
Revealing an Unusual Cause of Acute STEMI: Insight From Histopathological Analysis of Aspirated Thromboemboli
Kittipong Youpaniad1, Sukhum Tachasakunjareon1, Sakolwat Montrivade1, Wasant Soonfuang1, Anuruck Jeamanukoolkit1
Police General Hospital, Thailand1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A 66-year-old man with a past medical history of hypertension, hyperlipidemia and ischemic stroke presented with a subacute low-grade fever without any localizing signs of infection. On physical examination, his temperature was 37.8°C, lungs were clear on auscultation and cardiovascular examination revealed grade 3 diastolic blowing murmur at right upper parasternal border.
Relevant Test Results Prior to Catheterization
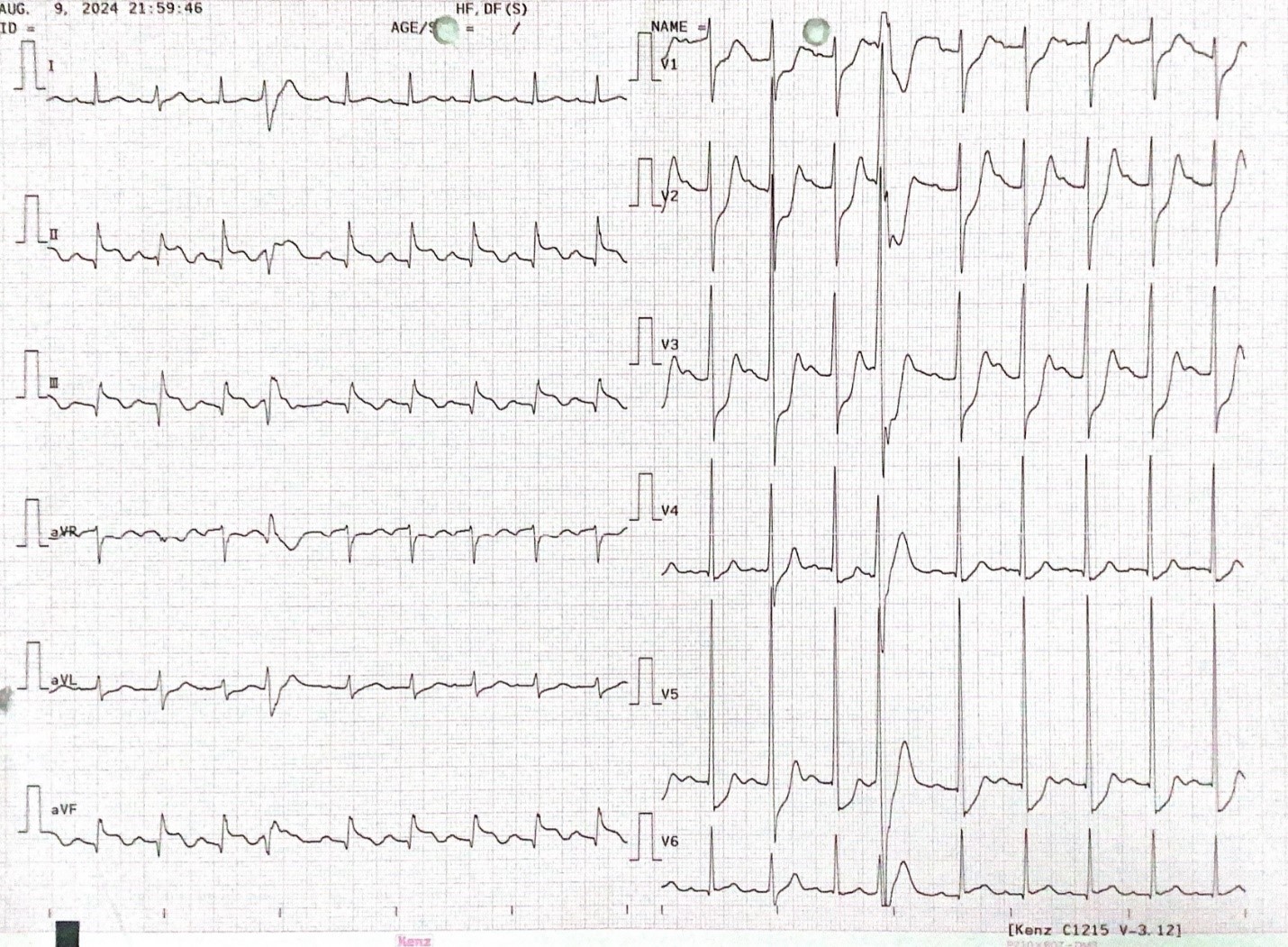
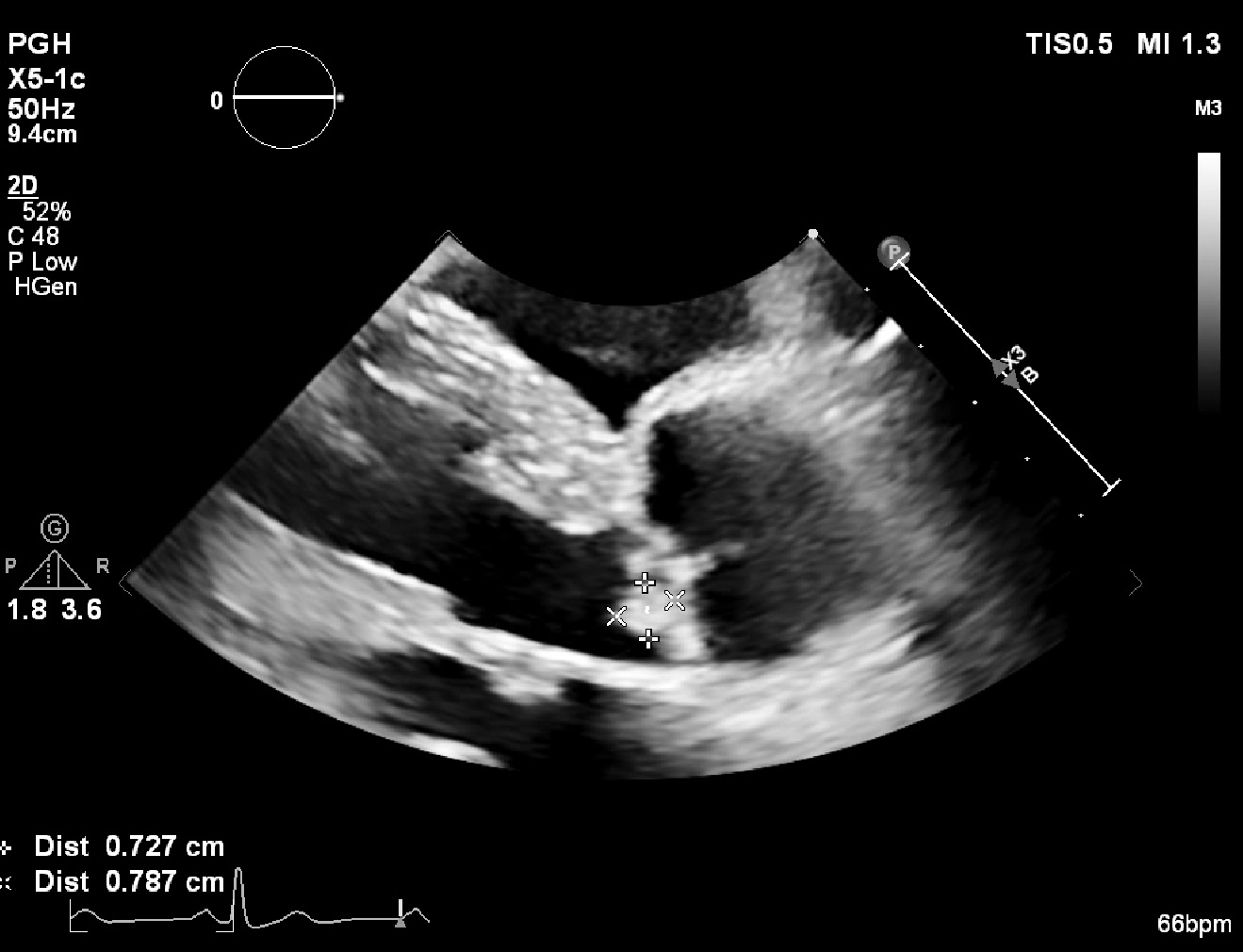
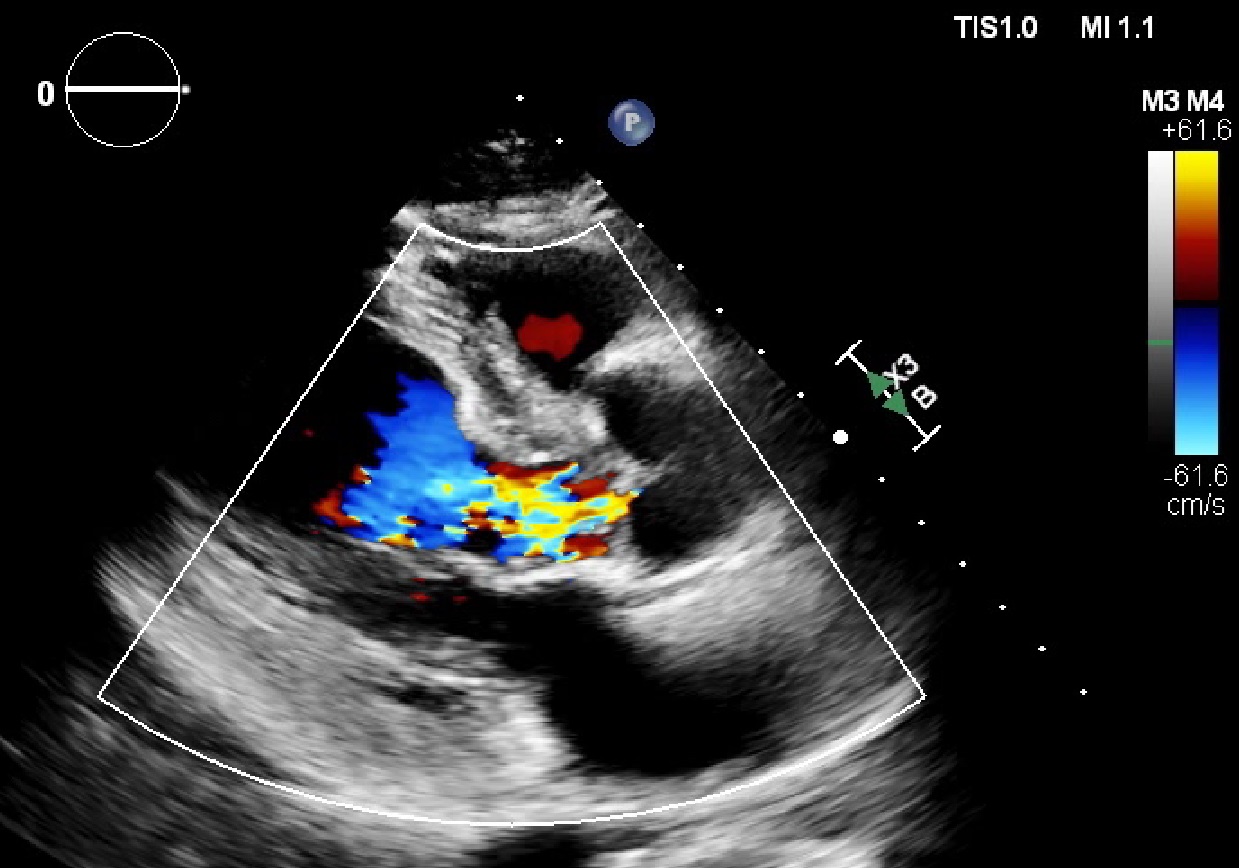
Blood cultures grew Streptococcus mitis. Echocardiograms revealed a 0.72x0.78 cm oscillating mass on LCC of aortic valve along with LCC perforation and severe aortic regurgitation consistent with acute infective endocarditis. After two weeks of intravenous antibiotics, patient experienced sudden onset of chest pain and dyspnea. ECG showed ST elevation in II, III and aVF with ST depression in V1-V5 consistent with inferior wall STEMI.

