
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-094
Advancing Cardiovascular Care: ECMO Support and CHIP-PCI for Two-Vessel CTOs
By Shu-Kai Hsueh, Chun-Ting Shih, Chiung-Jen Wu
Presenter
Chun-Ting Shih
Authors
Shu-Kai Hsueh1, Chun-Ting Shih1, Chiung-Jen Wu1
Affiliation
Kaohsiung Chang Gung Memorial Hospital, Taiwan1,
View Study Report
TCTAP C-094
Coronary - Complex PCI - CTO
Advancing Cardiovascular Care: ECMO Support and CHIP-PCI for Two-Vessel CTOs
Shu-Kai Hsueh1, Chun-Ting Shih1, Chiung-Jen Wu1
Kaohsiung Chang Gung Memorial Hospital, Taiwan1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
This 39-year-old man, a heavy smoker with a history of coronary artery disease, type 2 diabetes, dyslipidemia, and hypertension, presented to our hospital with shortness of breath and chest pain lasting several days.
Relevant Test Results Prior to Catheterization
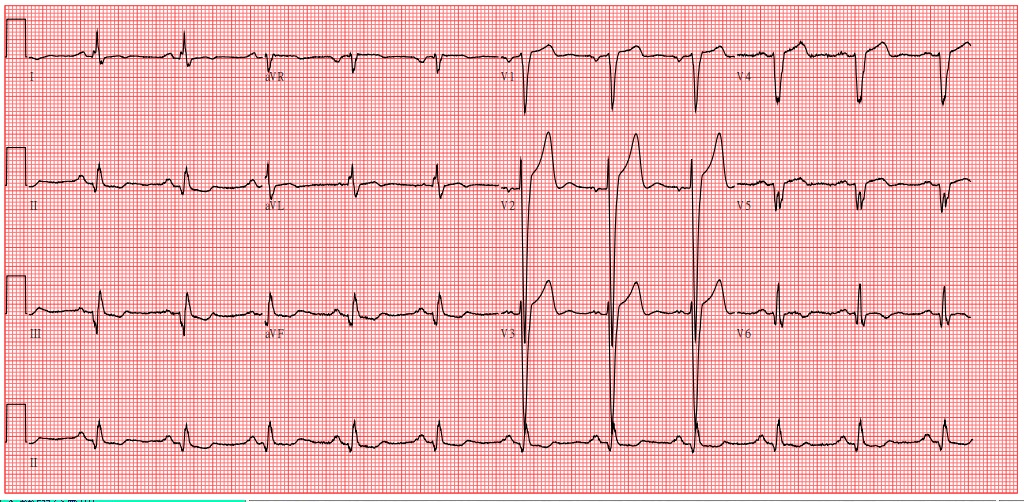
This 39-year-old man presented to our hospital with shortness of breath and chest pain lasting several days. A diagnosis of congestive heart failure with NYHA II classification may account for his clinical condition. Echocardiography revealed a dilated left atrium and left ventricle, as well as diffuse hypokinesis, particularly in the inferolateral wall, with a poor left ventricular ejection fraction of 30%.
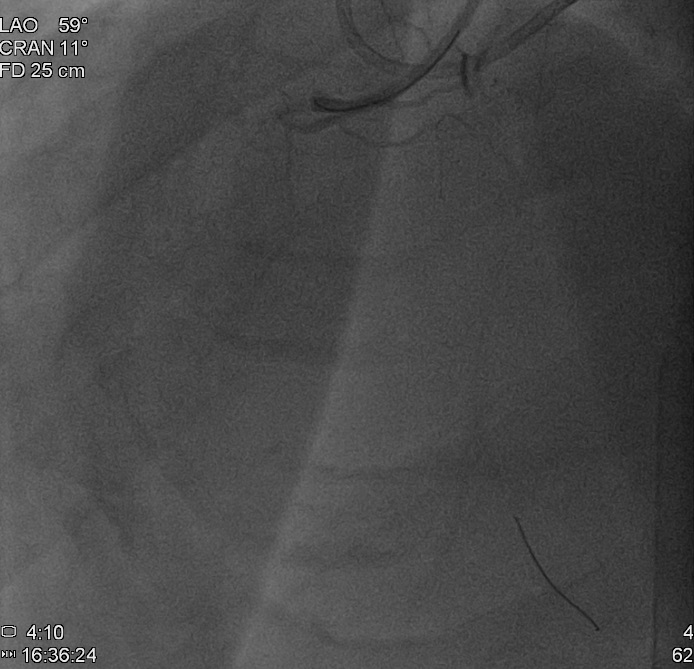
Relevant Catheterization Findings
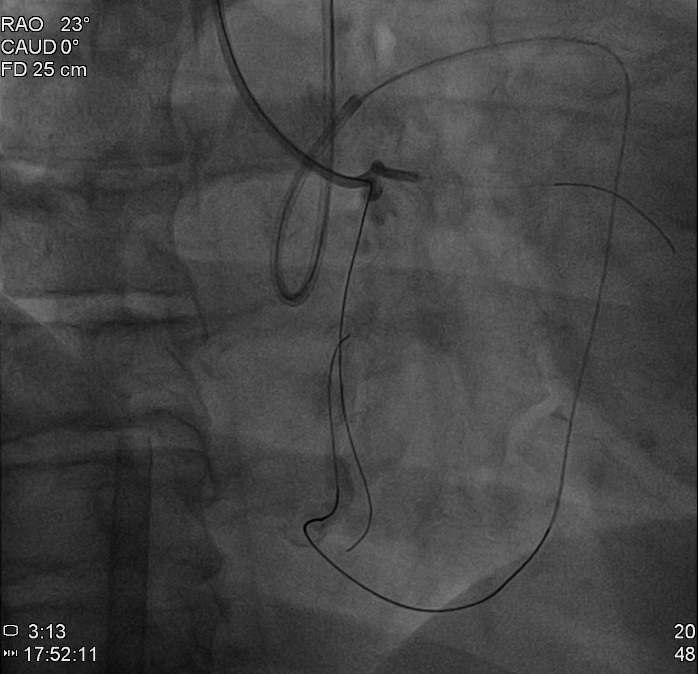
Although no in-stent restenosis was detected in the proximal portion of the left anterior descending artery (LAD), chronic total occlusions were noted in the proximal left circumflex artery (LCx) and proximal right coronary artery (RCA).
