
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-151
Entrapped Coronary Guidewire Knot
By Chi Na Cheng, Chi Wing Wong, Shung Yee Wong, Tsz Ho Chan
Presenter
Chi Na Cheng
Authors
Chi Na Cheng1, Chi Wing Wong1, Shung Yee Wong1, Tsz Ho Chan1
Affiliation
Pok Oi Hospital, Hong Kong, China1,
View Study Report
TCTAP C-151
Coronary - Complication Management
Entrapped Coronary Guidewire Knot
Chi Na Cheng1, Chi Wing Wong1, Shung Yee Wong1, Tsz Ho Chan1
Pok Oi Hospital, Hong Kong, China1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A 68 years old chronic smoker has history of diabetes, hypertension, and hyperlipidemia.
He presented with 2 weeks history of chest discomfort.
On physical examination, he has stable vital signs, chest clear, normal heart sounds with no murmur, and no peripheral edema

He presented with 2 weeks history of chest discomfort.
On physical examination, he has stable vital signs, chest clear, normal heart sounds with no murmur, and no peripheral edema
Relevant Test Results Prior to Catheterization
ECG showed sinus rhythm
Echocardiogram showed normal chambers size, LV ejection fraction of 51% with hypokinesia over inferolateral wall.
Relevant Catheterization Findings
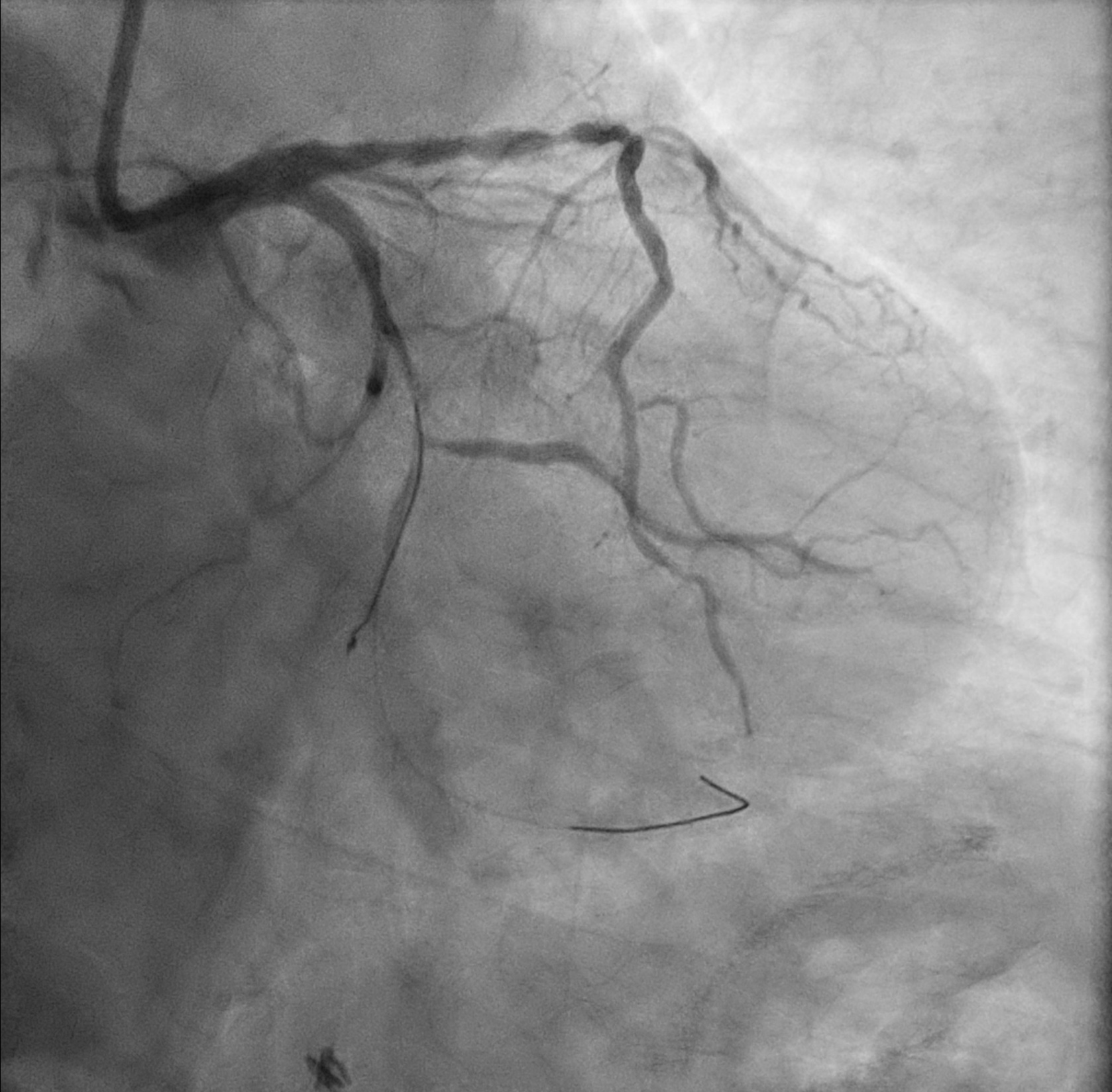
Coronary angiogram- Left main: normal- LAD: p-mLAD diffuse severe stenosis- LCx: mLCx total occlusion, dLCx supplied by septals- RCA: Dominant, pRCA diffuse mild to moderate stenosis, mRCA focal severe stenosis.
