
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-105
Navigating the Cross-Border Challenge: Managing Right Coronary Artery In-Stent Restenosis With Ostial Protrusion and Stent Deformation
By Mohd Ridzwan Jamaluddin, Aaron Hean Jin Ong, Jian-Chen Lim
Presenter
Mohd Ridzwan Jamaluddin
Authors
Mohd Ridzwan Jamaluddin1, Aaron Hean Jin Ong1, Jian-Chen Lim1
Affiliation
Sultan Idris Shah Hospital, Malaysia1,
View Study Report
TCTAP C-105
Coronary - Complex PCI - In-Stent Restenosis
Navigating the Cross-Border Challenge: Managing Right Coronary Artery In-Stent Restenosis With Ostial Protrusion and Stent Deformation
Mohd Ridzwan Jamaluddin1, Aaron Hean Jin Ong1, Jian-Chen Lim1
Sultan Idris Shah Hospital, Malaysia1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
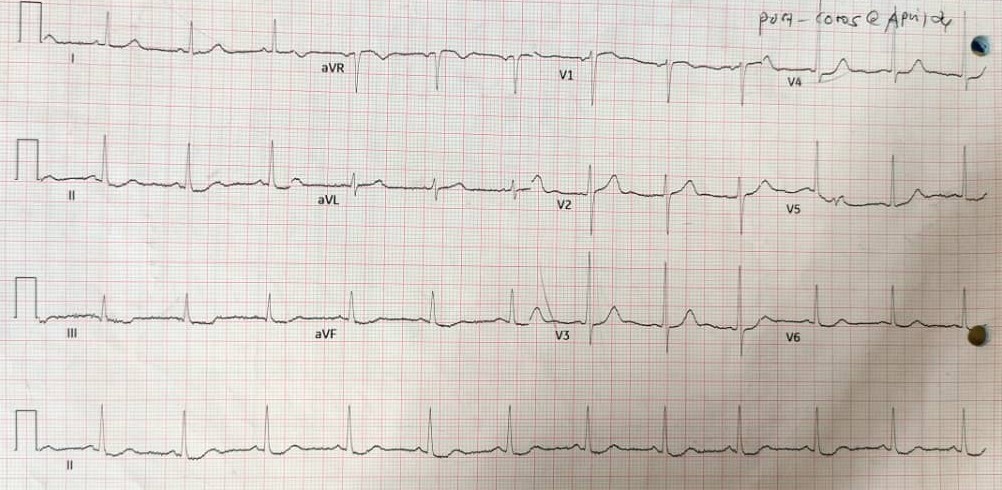
A 47-year-old diabetic Bangladeshi male with prior two-vessel disease history, PCI was done abroad about 4 months prior. He came to Malaysia, working as contract labourer, with financial limitation. Patient presented with typical