
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-196
Real-Time IVUS Guided Ostial Stenting
By Jonathan Gabriel Sung
Presenter
Jonathan Gabriel Sung
Authors
Jonathan Gabriel Sung1
Affiliation
Tuen Mun Hospital, Hong Kong, China1,
View Study Report
TCTAP C-196
Coronary - Imaging & Physiology - Invasive Imaging (IVUS, OCT, NIRS, VH, etc)
Real-Time IVUS Guided Ostial Stenting
Jonathan Gabriel Sung1
Tuen Mun Hospital, Hong Kong, China1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
We report a case of 72-year-old gentleman who was a chronic smoker with history of hypertension, diabetes mellitus and adenocarcinoma of lung status post open left pneumonectomy seven years ago. He was admitted to our unit for acute pulmonary oedema after presenting with sudden onset of dyspnoea at night. Physical examination revealed blood pressure of 141/60 mmHg and heart rate 94 bpm with crepitation over right lung base. He required high flow oxygen via CPAP at the emergency department.
Relevant Test Results Prior to Catheterization
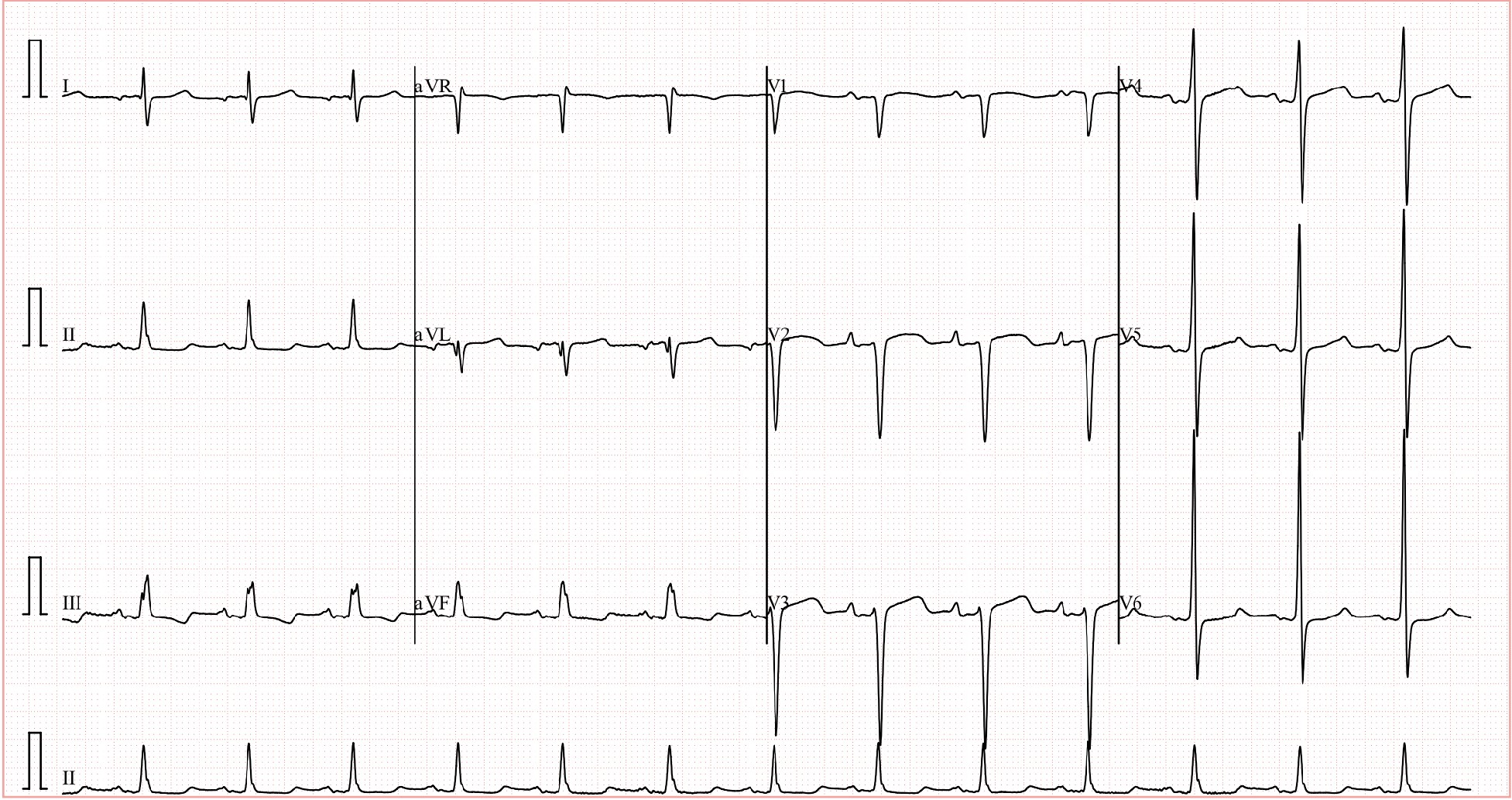
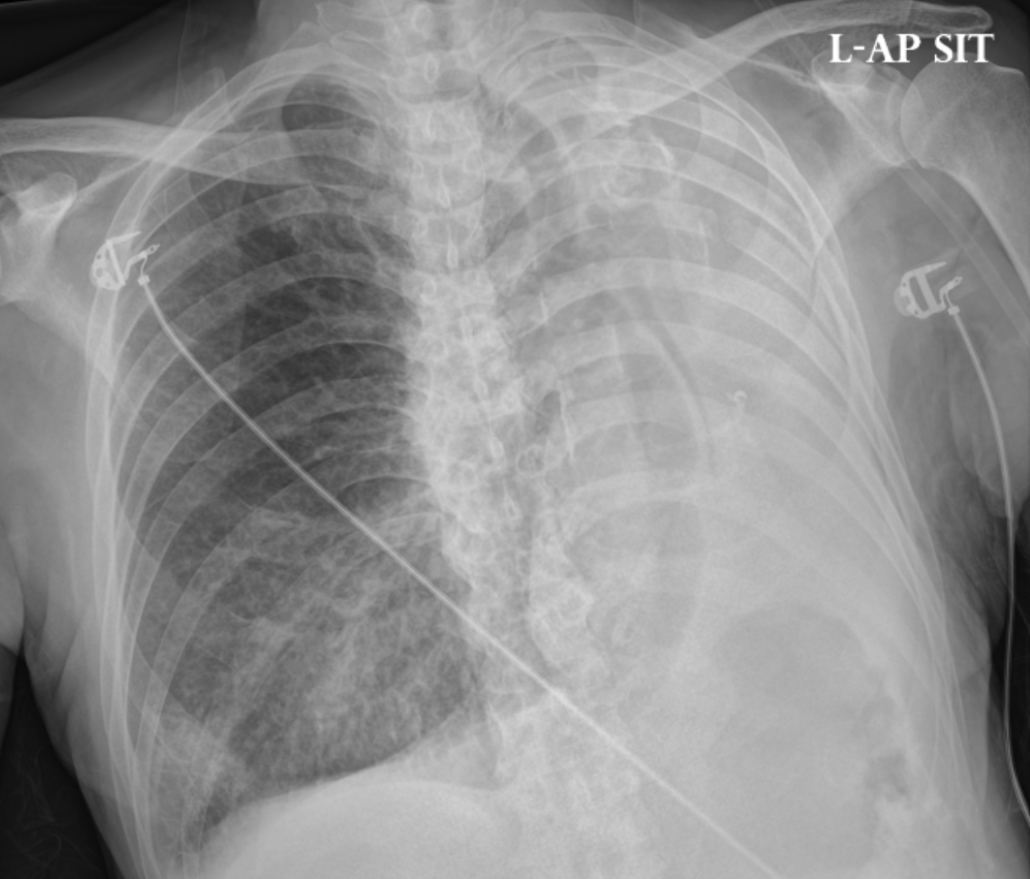
Electrocardiogram showed sinus rhythm with left ventricular hypertrophy by voltage and poor R wave progression. Chest radiograph revealed congestion over right lung basal region and evidence of left pneumonectomy. Blood tests were remarkable for mildly elevated troponins. Echocardiogram showed normal left ventricular systolic function with estimated left ventricular ejection fraction of 55%, no regional wall motion abnormality and structurally normal valves.
