
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-137
Two-Dimension Kinking JL Catheter Trapped at Upper Right Radial Artery During Diagnostic Procedure: A Safe Way for Removal
By Hung Ngo
Presenter
Hung Ngo
Authors
Hung Ngo1
Affiliation
Cho Ray Hospital, Vietnam1,
View Study Report
TCTAP C-137
Coronary - Complication Management
Two-Dimension Kinking JL Catheter Trapped at Upper Right Radial Artery During Diagnostic Procedure: A Safe Way for Removal
Hung Ngo1
Cho Ray Hospital, Vietnam1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
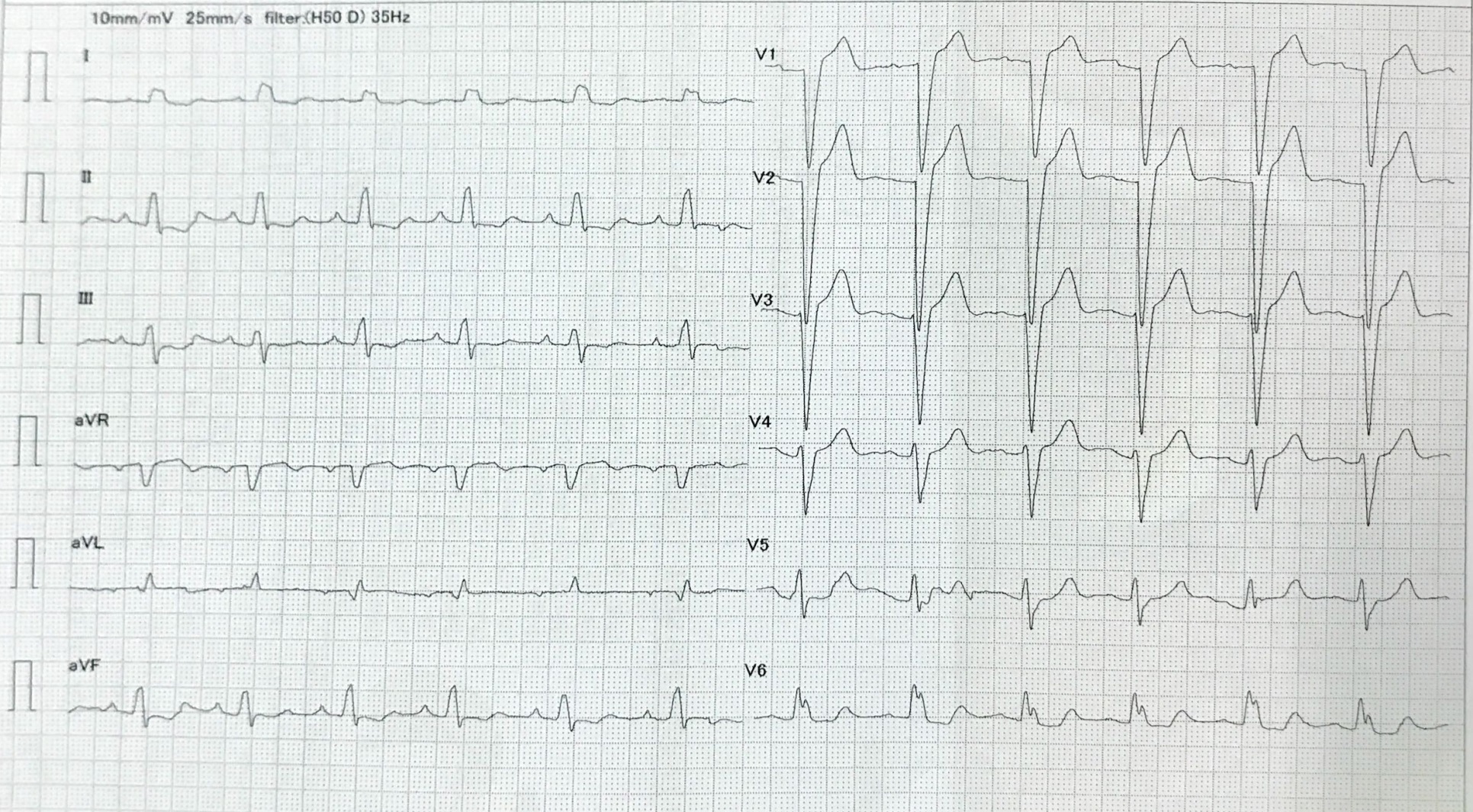
A 44-year-old male patient presented at an outpatient clinic with stable angina, classified as Canadian Cardiovascular Society (CCS) class III, despite being on optimal medical therapy. His cardiovascular risk factors included a history of smoking, dyslipidemia, and hypertension. Previous EKG showed normal sinus rhythm with complete LBBB (Figure 1). The clinical examination revealed no significant abnormalities. Coronary angiography was indicated for further diagnostic evaluation.
