
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-045
Graft Remnant Assisted Successful Unprotected Left Main Bifurcation Angioplasty Using T and Protrusion Technique: Novel Strategy (GRA-ULMCA)
By Satej Janorkar
Presenter
Satej Janorkar
Authors
Satej Janorkar1
Affiliation
Deenanath Mangeshkar Hospital, India1,
View Study Report
TCTAP C-045
Coronary - Complex PCI - Bifurcation
Graft Remnant Assisted Successful Unprotected Left Main Bifurcation Angioplasty Using T and Protrusion Technique: Novel Strategy (GRA-ULMCA)
Satej Janorkar1
Deenanath Mangeshkar Hospital, India1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
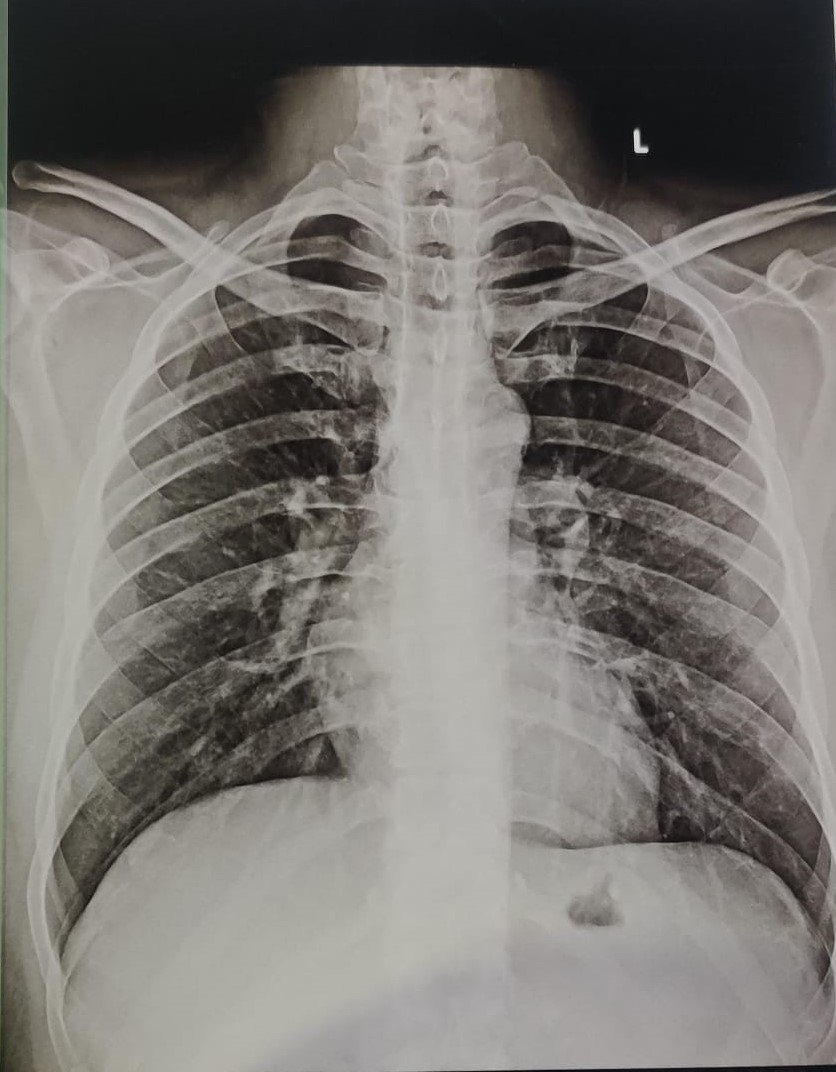
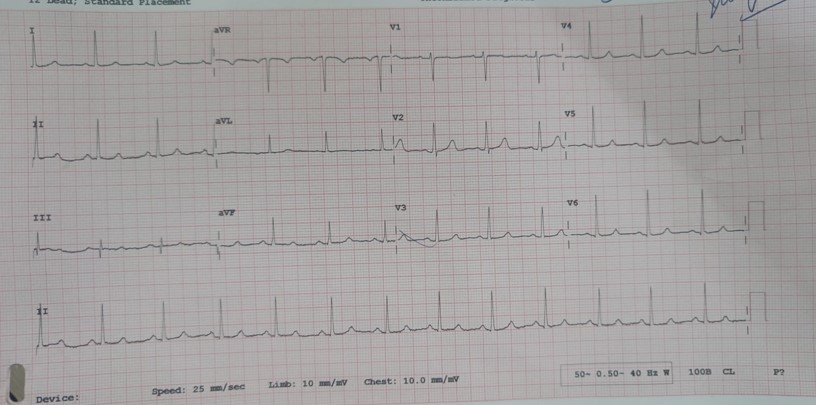
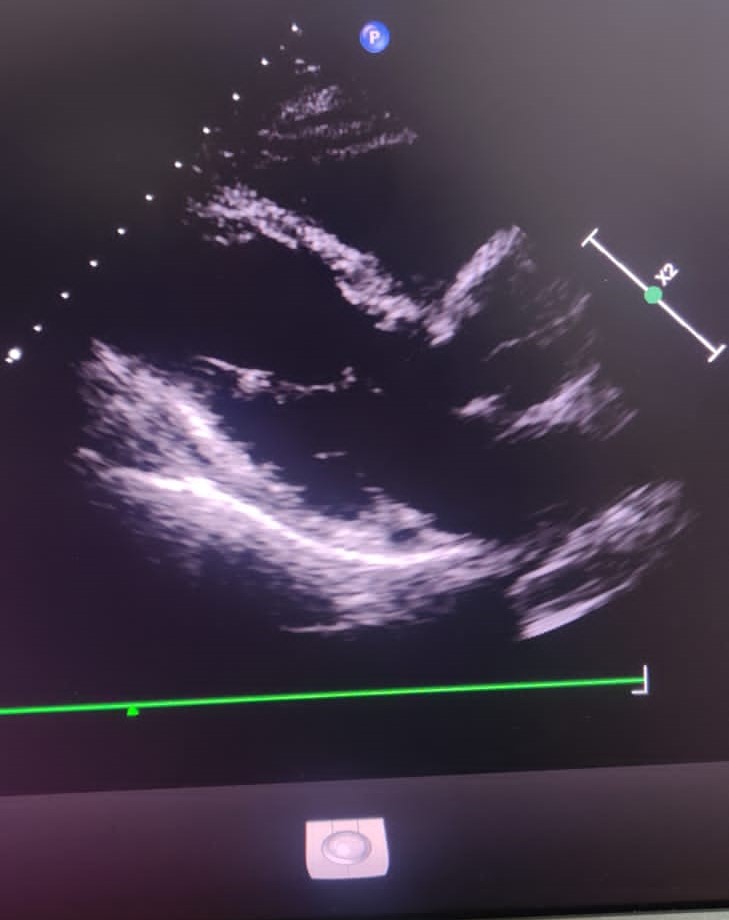
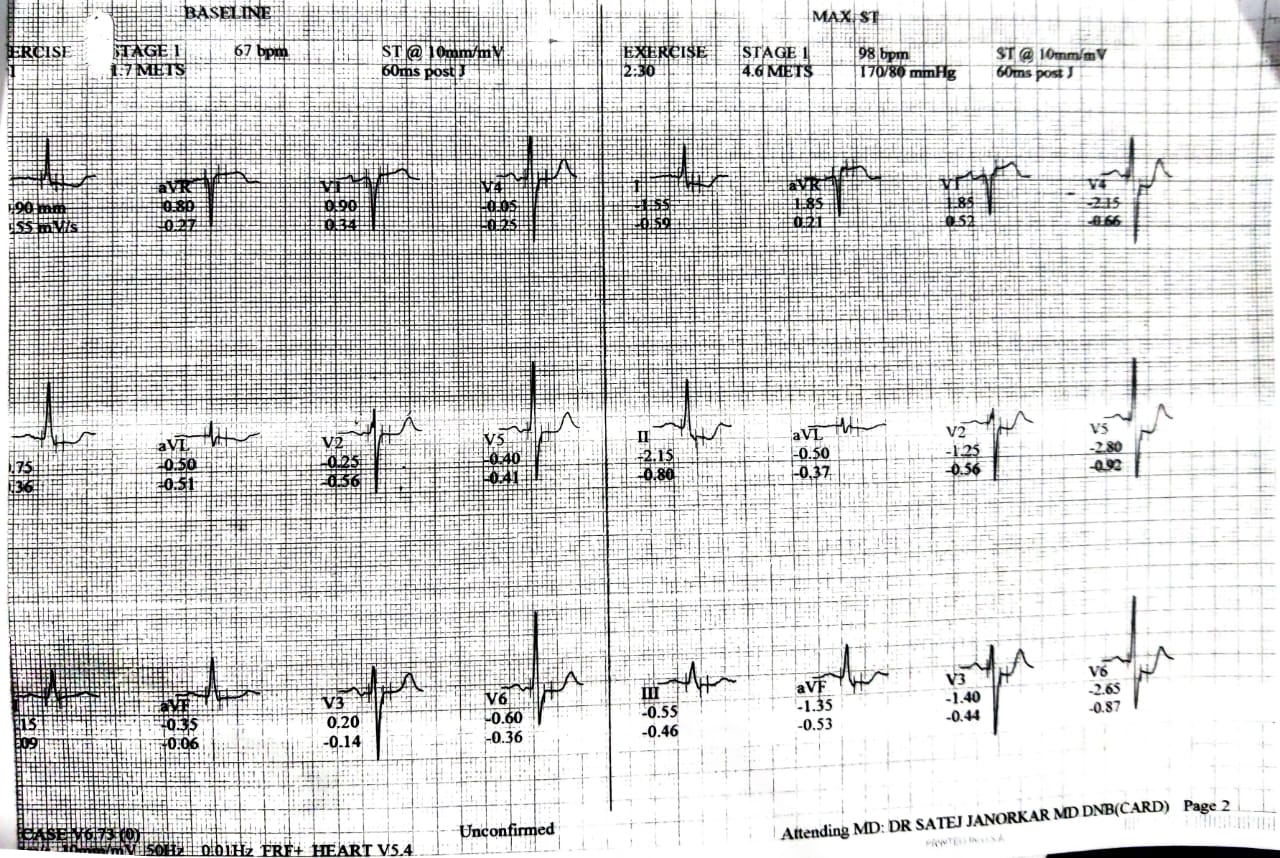