Relevant Catheterization Findings
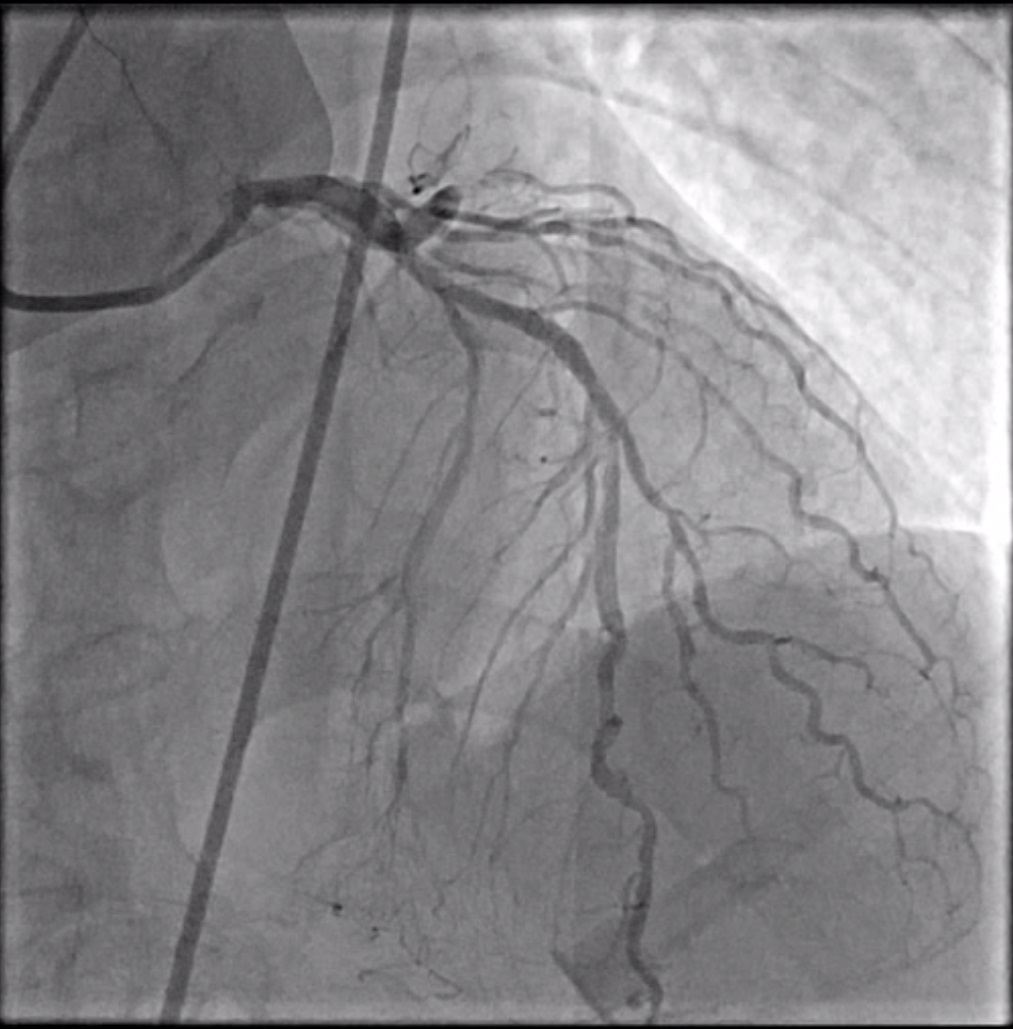
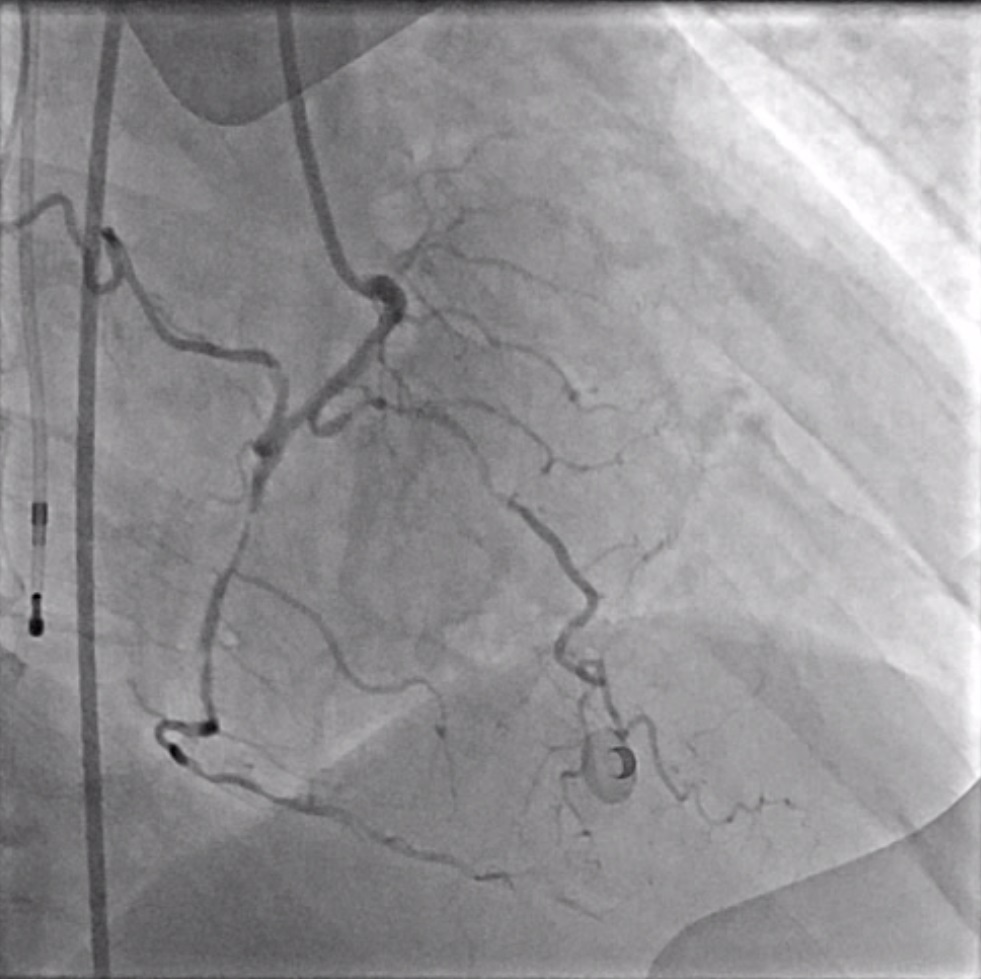
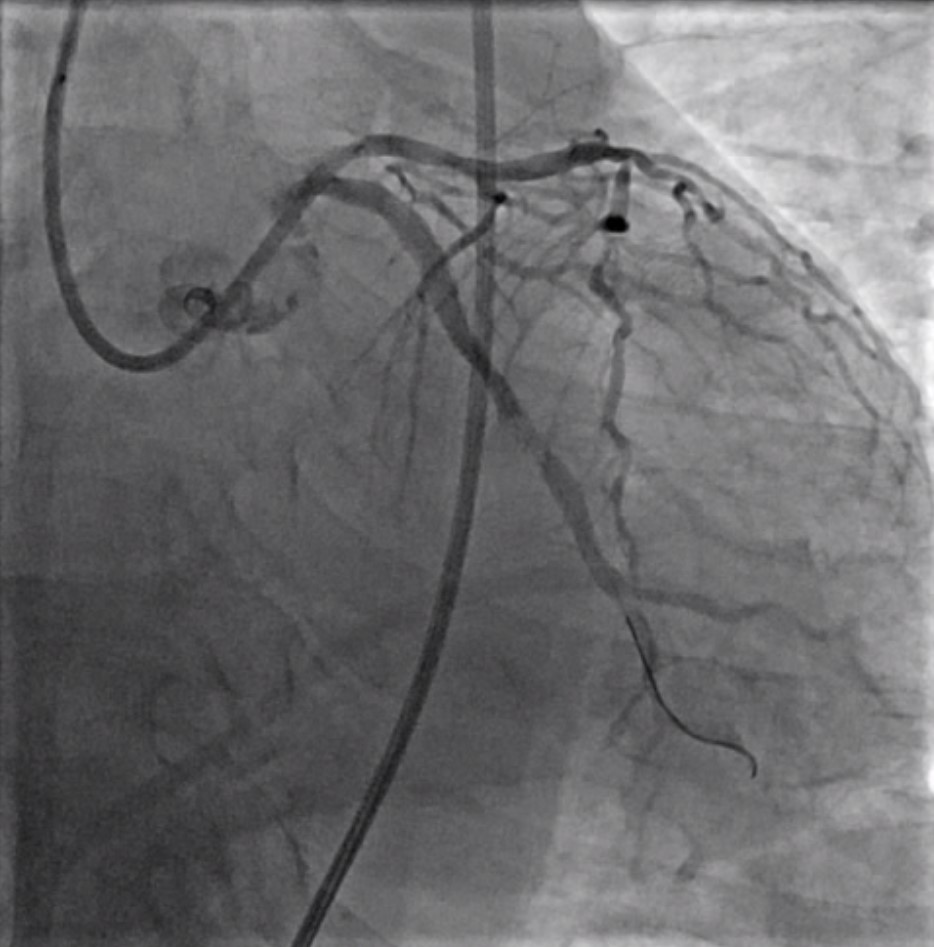
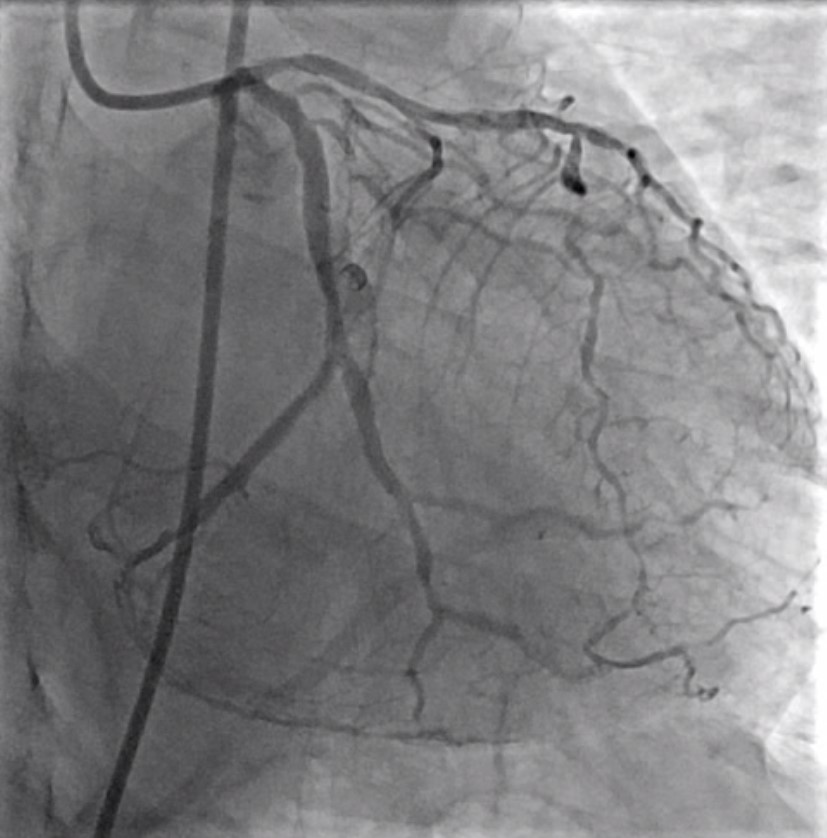
CAG showed three vessels disease. LM: 30% diffuse LM stenosis. LAD: Diffuse disease. 60% Focal stenosis at proximal LAD. 80-90% Focal stenosis at mid LAD. (TIMI III) LCx: 100% Acute thrombotic occlusion at proximal LCx. (TIMI 0) RCA: Diffuse disease. 95-99% Long stenosis at mid RCA. (TIMI III)
Interventional Management
Procedural Step
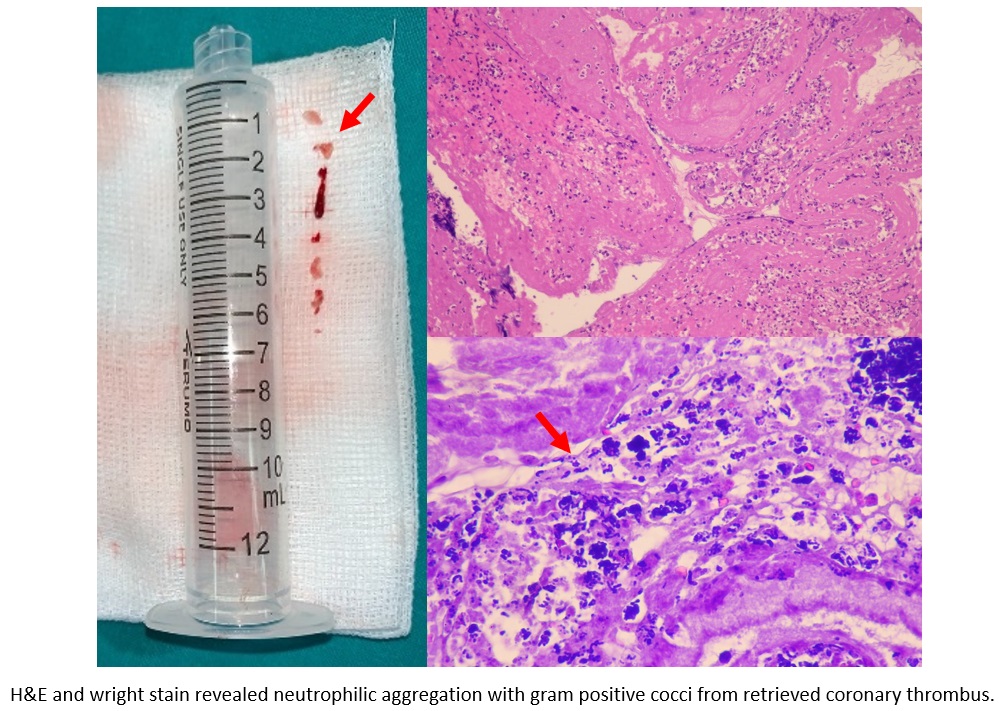