Relevant Test Results Prior to Catheterization
The left ventricular ejection fraction was 30% with global hypokinesia. The JL 3.5 5F diagnostic catheter was kinked at the axillary artery while engaging the left main trunk. Attempts to remove the catheter into the radial artery resulted in further twisting lodged at the upper right radial artery. Attempts to snare the JL catheter from femoral artery were failed, as the catheter tip was deeply clasped into the artery wall. The patient developed vasovagal reponse while the attempts (Figure 2).
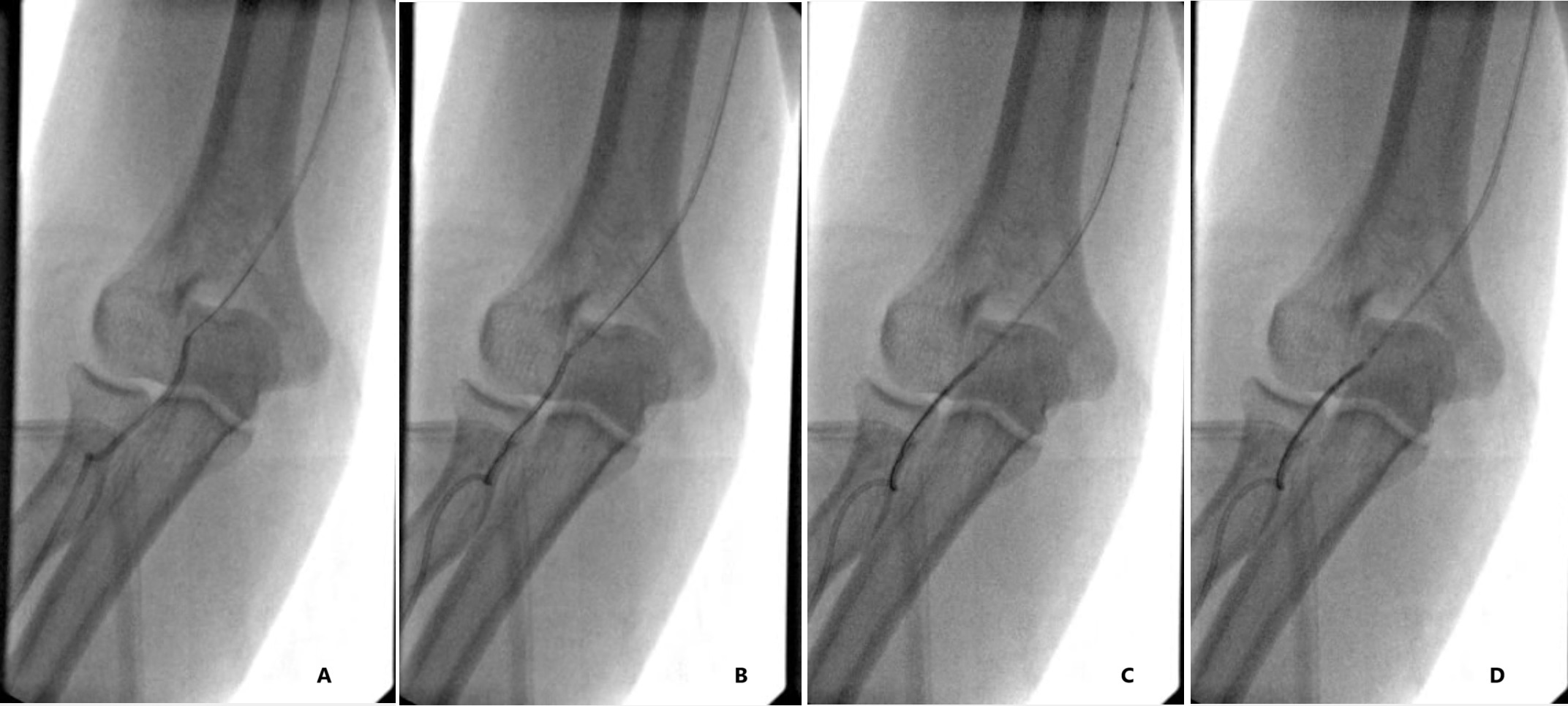
 Figure 2. Kinkking removing with wire and balloon.jpg