55 year old male with long standing Diabetes and with history of CABG in 2018, presented with recent onset angina and dyspnoea. Previous CABG involved LIMA to LAD, SVG to D1 and OM1 in sequential manner. TMT positive. Biochemistry normal. X Ray Normal, 2D Echo revealed LVEF - 35%.
Relevant Test Results Prior to Catheterization
Relevant Catheterization Findings
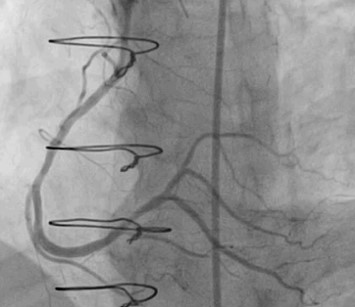
CAG: LMCA 60% stenosis distally. LAD Type III, with 80-90% discrete lesion proximally. D1 moderate sized, diffusely diseased vessel.LCX Non dominant with 80-90% lesion in OM1. RCA dominant with 30 – 40 % long plaque in mid segment. SVG to OM1 and D1 is totally occluded at the origin. LIMA to LAD is totally atretic vessel having no flow. Graft remnant from D1 to OM1 is noted.Impression: Critically double vessel coronary artery disease with totally occluded grafts.Advice: PCI to LM - LAD and LCX.
Interventional Management
Procedural Step
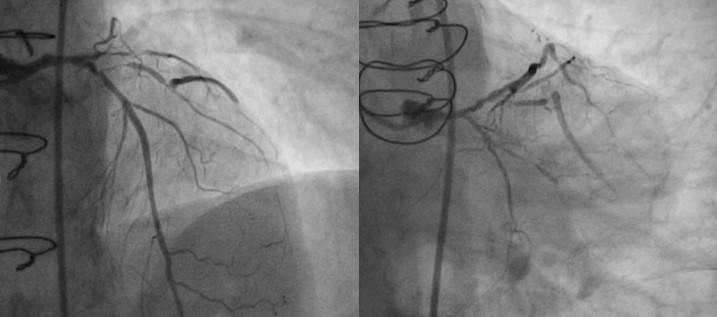
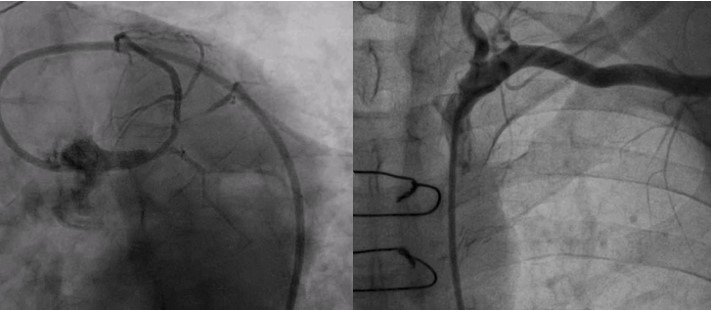