anginal chest pain, similar to prior event, and relieved by GTN. ECG showed ST depression at II, III, and aVF, and patient was diagnosed with NSTEMI. Exam revealed stable vitals, physical examination was unremarkable. He was admitted to ward and send for PCI urgently.
Relevant Test Results Prior to Catheterization
Renal profile : Creatinine 89 µmol/L, Urea2 mmol/L, Na 136 mmol/L, K 3.7 mmol/L, eGFR >90 mL/min/1.73m².Troponin I : 119 ng/L (elevated).
Relevant Catheterization Findings
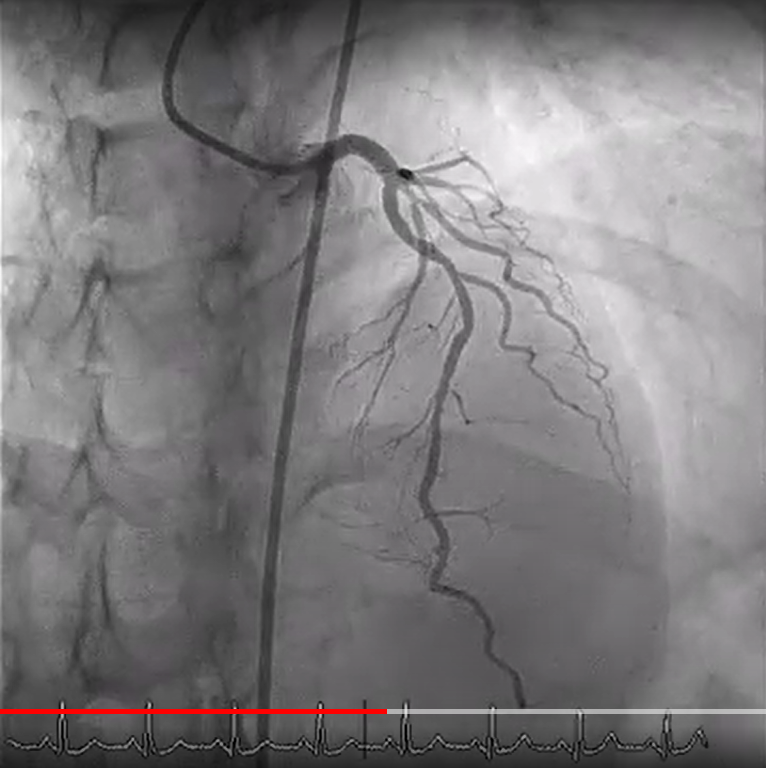
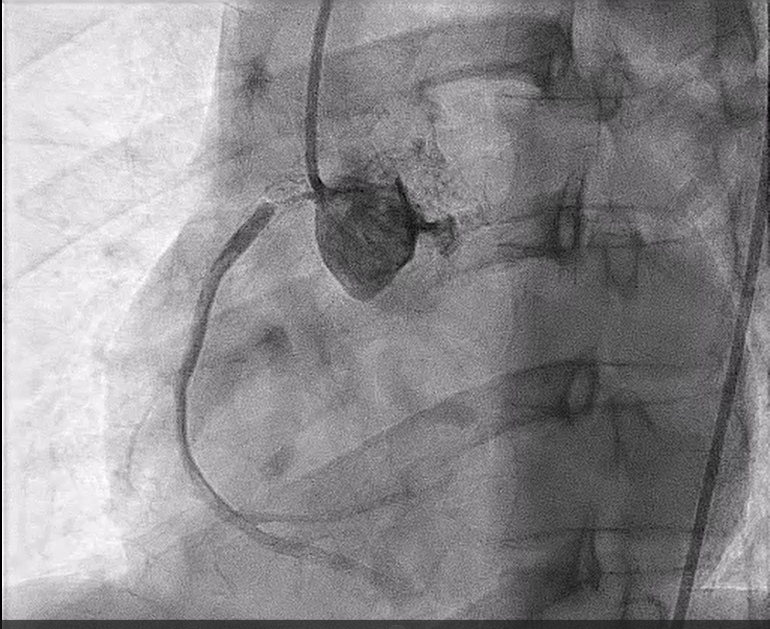
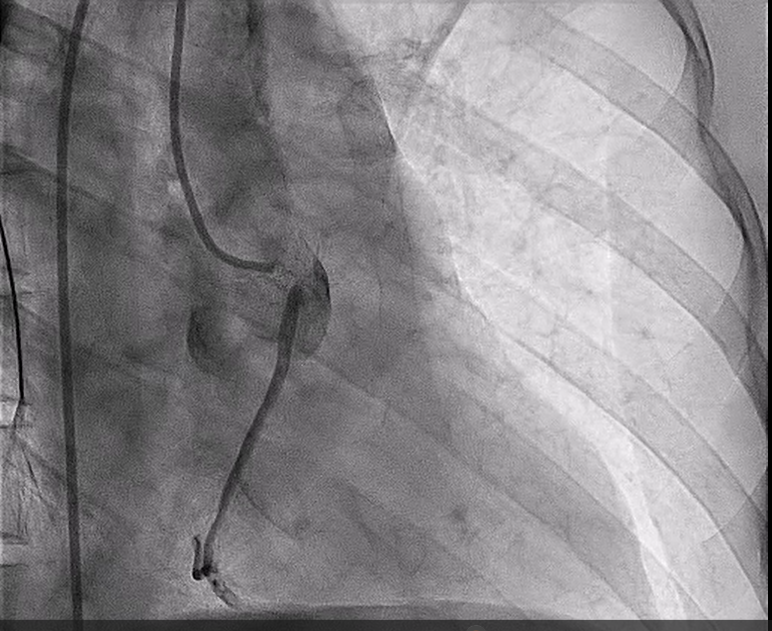
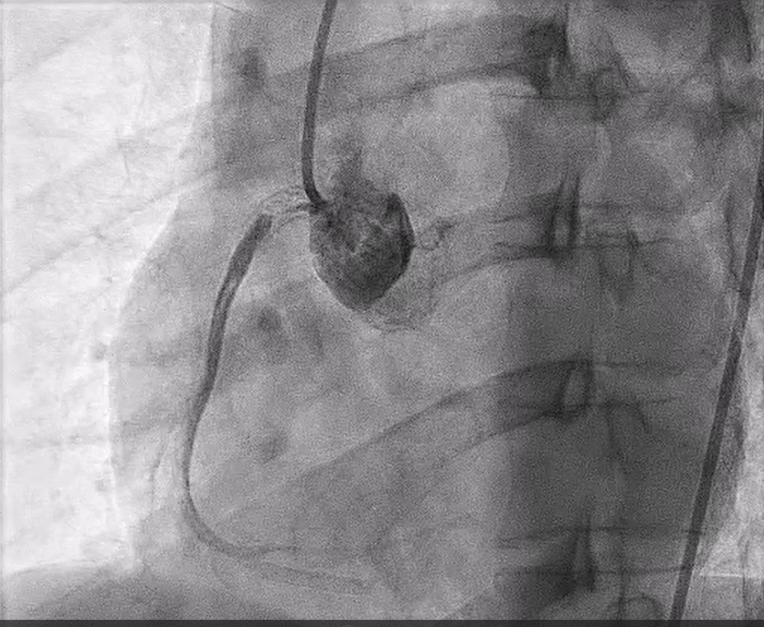
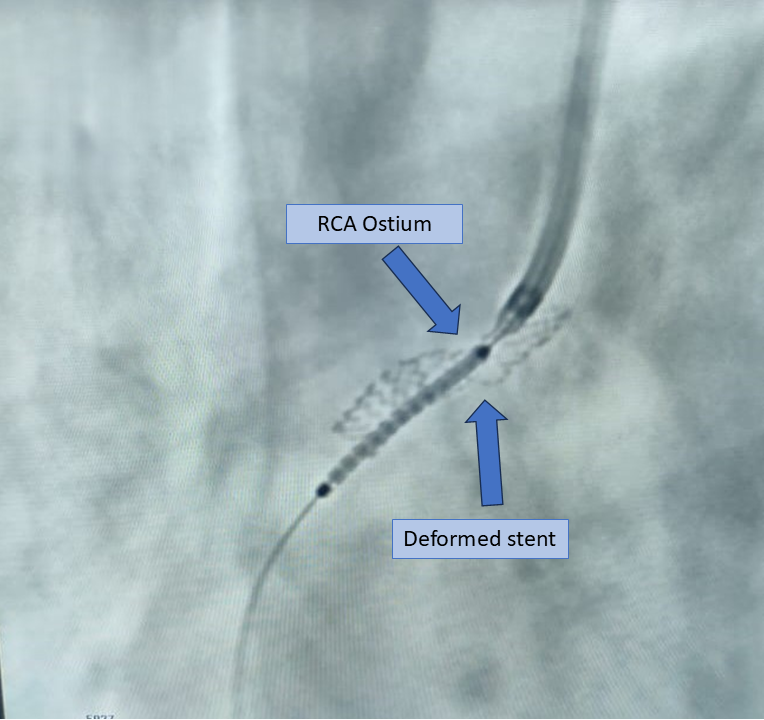
The previous PCI was done abroad, no formal result or PCI notes available, patient was unsure about the exact findings. Coronary angiogram was challenging due to difficult engagement of RCA. After careful engagement, RCA showed ISR at ostial to proximal area, Mehran class III (proliferative). There was significant stent protrusion estimated around 8mm into the aorta with deformation mid stent. Left anterior descending artery (LAD) and Left circumflex artery (LCX) showed mild disease.
