
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-016
The First Alarm: A Case of Early Morning STEMI Intervention
By Noor Muhammad Azlan Shah Atan, Teh Khai Chih, Ahmad Suhailan Mohamed, Danial Shaharel, Aslaniff Roslan
Presenter
Noor Muhammad Azlan Shah Atan
Authors
Noor Muhammad Azlan Shah Atan1, Teh Khai Chih1, Ahmad Suhailan Mohamed1, Danial Shaharel1, Aslaniff Roslan1
Affiliation
National Heart Institute, Malaysia1,
View Study Report
TCTAP C-016
Coronary - ACS/AMI
The First Alarm: A Case of Early Morning STEMI Intervention
Noor Muhammad Azlan Shah Atan1, Teh Khai Chih1, Ahmad Suhailan Mohamed1, Danial Shaharel1, Aslaniff Roslan1
National Heart Institute, Malaysia1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A middle-aged man with mild coronary artery disease and dyslipidemia referred to us at 8am for primary percutaneous coronary intervention. He presented earlier with left sided chest pain, crushing in nature, radiating to left arm and jaw with diaphoresis started at 7am which prompting for urgent evaluation. Initial assessment revealed that GCS full of pain score 7/10, blood pressure 197/127 heart rate 100 beat per minute lung clear and no murmur in cardiovascular assessment.
Relevant Test Results Prior to Catheterization
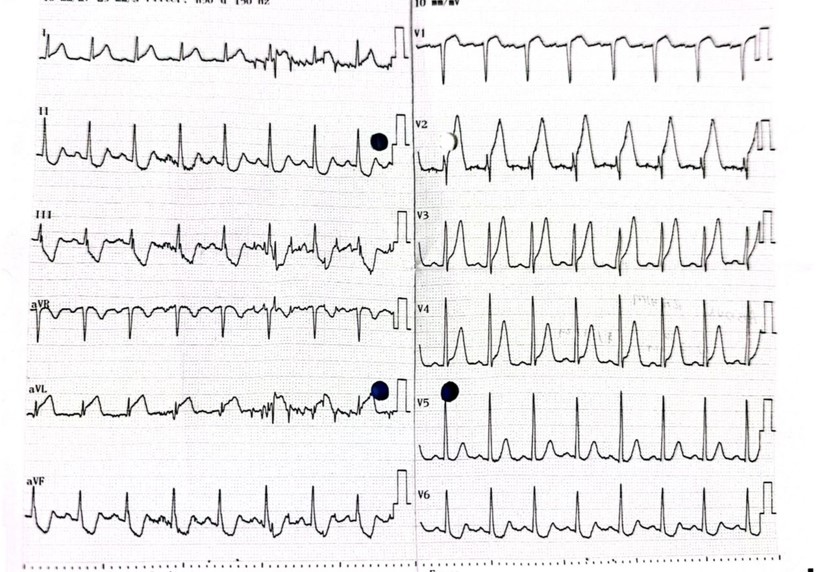
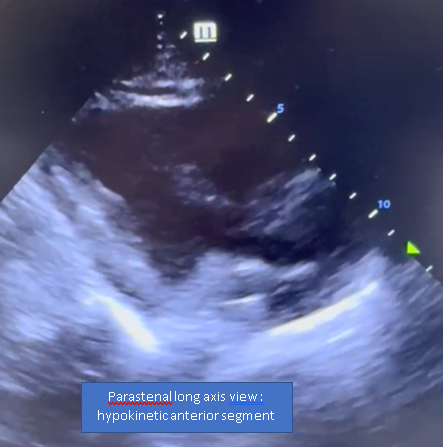
An electrocardiogram (ECG) revealed ST elevation in the anteroseptal leads and reciprocal changes in the inferior leads. Transthoracic echocardiography (TTE) showed an ejection fraction of 40% with hypokinetic anterior segments, effectively ruling out aortic dissection, mitral regurgitation, ventricular septal rupture, and pericardial effusion. Patient was classified as Killip Class I. Other investigation showed normal full blood count, renal function and liver function test. Troponin was 147.