Relevant Catheterization Findings
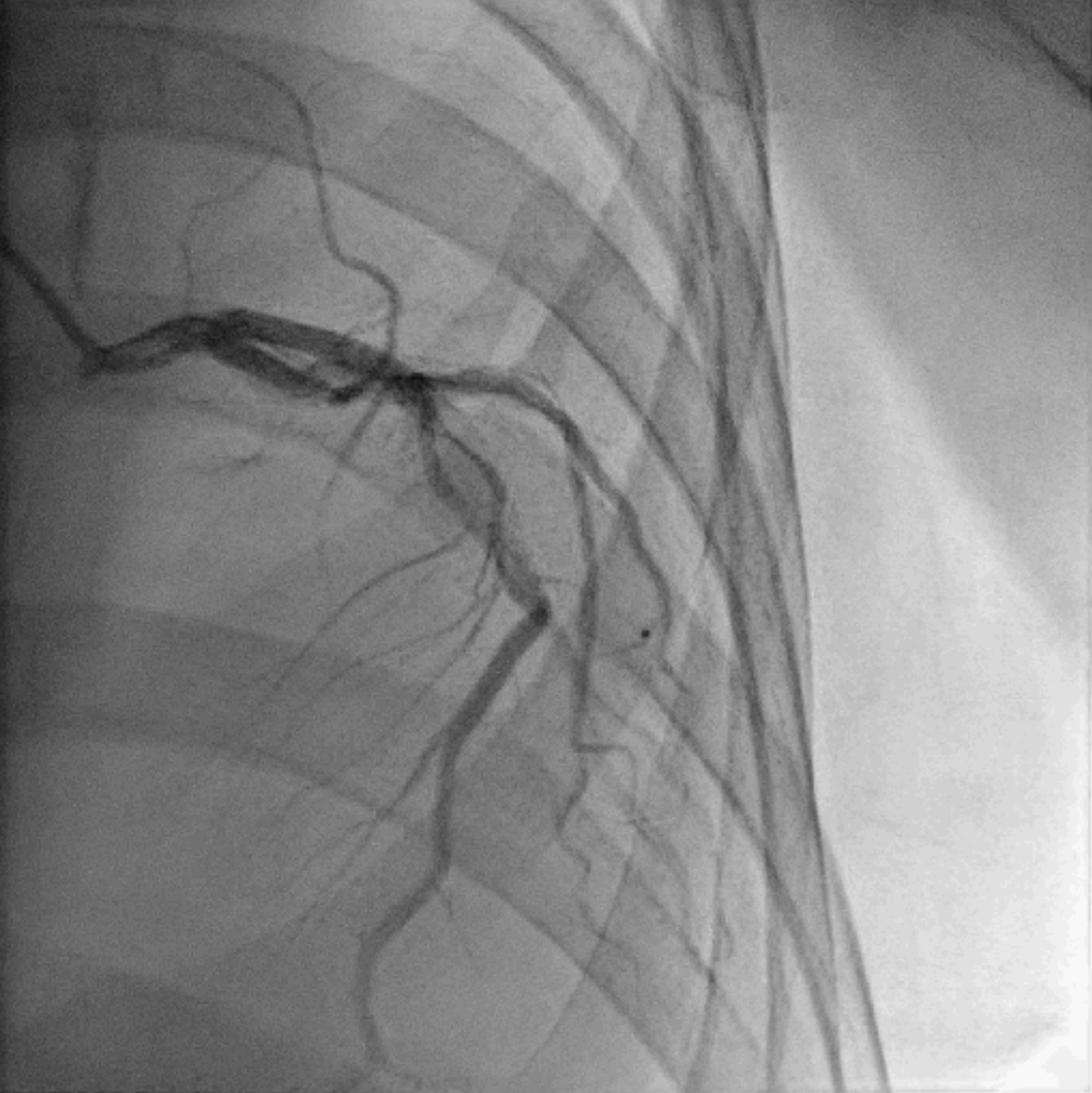
Patient was brought to the catheterization laboratory after initial stabilization. Coronary angiogram showed distorted coronary courses due to previous pneumonectomy, heavily calcified left coronary system with critical disease over mid-LAD and mid-LCx, and minor disease over dominant RCA. After off-table detailed discussion with both patient and family, decision was made to move forward with LAD intervention first, and then consider intervening LCx if patient remained symptomatic.

Interventional Management
Procedural Step
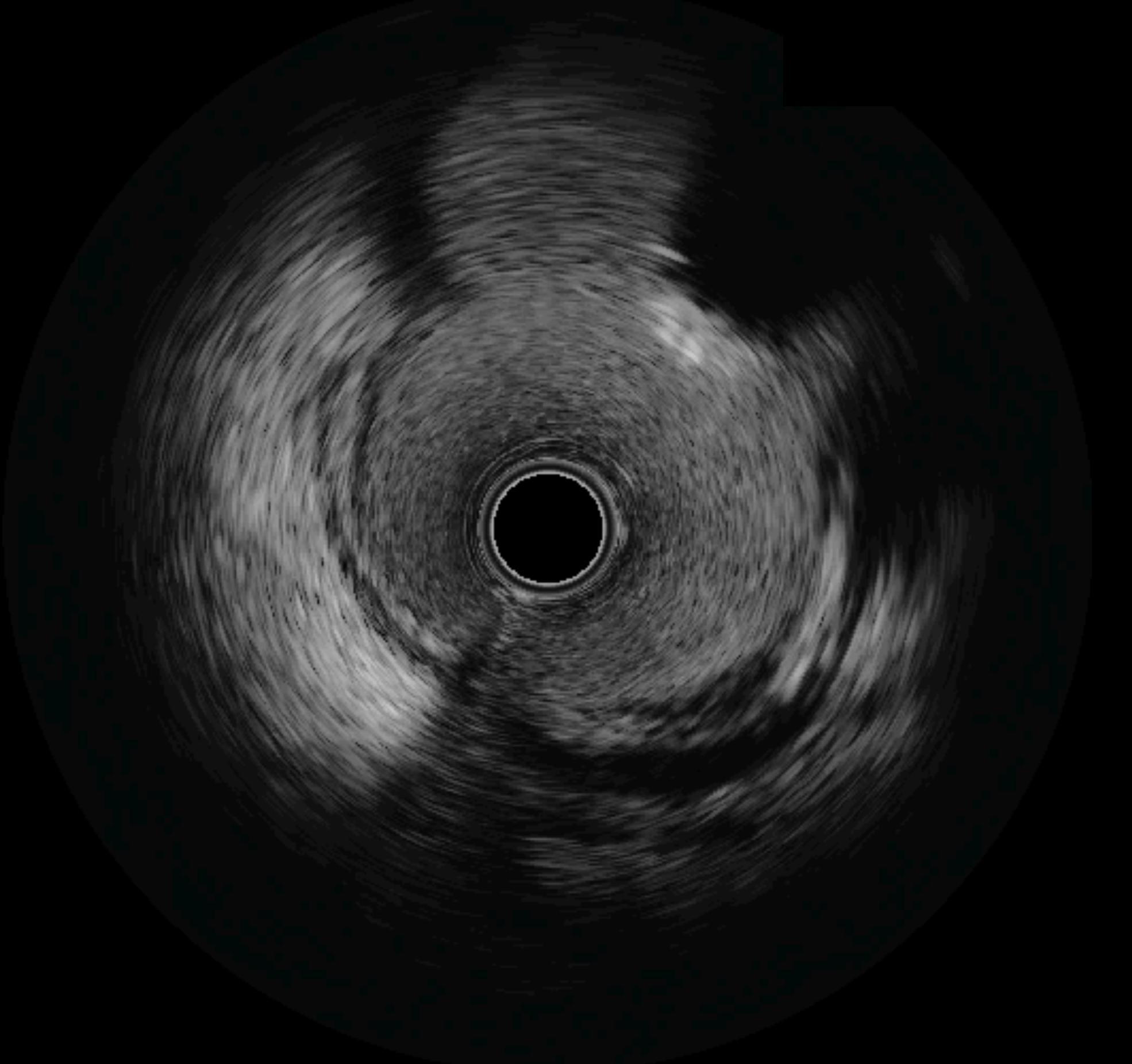
Patient returned to the catheterization laboratory for LAD intervention. Right common femoral artery access was obtained under ultrasound and fluoroscopy guidance. Long sheath was inserted due to tortuous aorta. Left main coronary artery was engaged with EBU 3.5 guide catheter. IVUS catheter failed to pass through mid-LAD calcified segment. Rotational atherectomy was performed using 1.5 mm burr at 180,000 rpm along mid-LAD. IVUS catheter was then able to cross the lesion and revealed significant circumferential calcification along mid-LAD and significant plaque extension to very proximal LAD. Intravascular lithotripsy was then performed along mid-LAD using Shockwave 2.5/12 mm and Shockwave 3.0/12 mm. Lesion was further prepared using non-compliant balloon 3.0/15 mm with full balloon expansion achieved. First diagonal artery was protected with jailed semi-compliant balloon 1.5/15 mm. A drug eluting stent 3.0/48 mm was deployed over proximal-distal LAD at nominal pressure.
