
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-146
Inflated Balloon Entrapment With Recurrent VT During LMCA Angioplasty in Acute Myocardial Infarction
By Susanta Pradhan
Presenter
Dr Susanta Pradhan
Authors
Susanta Pradhan1
Affiliation
Utkal Hospital Bhubaneswar, India1,
View Study Report
TCTAP C-146
Coronary - Complication Management
Inflated Balloon Entrapment With Recurrent VT During LMCA Angioplasty in Acute Myocardial Infarction
Susanta Pradhan1
Utkal Hospital Bhubaneswar, India1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A 67 year Male presented with severe chest pain of 8 hr duration. He was diagnosed as Acute anterior wall MI and received loading dose of Dual antiplatelets and Atorvastatin. At presentation his blood pressure was 106/70 mm of Hg and Heart rate of 107/min. Patient was restless and Oxygen saturation was 90% .Patient was managed with NIV ventilation in Emergency. His coronary artery disease risk factors were Diabetes & Smoking.
Relevant Test Results Prior to Catheterization
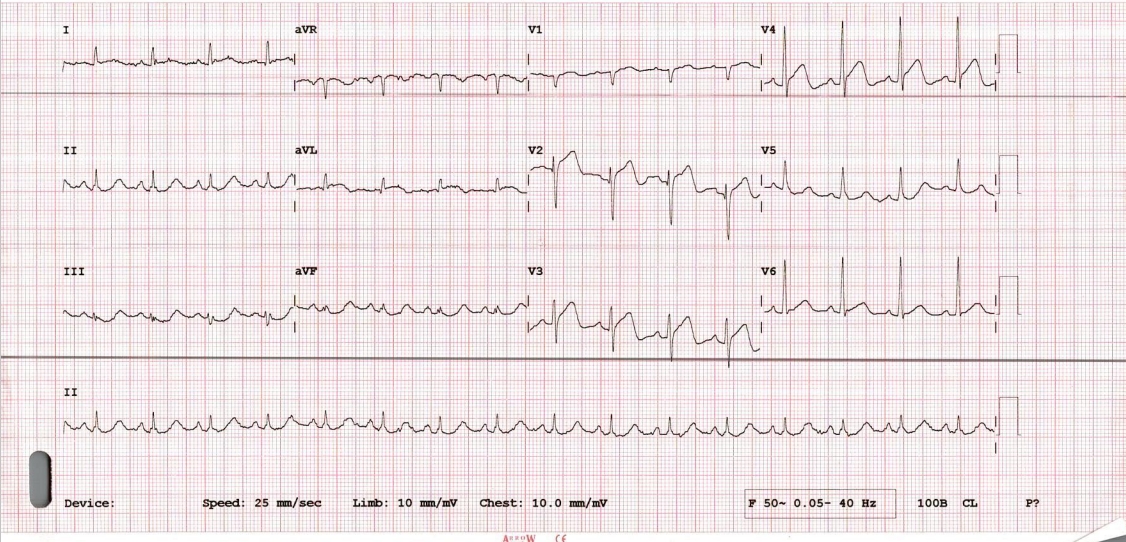
His baseline ECG showed ST elevation in V1-V4 . Echocardiography revealed Hypokinesia of anterior wall and LV ejection fraction of 40%.His initial blood sugar was 352 mg/dl ,serum creatinine of 1.45 mg/dl and Troponin I was 8096 ng/L . Patient was immediately taken for primary angioplasty.