Relevant Catheterization Findings
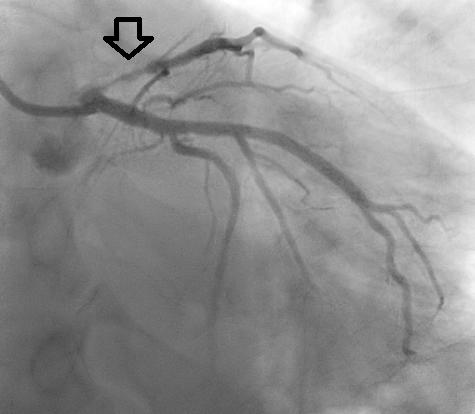
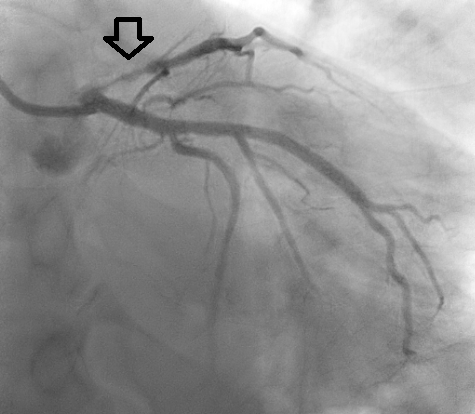
Punctured at right radial approach with terumo method 6FR and diagnostic shot over right system with optitorque 6FR revealed normal right coronary artery. Coronary angiogram showed 80% stenosis in the proximal left anterior descending (LAD) artery with short left main artery. Normal left circumflex artery as well. Not much thrombus seen at the proximal LAD.

Interventional Management
Procedural Step
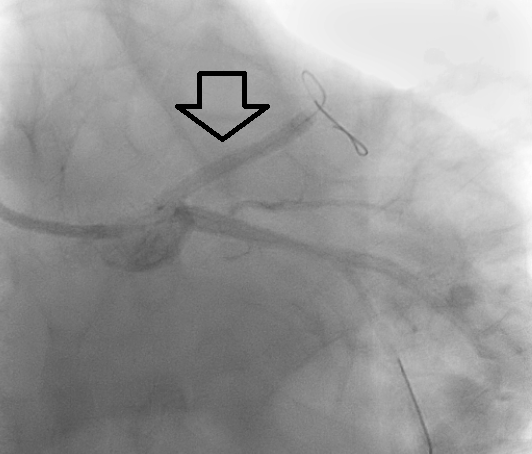
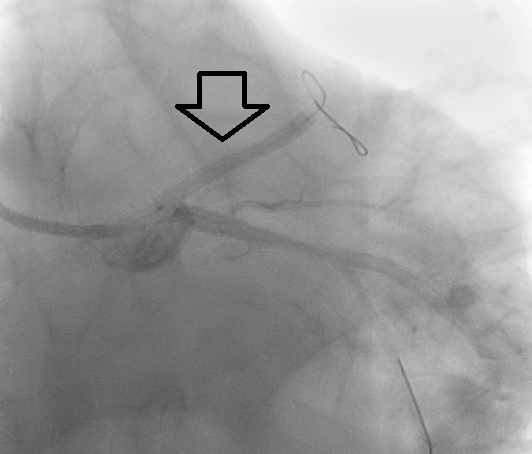
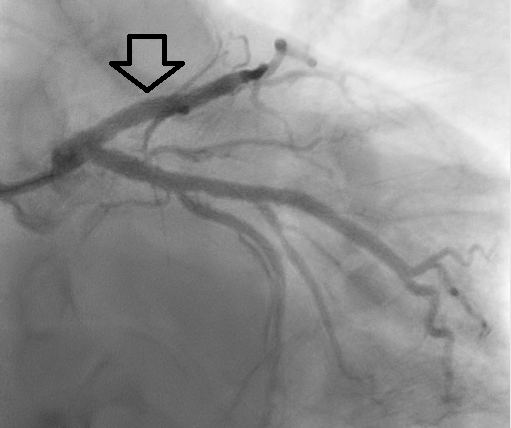
Recognizing the urgency of the situation, the patient was rapidlytransferred to our center for primary percutaneous coronary intervention (PCI).Coronary angiography revealed significant 80% stenosis in the proximal left anteriordescending (LAD) artery. We employed an Extra-Backup (EBU) 3.5 6FR guidecatheter for optimal support and access, meticulously wiring the LAD with aRun-Through Floppy (RTF) guidewire. Stability was further enhanced with a SionBlue guidewire for the left circumflex (LCx) artery.
Case Summary
Post-procedure, the patient experienced an uneventful recovery and was discharged in stable condition, underscoring the critical importance of timely intervention in acute myocardial infarction. This case illustrates the rapid assessment and intervention required in managing acute coronary syndromes, highlighting the effectiveness of PCI in restoring blood flow and preserving myocardial function. Early recognition and swift action can significantly impact patient outcomes, reaffirming the need for vigilant monitoring and rapid response in acute cardiac care.