
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-125
Complex and High-Risk Intervention in Indicated Patients (Chip) - PCI for 2-Vessel CTO and Left Main Trunk Lesion With Severe Calcification in a Polyvascular Disease Patient With Cardiogenic Shock
By Yasunori Inoguchi, Ryo Nishikawa, Yohei Yakuta, Taiji Yoshida, Hidenobu Terai
Presenter
Yasunori Inoguchi
Authors
Yasunori Inoguchi1, Ryo Nishikawa1, Yohei Yakuta1, Taiji Yoshida1, Hidenobu Terai1
Affiliation
Kanazawa Cardiovascular Hospital, Japan1,
View Study Report
TCTAP C-125
Coronary - Complex PCI - Multi-Vessel Disease
Complex and High-Risk Intervention in Indicated Patients (Chip) - PCI for 2-Vessel CTO and Left Main Trunk Lesion With Severe Calcification in a Polyvascular Disease Patient With Cardiogenic Shock
Yasunori Inoguchi1, Ryo Nishikawa1, Yohei Yakuta1, Taiji Yoshida1, Hidenobu Terai1
Kanazawa Cardiovascular Hospital, Japan1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
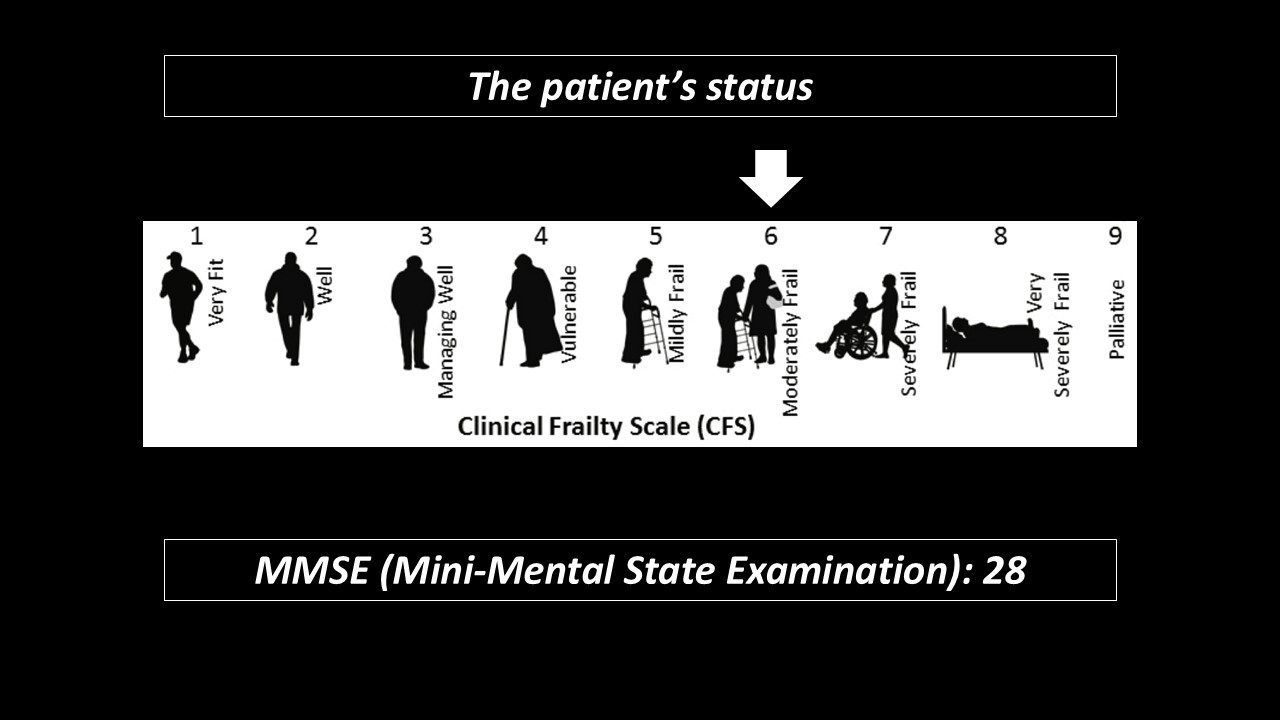
A 83-year-old woman was admitted ourhospital due to acute decompensated heart failure.