Workhorse wire was removed from first diagonal after good flow confirmed and threaded into LCx. IVUS catheter was parked around ostial LCx to visualize LAD ostium. Another drug eluting stent 4.0/15 mm was deployed over ostial-proximal LAD with real-time IVUS guidance. The stents were optimized using 3.5 mm, 3.75 mm and 4.0 mm non-compliant balloons. Repeated IVUS confirmed proximal stent edge landing exactly at ostial LAD without any protrusion into left main coronary artery, and excellent stents expansion.

Workhorse wire was removed from first diagonal after good flow confirmed and threaded into LCx. IVUS catheter was parked around ostial LCx to visualize LAD ostium. Another drug eluting stent 4.0/15 mm was deployed over ostial-proximal LAD with real-time IVUS guidance. The stents were optimized using 3.5 mm, 3.75 mm and 4.0 mm non-compliant balloons. Repeated IVUS confirmed proximal stent edge landing exactly at ostial LAD without any protrusion into left main coronary artery, and excellent stents expansion.
Case Summary
This case illustrates the use of real-time IVUS to guide ostial LAD stenting. While the technique is easy to perform with reproducible results, attention should be drawn to several aspects. Firstly, at least 7Fr guide is needed and some IVUS catheters might require 8Fr guide. Secondly, if the stent is significantly under-sized, there might be issue of stent elongation following post-stent high-pressure ballooning. Thirdly, result is often less ideal in bifurcations with acute angles. Finally, this technique is only suitable for medina (0,1,0) or (0,0,1) left main bifurcation, and should not be used if there is significant disease involving distal left main or the other ostium.