The patient underwent emergency coronary angiography via right femoral access using a 6 Fr sheath. Left coronary artery was engaged with an XB 3.5, 6 Fr catheter and Sion Blue guidewire was advanced into LCx. Manual thrombus aspiration was performed for five times using Export aspiration catheter and large amount of thrombi was obtained as shown. The lesion was further dilated with a 2.5 x 15 mm NC balloon. Although flow was restored, patient continued to experience chest pain with persistent ST elevation on ECG monitoring. After careful review of the angiogram, Sion Blue wire was repositioned into the "true" distal LCx. Additional manual thrombus aspiration was performed and a large amount of thrombi was obtained. Final angiogram showed fully restored flow to the distal LCx and patient’s chest pain resolved. Procedure was concluded and the patient was stabilized for subsequent CABG with aortic valve replacement for the treatment of infective endocarditis and multivessel disease. Gross examination of the retrieved thrombi revealed two red clots measuring 1.5 x 1.0 cm. H&E and wright stain demonstrated gram-positive cocci and evidence of neutrophilic aggregation. These findings definitely confirmed diagnosis of coronary artery embolism from aortic valve vegetation.
Case Summary
Infective endocarditis is a rare cause of ACS. Embolization from valvular vegetations can lead to life-threatening complications such as STEMI. This case highlights coronary embolism originated from aortic valve vegetation demonstrated by tissue histopathological specimen. Thrombus aspiration of coronary embolism is the only effective treatment given the nature of infective tissue unlike thrombosis which can be resolved only with medication.