Interventional Management
Procedural Step
Left main was engaged with 7F EBU 3.5. Attempt wiring to mLCx total occlusion by Runthrough NS and Fielder XT-A with Caravel support but failed. mLCx finally wired with Gaia Next 1 and switched to Runthrough NS. Predilation to mLCx with Sapphire 1.0/15 and Ryurei 2.0/15.
After dilation to mLCx, runthrough NS wire knuckled in dLCx and failed to be straightened up. Another Runthrough NS wired to dLCx with Crusade Type R catheter.
On removal of the knuckled runthrough NS, it was stucked in ventricular branch. Cine confirmed coronary guidewire knot was formed.
Attempted removal with caravel but failed.Attempted wiring to ventricular branch for ballooning but failed.
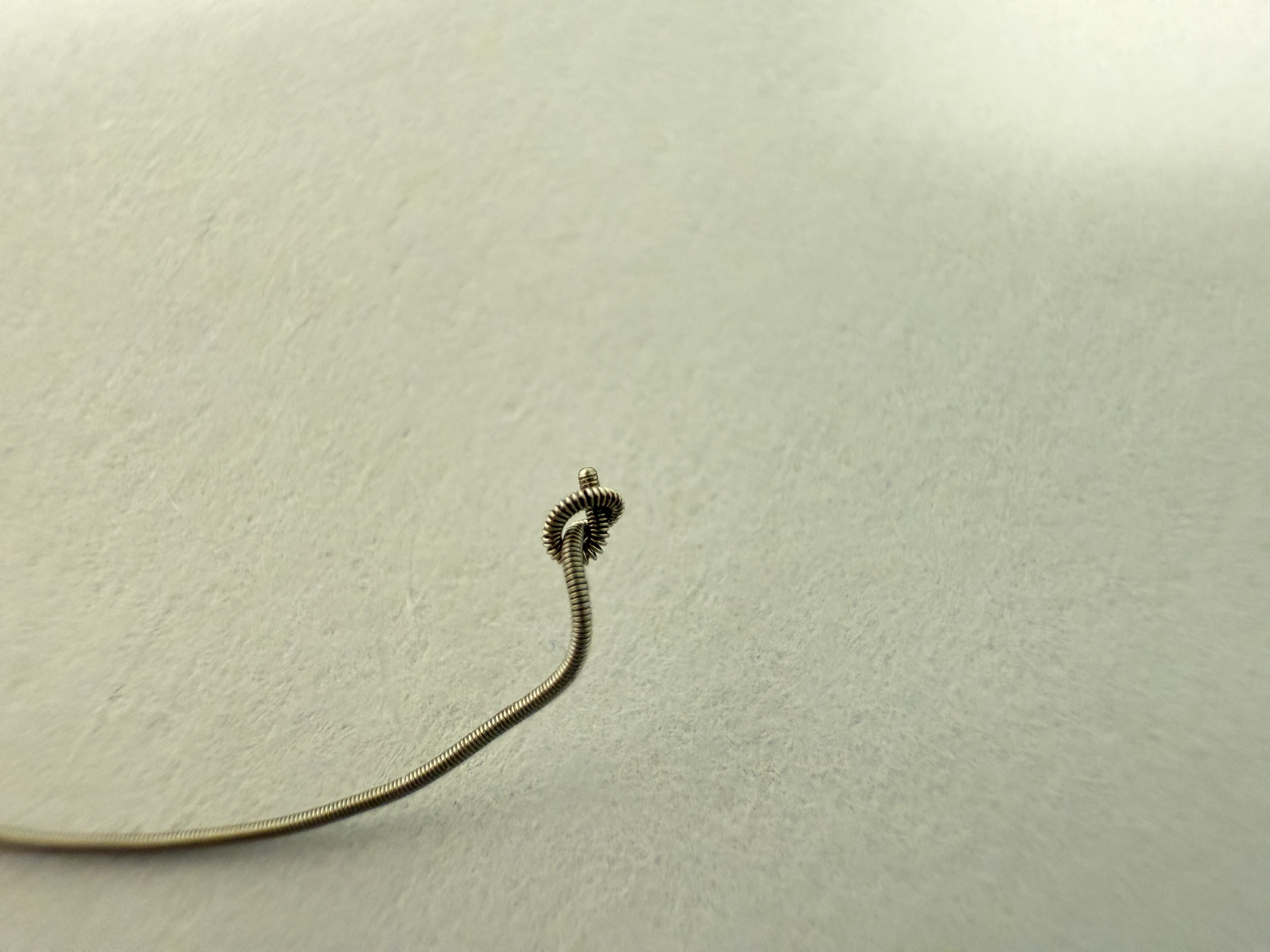
Finally trapped knotted guidewire was removed with Turnpike.
dLCx and OM1 were rewired. After serial dilatation, OM1 was treated with DEB Magic Touch at 8atm for 1 min, and dLCx was treated with DEB Pantera Lux 2.0/15 at 7atm for 1 min.Ostial to mLCx was stented with Orisiro Mission 2.5/35 at 10atm. POT with NC Pantera LEO 4.0/8 at 12atm.
Final angiogram showed good result.
After dilation to mLCx, runthrough NS wire knuckled in dLCx and failed to be straightened up. Another Runthrough NS wired to dLCx with Crusade Type R catheter.
On removal of the knuckled runthrough NS, it was stucked in ventricular branch. Cine confirmed coronary guidewire knot was formed.