Relevant Test Results Prior to Catheterization
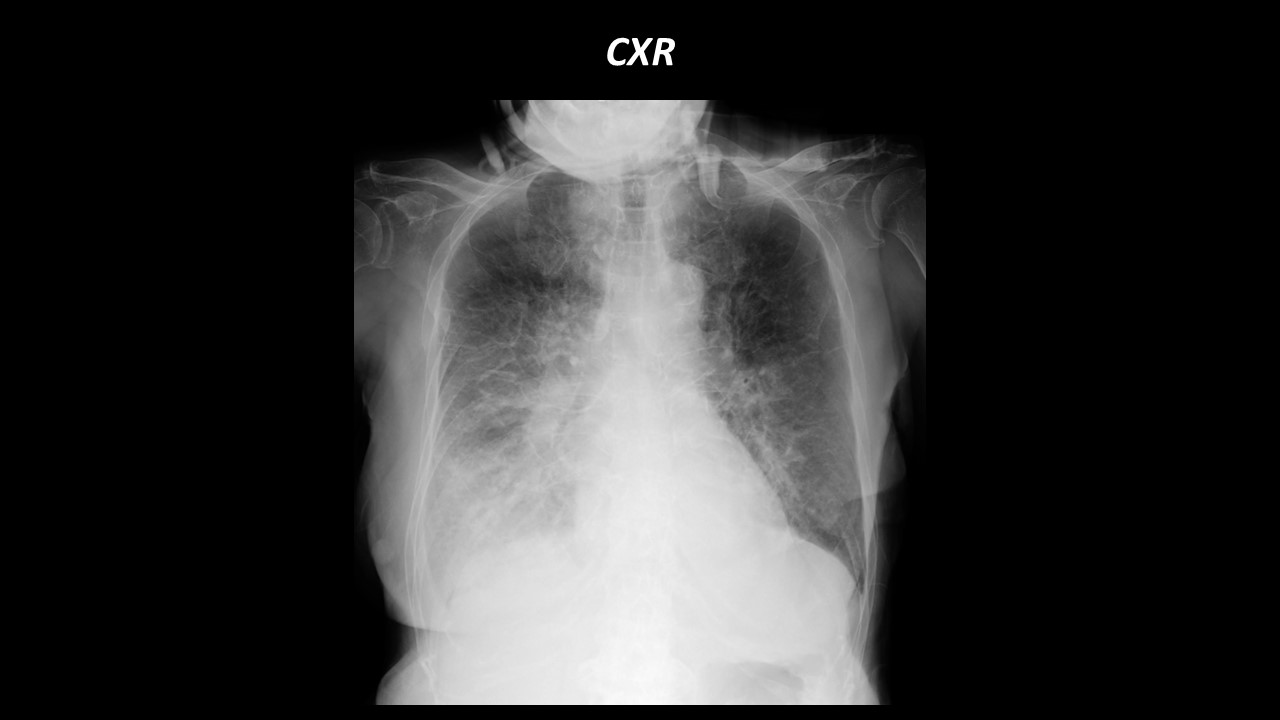
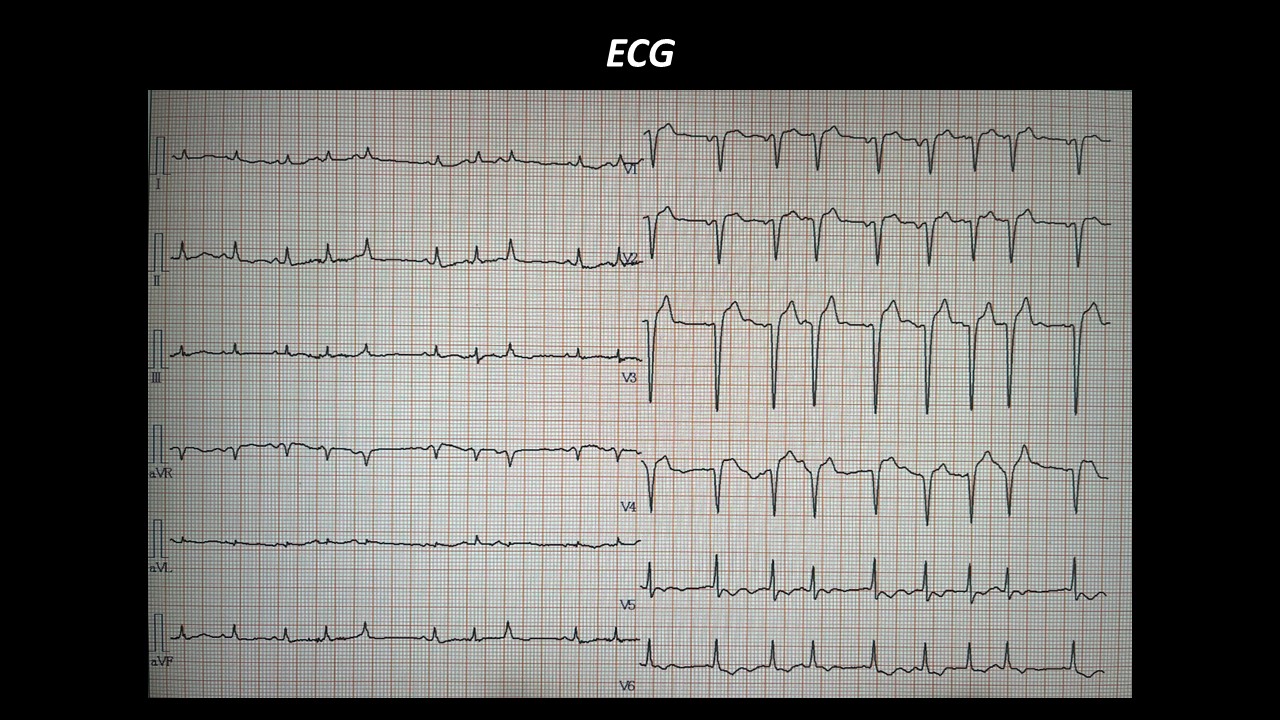
Chest X-ray showed bilateral lung congestion and pleural effusion.Electrocardiography showed poor progressionR in V1 to V4 inductions and ST depression in V5-6 induction.