Figure 2. Kinkking removing with wire and balloon.jpg
Relevant Catheterization Findings
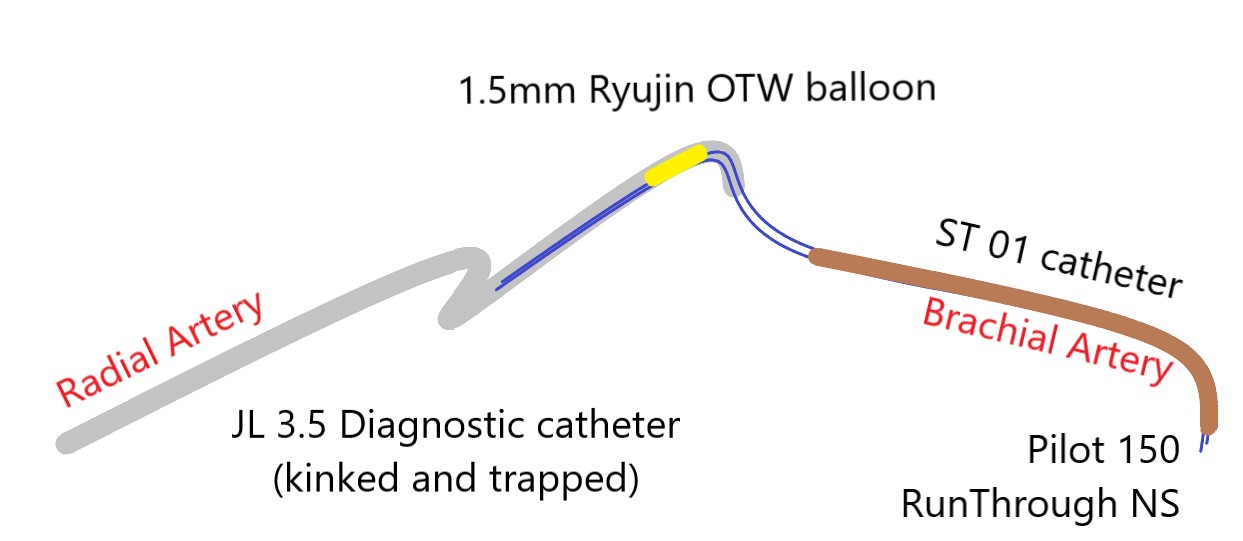
The failure to retrieve the JL catheter with snares led us to consider other techniques. A Pilot 150 and a Runthrough NS wire loaded into a 5F ST 01 catheter were used to locate the JL tip. Retrograde trapping with a 1.5 OTW Ryujin balloon was successfully performed, stretching and pulling the JL tip back into the axillary artery. This maneuver unlocked the kinked segment, allowing a 0.035" hydrophilic guide wire to cross it, and the damaged catheter was retrieved uneventfully (Figure 3).