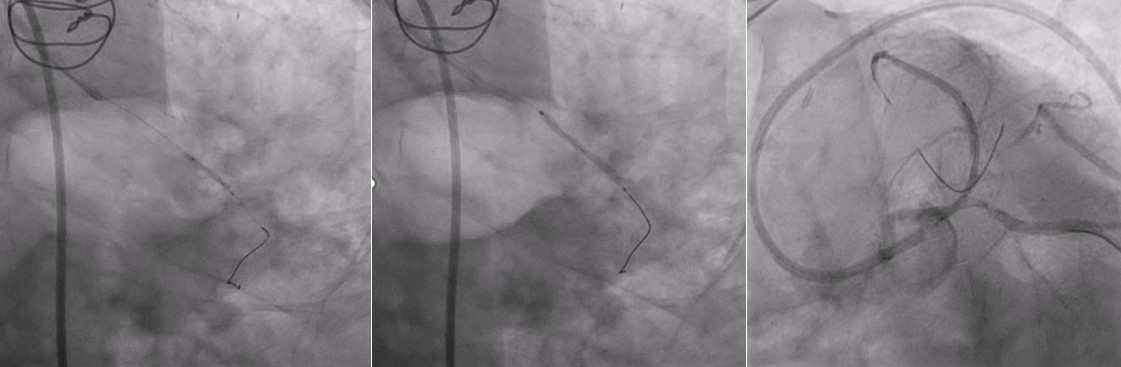
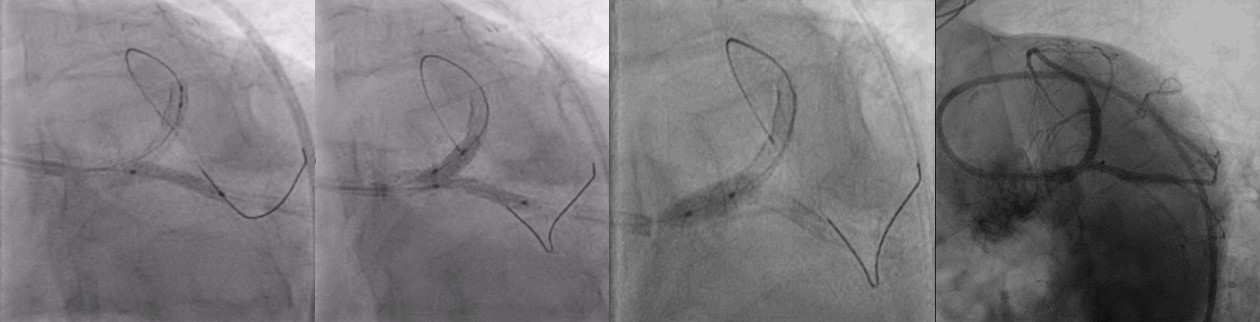
Plan: Stenting of distal LCX to enhance the flow of graft remnant in order to increase overall perfusion of Left coronary system followed by LM-LAD stenting as a provisional stenting strategy.LAD and LCX were wired with 2 hydrophobic wires. LCX lesion was predilated with 2.0x 12 mm semi compliant balloon and stented with 2.25 x 24 mm DES in OM1. LM and LAD lesions were predilated with 2.0 x 12 mm semi compliant balloon and stented with 3.00 x 32 mm DES and post dilated with 3.0 x 12 mm non compliant balloon. Left main was dilated with 4.0 x 08 mm non compliant balloon. During this intervention, ostium of LCX was stenosed significantly due to plaque shift. LCX was rewired through stent in left main and predilated with 2.0 x 12 mm semi compliant balloon. 2.50 x 12 mm DES was deployed in LCX ostium by TAP technique overlapping previously deployed stent in OM1. Stent in left main and LCX were dilated with final kissing balloon technique. Proximal part of left main was post dilated with 4.0 x 08 mm non compliant balloon POT technique.

Case Summary
LM stenosis is present in 4 - 6% of patients.PCI of ULMCA is 0.7 – 1.3%.Graft remnant assisted LM-PCI (GRA-ULMCA) has not been documented in literature.Redo CABG surgery remains equipoised option if patient is willing for the same. Initial stenting of LCX enhanced the graft remnant flow which improved overall perfusion of Left coronary system.Graft flow acted as collateral circulation which reduced the duration of ischaemia while inflating balloon / stent in LM, which also avoided the use of IABP in this case (LVEF - 35%) Although, provisional stenting remains better strategy for distal LM - Bifurcation stenosis, TAP technique proved to be a better two stent strategy after plaque shift.