Relevant Catheterization Findings
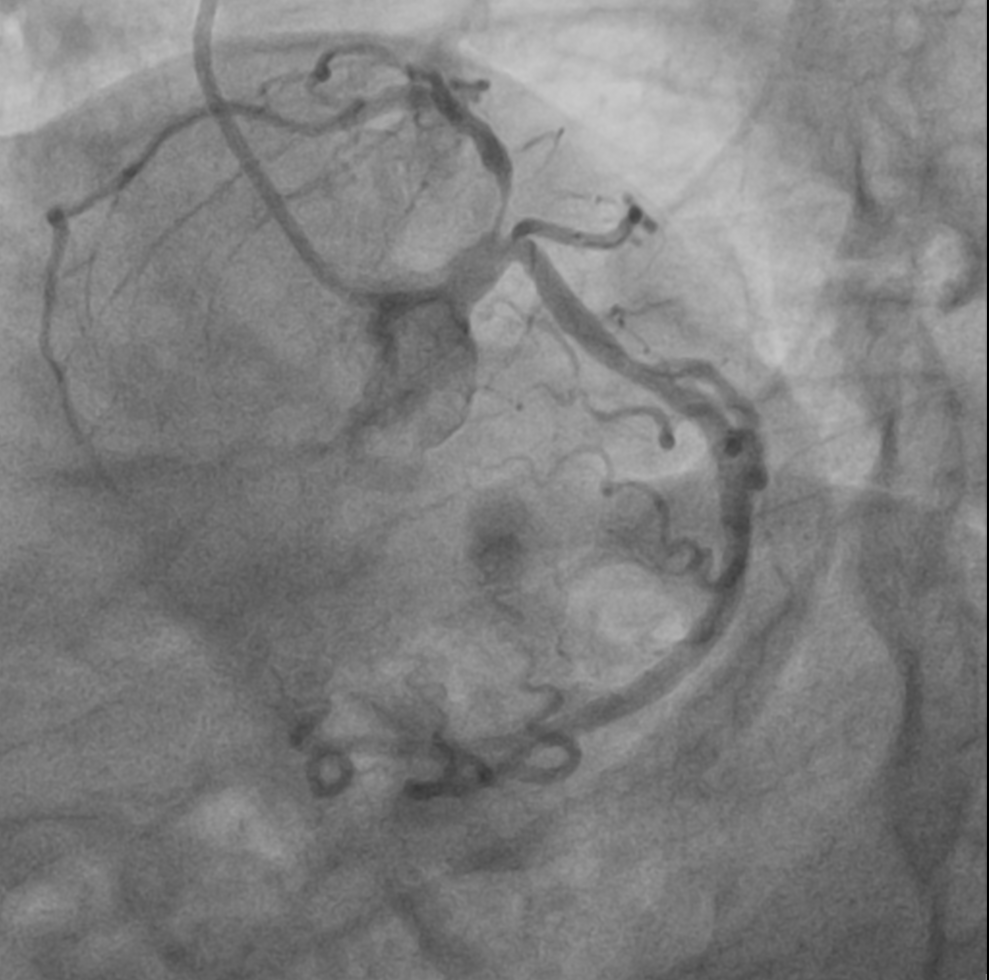
Baseline Coronary Angiography- Angiography was done through right radial artery approach.1. Left coronary angiography : LMCA- distal minor disease, LAD- ostio-proximal 95% long segment disease, LCx-Dominant vessel with minor disease at OM1 ostium.2.Right coronary angiography : Non-dominant vessel.


Interventional Management
Procedural Step
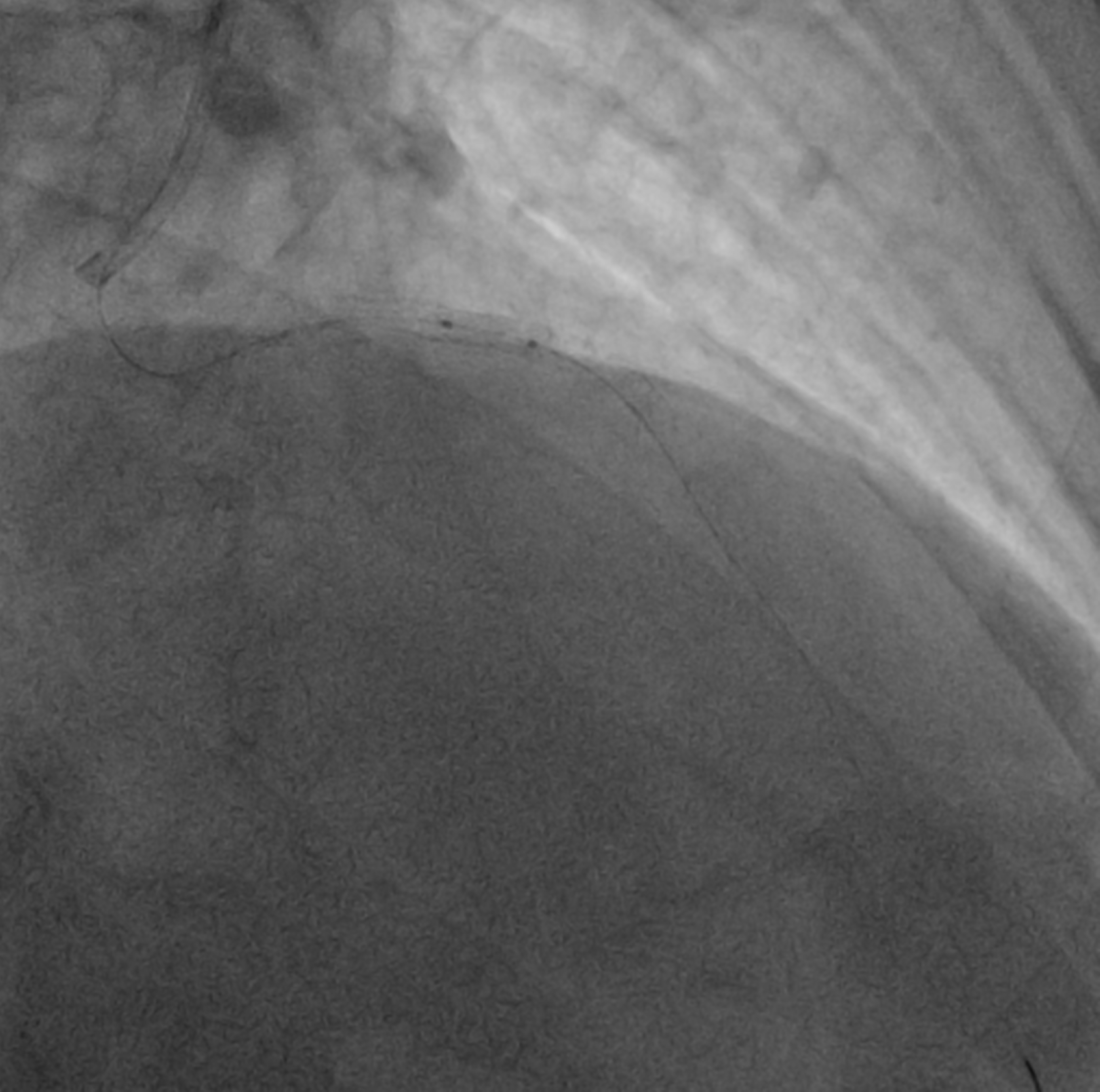
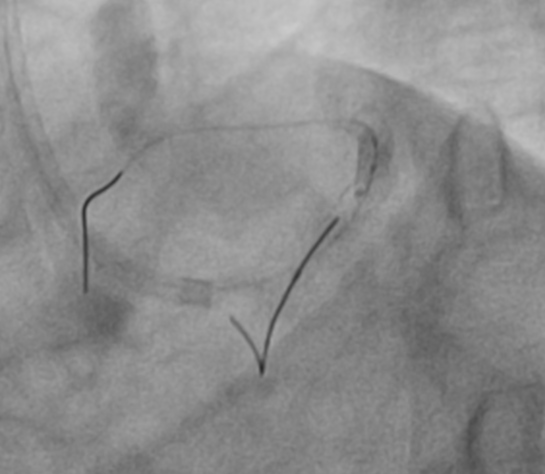
The LMCA was engaged with 7F JL 3.5 guiding catheter through right radial artery approach. The LAD lesion was crossed with one 0.014 wire and another 0.014 wire was placed in LCX. Than ostial to mid LAD lesion was sequentially predilated with 2.5x15 mm balloon, 3.0x10 mm Wolverine cutting balloon and 3.0x20 mm balloon after IVUS evaluation. After checking a 3.5x40 mm DES was positioned from LMCA to LAD. While positioning the stent patient developed VT, so immediately DC-cardioversion and chest compression was given. During this guide catheter was automatically disengaged and everything came out of coronaries. Again after careful guide catheter engagement the DES of 3.5x38 mm Ultimaster nagomi was deployed from LMCA to LAD. Than POT was done to LMCA stent with 5.0x8 mm NC balloon and LAD with 3.5x20 mm NC balloon. As LCX was dominant vessel, so kissing was done to distal LMCA with 3.5x20 mm NC balloon in LAD and 2.5x12 mm balloon in LCX.As IVUS revealed under expanded LAD stent so post dilatation done with 3.5x8 mm NC balloon at 16 atm pressure, than balloon failed to deflate. Gentle traction was applied to inflated balloon keeping negative suction ,but failed. Patient again developed VT, so DC-cardioversion was given. Trying to rupture the balloon with reverse end of BMW wire through OTW balloon, not worked. Than we used saline instead of dye with two indefaltors in three ways and negative pressure was given and that worked. Than procedure was completed with another balloon.

Case Summary
Deflation failure of balloon during coronary angioplasty is a extremely rare complication. Cath lab should be prepared with managing this life threatening complication by few bail-out techniques available. However, if the patient is unstable, it is required urgently to restore the blood flow in the blocked coronary arteries. In our case, we successfully managed this complication by deflating the balloon using normal saline instead of contrast with 2 indeflator devices connected with three way.