Interventional Management
Procedural Step
Attempts to unlock the trapped JL 3.5 5F catheter were unsuccessful despite multiple efforts. The diagnostic JL catheter could not move forward and backward anymore. The patient developed hypotention and vasovagal response due to the pain at right hand.A femoral approach was accessed and a multi-purpose catheter (MP 5F; 100cm) was first used with a snare but it's not long enough to reach right elbow from right groin. Hence, a ST 01 5F 120cm was then used for snaring. Although the trapped catheter was captured, it could not be pulled back and stretched due to the JL tip being deeply clasped into the radial artery wall. The patient again experienced a vasovagal response during the attempt to pull the JL catheter into the right brachial artery, causing the snare to slip from the trapped catheter (Figure 4).The failure to retrieve the JL catheter retrogradely using snares prompted consideration of alternative techniques, including minimally invasive or surgical procedures. A Pilot 150 and a Runthrough NS wire loaded into a 5F ST 01 catheter were used to locate the JL tip. Retrograde trapping with a 1.5 OTW Ryujin balloon was successfully performed. This maneuver allowed the JL tip to be stretched and pulled back into the axillary artery, thereby unlocking the kinked segment. A 0.035" hydrophilic guide wire was then used to cross the kinked segment,and the damaged catheter was retrieved without consequences (Figure 5).

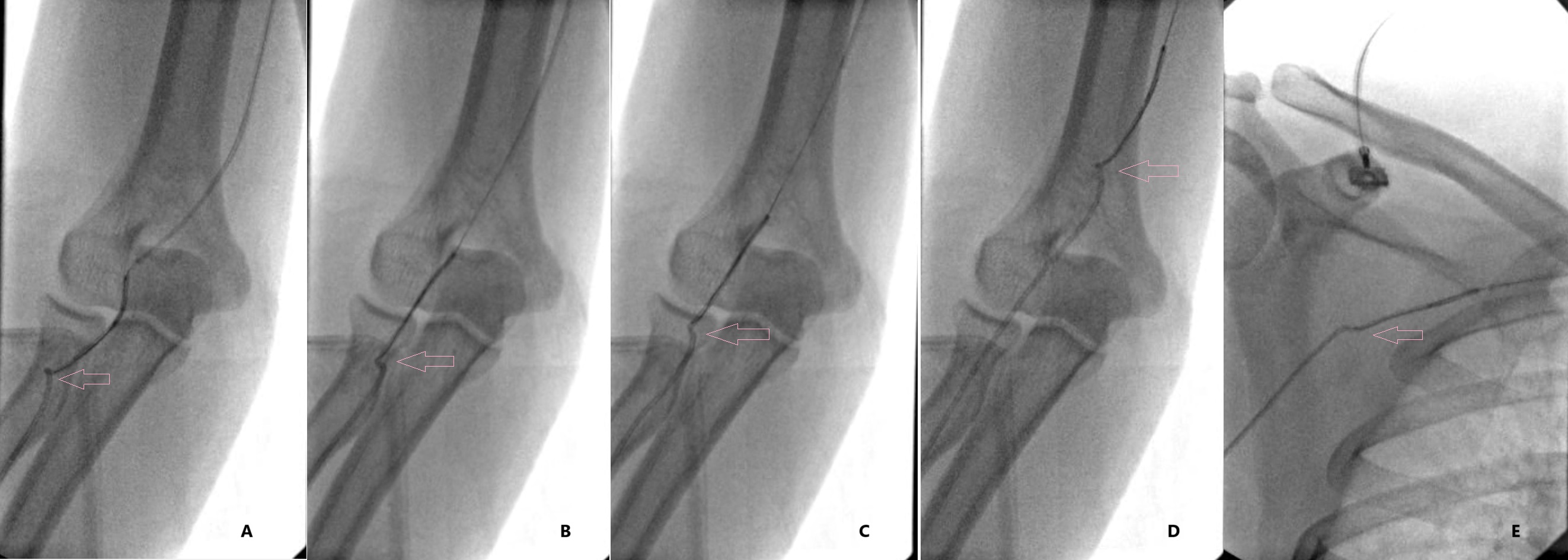
Figure 5. Kinkking removed with wire and balloon to untwist.jpg
Case Summary
A kinked and entrapped catheter often arises from excessive rotation within a tortuous vessel in the absence of a guide wire. This scenario necessitates meticulous and strategic maneuvers to mitigate severe systemic and vascular complications, particularly in small vessels such as the radial artery during trans-radial procedures. Retrograde trapping of the catheter tip with a balloon and guide wire is an effective method for stretching the clasped tip and releasing the kinked segment. This technique serves as a viable alternative when conventional retrieval methods prove unsuccessful.