
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-185
Invasive Physiological Assessment of a Unique Case of Twin Coronary Anomalies
By A Shaheer Ahmed
Presenter
A Shaheer Ahmed
Authors
A Shaheer Ahmed1
Affiliation
Jawaharlal Institute of Postgraduate Medical Education and Research, India1,
View Study Report
TCTAP C-185
Coronary - Imaging & Physiology - FFR
Invasive Physiological Assessment of a Unique Case of Twin Coronary Anomalies
A Shaheer Ahmed1
Jawaharlal Institute of Postgraduate Medical Education and Research, India1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
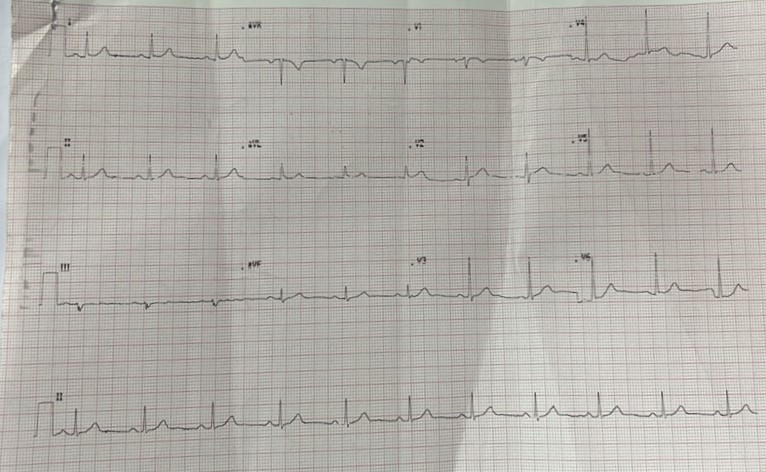
A 53-year-old male, ex-smoker, presented with angina on exertion class II for the past 6 months, which was moderate intensity. He did not have any dyspnea, palpitations or syncope. His electrocardiography was normal.
Relevant Test Results Prior to Catheterization
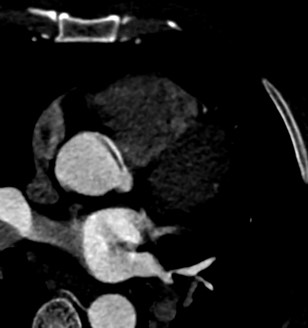
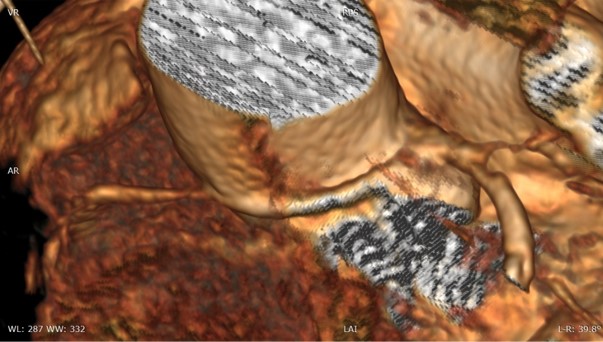
He underwent CT coronary angiogram to look forcoronary anatomy. CT revealed anomalous origin of right coronary artery from the left sinus with intramural and interarterial course and myocardial bridging in the mid part of LAD. There was around 50 % stenosis in the LAD just proximal to the bridging segment. TMT showed an exercise capacity of 7.1 METS.

Relevant Catheterization Findings
Since there were two coronary anomalies and TMT was inconclusive, we decided to proceed with an invasive physiological assessment. EBU and AL 0.75 guiding catheter ere used to engage left and right coronary arteries respectively
Interventional Management
Procedural Step
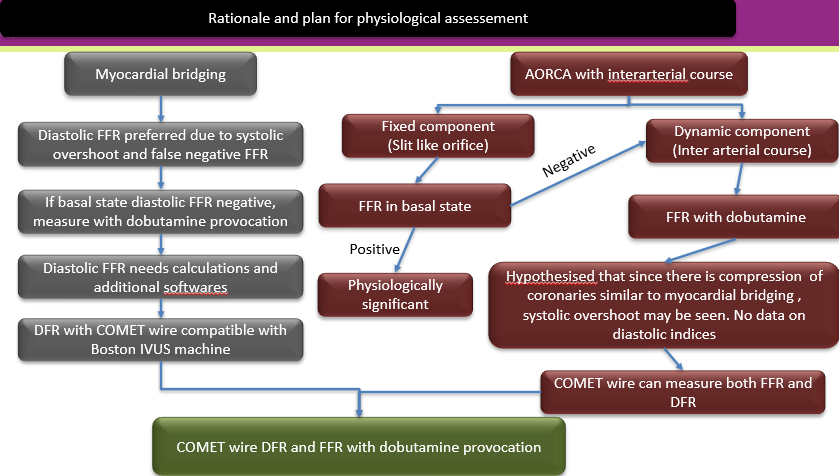
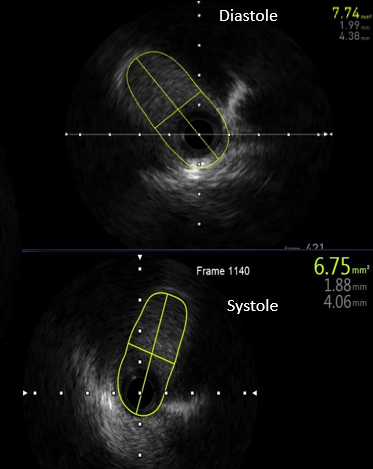
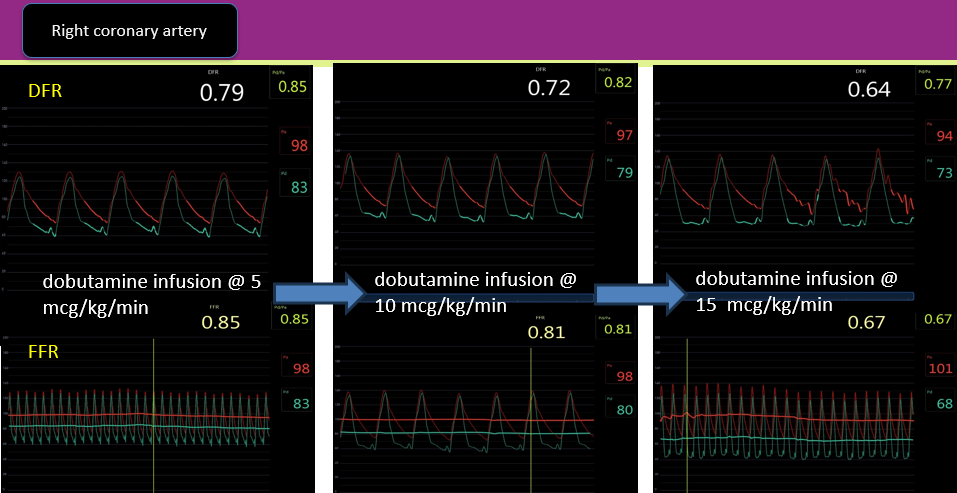
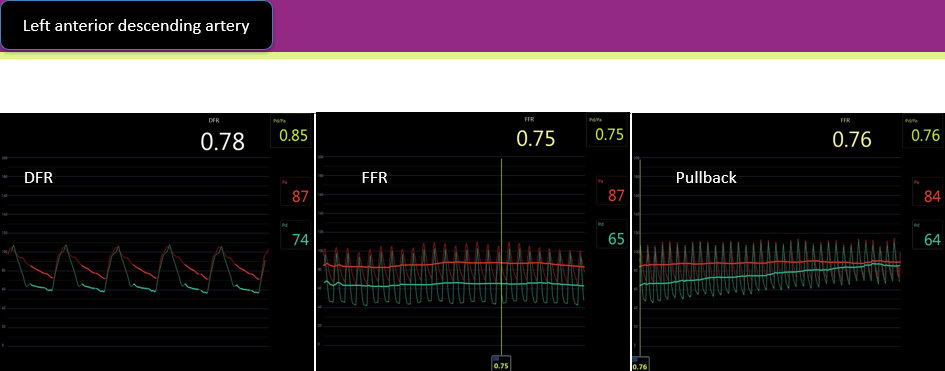