Relevant Catheterization Findings
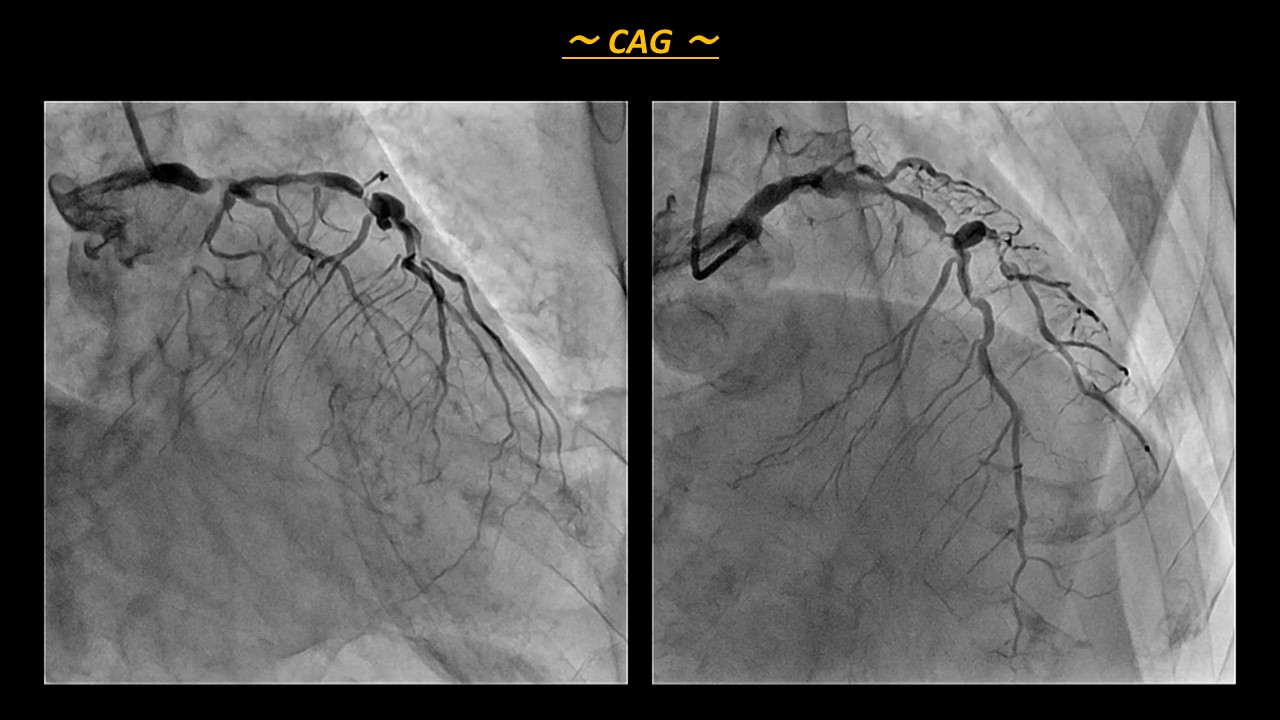
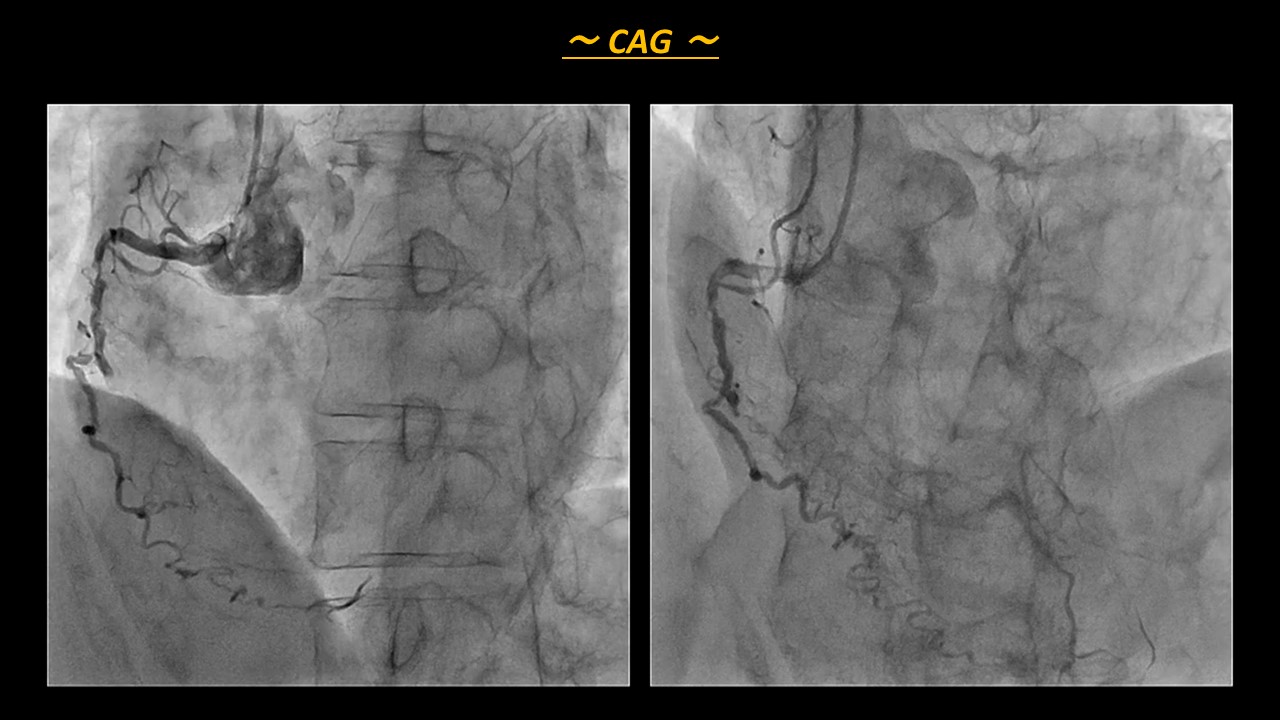
Coronary angiography (CAG) showed triplevessel disease with 2 vessel CTO. There was 99% stenosis with severecalcification in LMT, 99% stenosis in LAD seg7, and CTO in LCx seg11 and RCAseg2.After angiography, we considered how torevascularization for this patient in our heart team including cardiac surgeon.However, surgeon hesitated to CABG because of her severe comorbidities.The day after CAG, she fell into cardiogenic shock, so we had no choice but to performed emergent revascularization.