Interventional Management
Procedural Step
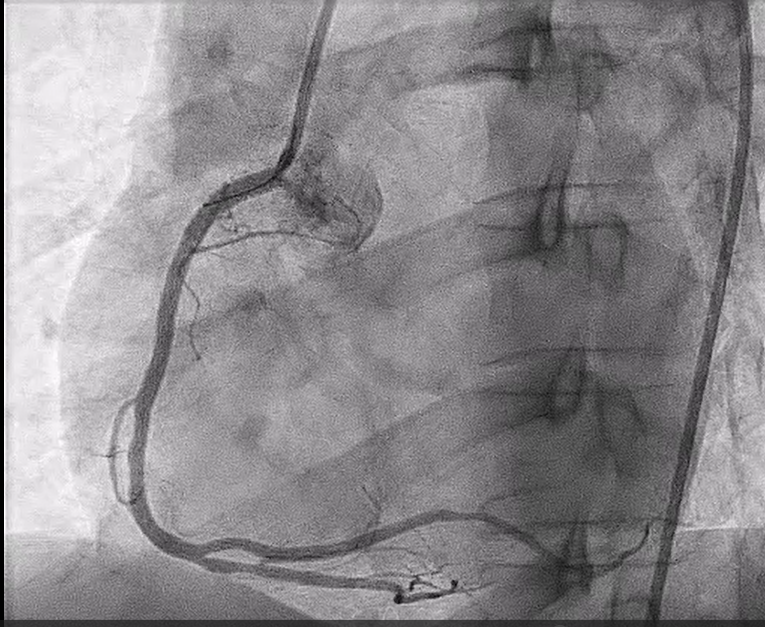
This PCI addressed a challenging case of significant in-stent restenosis (ISR), where the prior stent protruded into the aorta and deformed, almost completely obstructing blood flow to RCA.
Case Summary
This PCI case highlights the importance of a structured approach to complex in-stent restenosis (ISR), especially when mechanical stent issues are present. Preventing similar complications in the future requires thorough pre-procedural strategy, usage of imaging such as intracoronary imaging (IVUS/OCT) whenever possible, proper usage of DCB or DES, and careful catheter navigation to avoid further stent damage is crucial. High-pressure ballooning and the use of DES remain effective in managing ISR. Each case enriches our strategies for complex ISR, ensuring even high-risk cases are managed with precision and confidence.