Interventional Management
Procedural Step
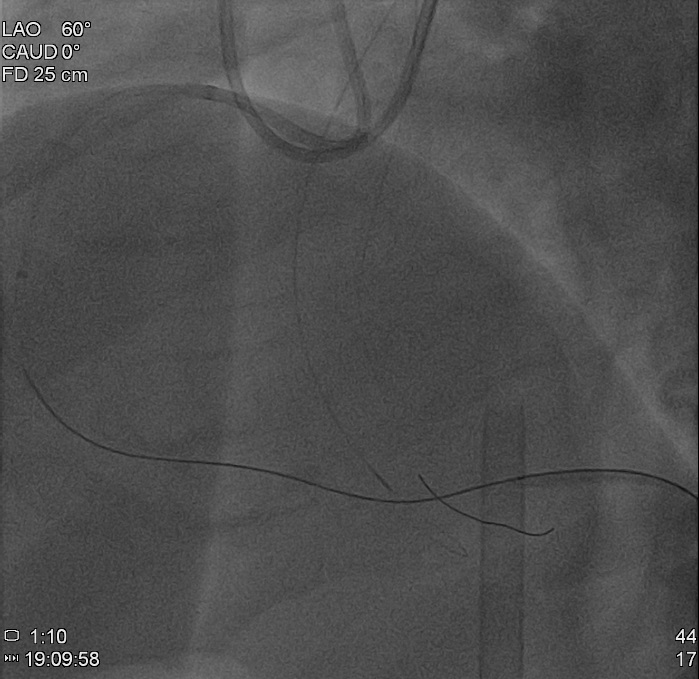
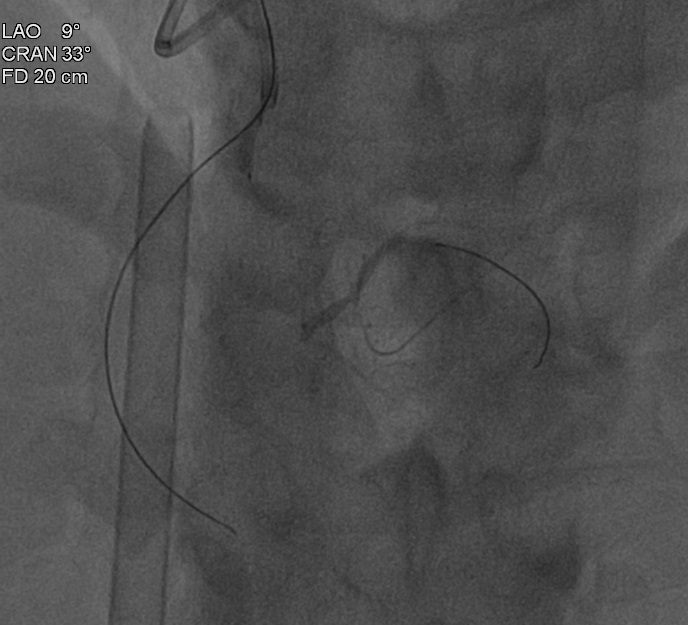
A 0.014-inch Runthrough wire was advanced to the conus branch and an angle balloon (2.0 × 15 mm) was inflated to a pressure of 12 bar. Antegrade wiring was performed using a Gia 2nd wire, which was escalated to a Gia 3rd wire with support from a 130 cm Finecross microcatheter. Simultaneously, a retrograde approach from the left anterior descending artery (LAD) was employed, wiring with a Sion wire to the septal branch using a Caravel microcatheter. The wire was then changed to a Suoh wire to access the PDA and PL branch bifurcation, successfully advancing to the PDA branch. A Gladius wire was then used to wire the mid RCA retrogradely with the knuckle wire technique. The Conquest Pro 12 was employed for antegrade wiring, kissing the retrograde wire. Reverse CART was performed using Terumo Ryurei 1.0 × 5 mm and 2.0 × 15 mm balloons sequentially, and the Fielder FC was successfully advanced to the antegrade guiding catheter. The wire was then switched to an RG 3 wire with a Guidezilla extension catheter.
Case Summary
In conclusion, the proactive use of mechanical circulatory support (MCS) prior to CHIP-PCI has the potential to minimize local femoral access complications, leading to improved patient outcomes compared to bail-out MCS strategies. Furthermore, ensuring an adequate dosage of heparin and regularly monitoring activated clotting time (ACT) at 30-minute intervals significantly reduces the risk of peri-procedural in-stent thrombus formation. Additionally, employing bail-out knuckle wires for challenging courses in the mid-right coronary artery (RCA) can facilitate reverse CART (R-CART).