Interventional Management
Procedural Step
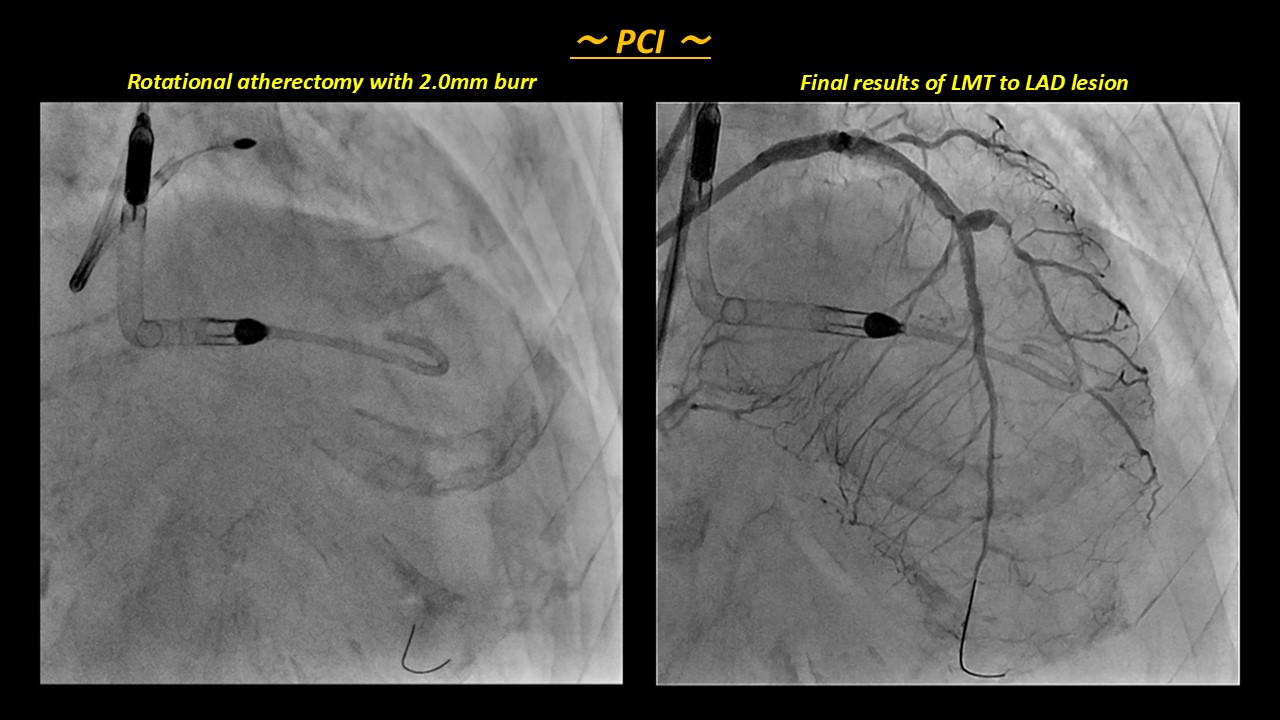
At first, we inserted the Impella CP, and triedto revascularization for LMT and LAD lesion.
Case Summary
We finally could success the one stagerevascularization both LMT to LAD lesion and RCA CTO supported by Impella CP.