Since compression in AORCA is similar to compression in myocardial bridging, we hypothesized that diastolic measures will be affected more with systolic overshoot in AORCA too. Hence, we decided to use a COMET pressure wire since it gives a measure of both DFR and FFR. Initially we did IVUS to look at the ostium of RCA, which was elliptical, which compression during systole. The baseline pd/pa in RCA was normal (0.91). But dFR was positive, just crossing the cut-off for significant narrowing. Then we started dobutamine infusion at 5 mcg/kg/min and increased by 5 mcg/kg/min till we achieved either positive FFR or heart rate reached 120 bpm with a maximum dose of 40 mcg/kg/min. On the serial increase in dobutamine dose, we noted a progressive reduction in distal diastolic pressure, whereas systolic pressure remained unchanged. On reaching 15 mcg/kg/min, FFR also became positive, mainly due to a significant drop in diastolic pressure, which in turn reduced the distal mean pressure and hence FFR became positive. DFR across LAD bridging was also positive. Pullback of pressure revealed a drop of pressure only across the myocardial bridging segment. The patient was explained the nature of the disease and the potential benefit of CABG due to the intramural course of RCA and hemodynamically significant bridging of LAD. Due to a lack of severe symptoms, the patient opted for medical therapy.
Case Summary
He was given beta blockers titrated to heart rate along with statins/aspirin and advised to avoid nitrates. Since the patient has presented in the fifth decade,he might not be at risk of sudden death. However, CABG might help to reduce the ischemia burden. This case highlights systolic overshoot and diastolic reduction of pressure that occurs in diastole in AORCA, proving that reduced coronary perfusion pressure may be seen in AORCA, contrary to conventional belief. CT coronary angiogram should preferably be the first line of investigation in patients with stable angina unless symptoms are severe.