Attempted removal with caravel but failed.Attempted wiring to ventricular branch for ballooning but failed.
Finally trapped knotted guidewire was removed with Turnpike.
dLCx and OM1 were rewired. After serial dilatation, OM1 was treated with DEB Magic Touch at 8atm for 1 min, and dLCx was treated with DEB Pantera Lux 2.0/15 at 7atm for 1 min.Ostial to mLCx was stented with Orisiro Mission 2.5/35 at 10atm. POT with NC Pantera LEO 4.0/8 at 12atm.
Final angiogram showed good result.
Case Summary
Guidewire knot entrapment is a rare complication and is better to be avoided.
Bailout solution includes traction with microcatheter and guide extension support.
Other solutions include parallel wire for balloon dilatation of the entrapment site, with or without a second guiding catheter.
Forcefully pulling the wire may result in retained fractured guidewire.
In our case, the entrapped guidewire knot was retrieved successfully with gentle traction with microcatheter support for en-bloc removal.
Bailout solution includes traction with microcatheter and guide extension support.
Other solutions include parallel wire for balloon dilatation of the entrapment site, with or without a second guiding catheter.
Forcefully pulling the wire may result in retained fractured guidewire.
In our case, the entrapped guidewire knot was retrieved successfully with gentle traction with microcatheter support for en-bloc removal.