
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-107
A Case of In-Stent Restenosis Successfully Treated With Rotational Atherectomy
By Rie Aoyama, Shinichi Okino, Shigeru Fukuzawa
Presenter
Rie Aoyama
Authors
Rie Aoyama1, Shinichi Okino1, Shigeru Fukuzawa1
Affiliation
Funabashi Municipal Medical Center, Japan1,
View Study Report
TCTAP C-107
Coronary - Complex PCI - In-Stent Restenosis
A Case of In-Stent Restenosis Successfully Treated With Rotational Atherectomy
Rie Aoyama1, Shinichi Okino1, Shigeru Fukuzawa1
Funabashi Municipal Medical Center, Japan1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
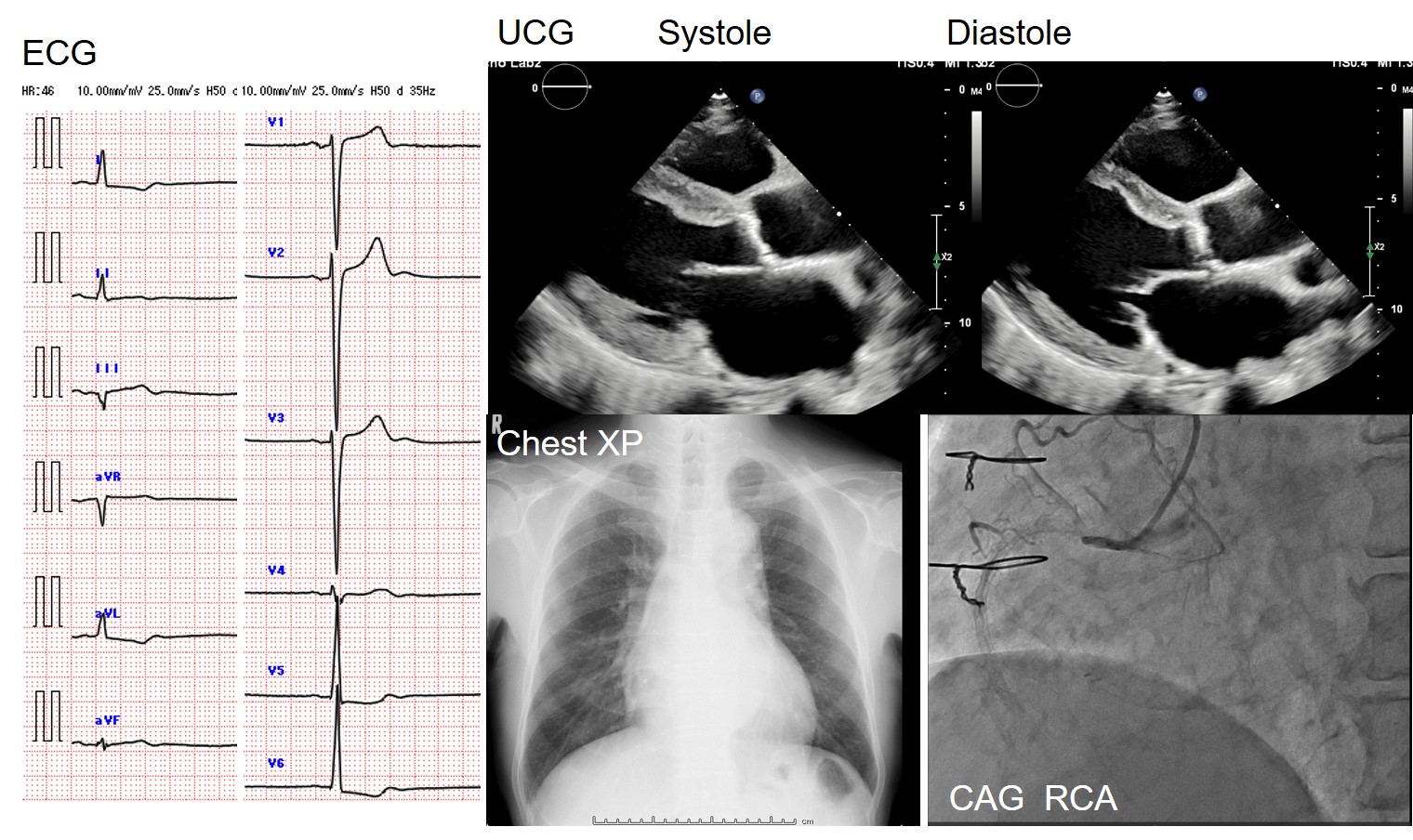
Thepatient is an 81-year-old male with type 2 diabetes mellitus, hypertension, andend-stage renal disease on dialysis. He has ischemic cardiomyopathy with EF 30%and a history of CABG (LITA-LAD, RITA-RCA-LCX) 20 years ago. A Bare metal stent(3.0/24mm) was implanted 15 years ago for native RCA due to RITA obstruction. Inthis time, he was hospitalized for worsening heart failure, and after the heartfailure improved, CAG revealed that the native RCA was completely occluded fromthe orifice.
Relevant Test Results Prior to Catheterization
Relevant Catheterization Findings
Interventional Management
Procedural Step
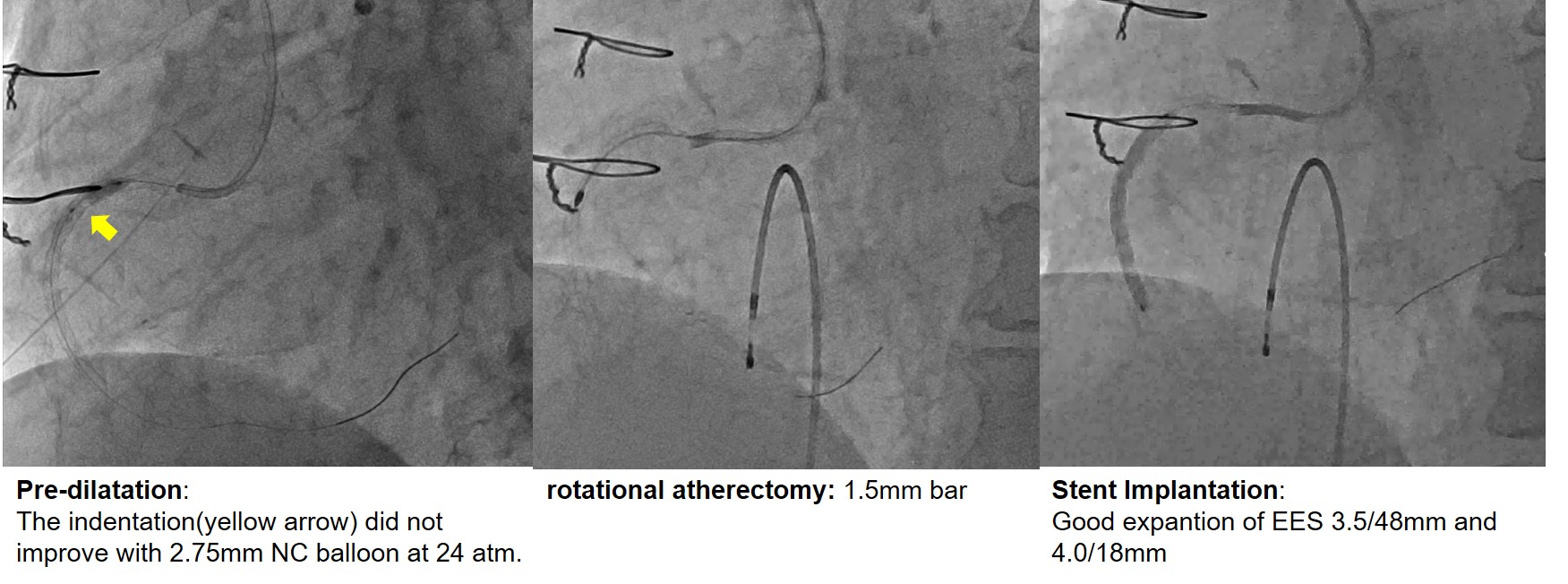
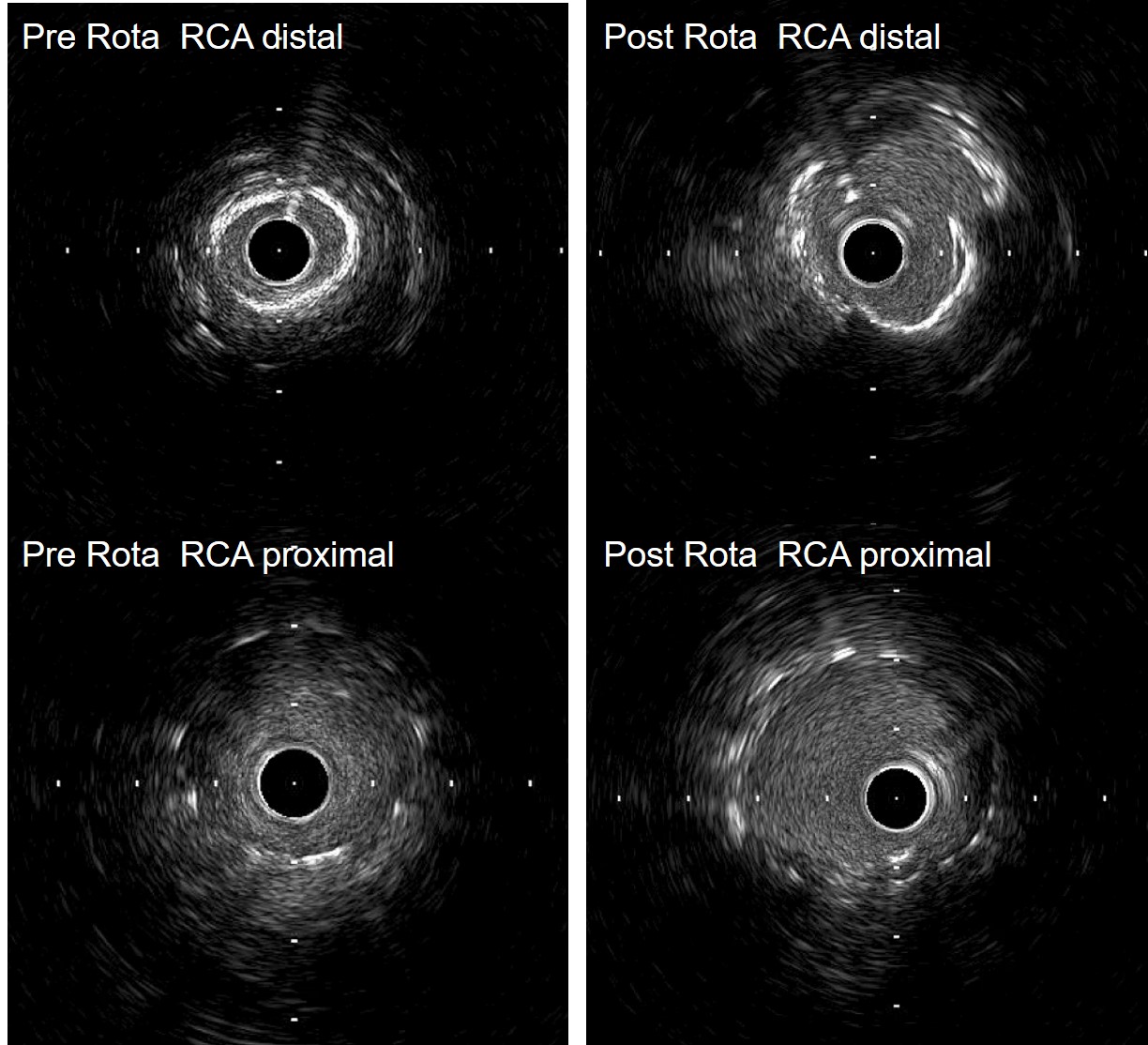
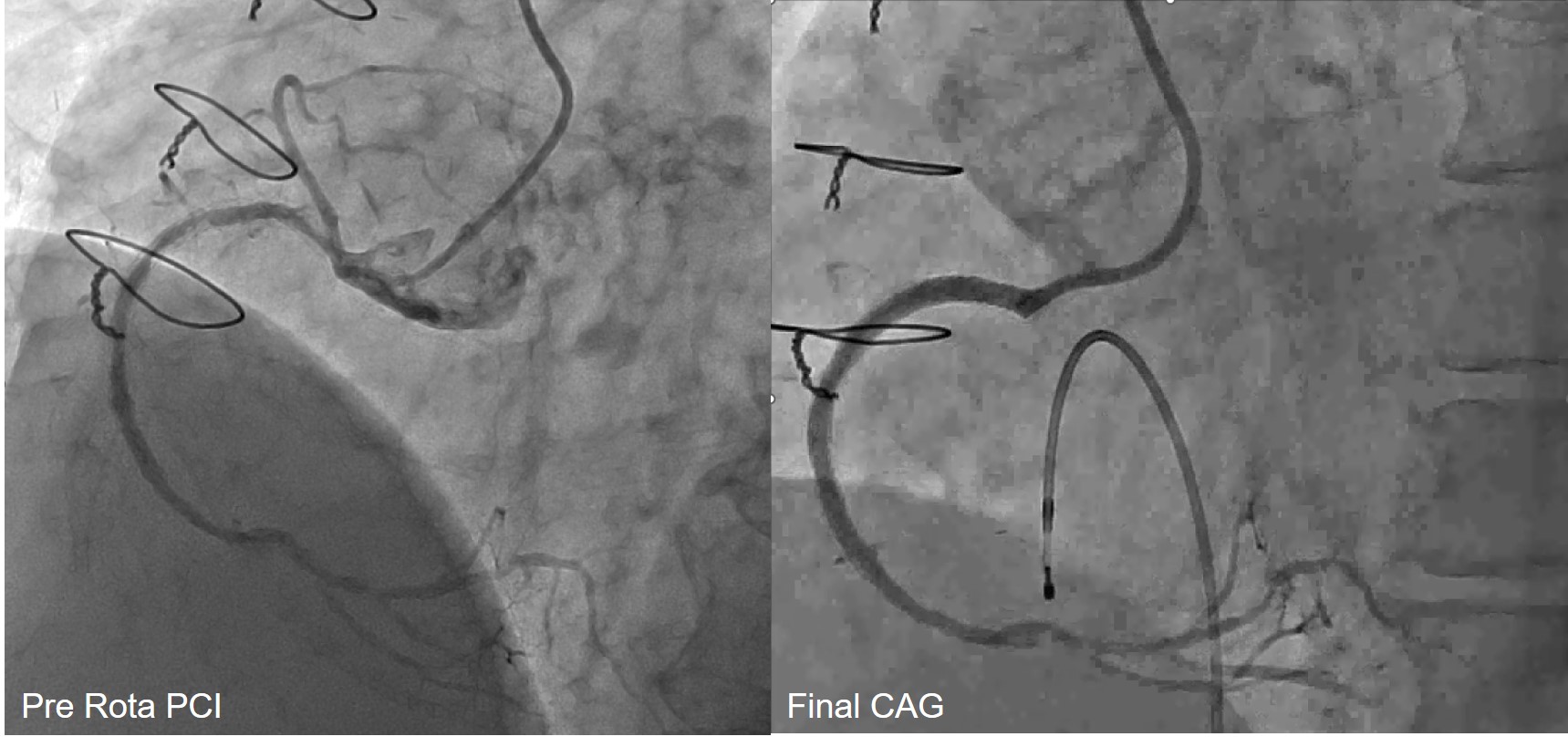
He had a chronic dissection of the abdominal aorta and a 6Fr guide catheter JR4.0 was placed in the RCA via the right brachial artery. Sequential balloon dilatation was performed with 2.0mm and 2.75mm cutting balloons, but the restenosis lesion in the stent was highly calcified and indentations did not improve even with a 2.75mm NC balloon at 24 atm. Debulking was deemed necessary and PCI was performed on another day. A 7Fr guide catheter AL0.75 was placed in the RCA via the right brachial artery. 14 times of rotational atherectomy at 210,000 rpm with a 1.5mm bar were performed in ISR lesions. A 3.0 mm scoring balloon was used for additional dilation to 22atm. IVUS showed that the calcification had faded, and the small fractures of the calcification were made. The EES 3.5/48mm and 4.0/18mm were overlapped and implanted. Good dilation and crimping were confirmed by IVUS, and the procedure was completed.
Case Summary
Highly calcified coronary lesions and restenosis are common and poor stent dilatation can lead to restenosis. Plaque modification prior to stent implantation is particularly important in dialysis patients. In this case, when neointimal calcification due to in-stent restenosis was evident, gentle rotational atherectomy with high-speed rotation was effective and the stent was successfully expanded and implanted.