
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-092
A Twist, Turn and Tear
By Khai Chih Teh
Presenter
Khai Chih Teh
Authors
Khai Chih Teh1
Affiliation
Institut Jantung Negara, Malaysia1,
View Study Report
TCTAP C-092
Coronary - Complex PCI - CTO
A Twist, Turn and Tear
Khai Chih Teh1
Institut Jantung Negara, Malaysia1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
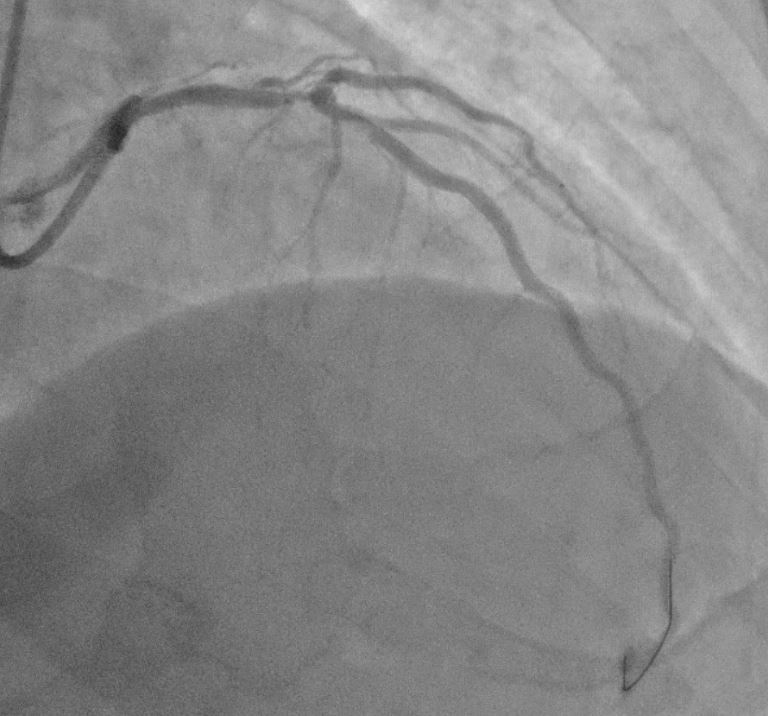
63 year old gentleman with background history of smoking and hyperlipidemia, treated at a private hospital for recurrent angina. Coronary angiogram showed 2 vessel disease - severe proximal LAD disease with CTO of proximal RCA. PCI to LAD was performed without any complications and he was referred to us for PCI of the CTO RCA. Unfortunately no cine images of the CTO RCA were available for review.Physical examination was uneventful with BP 135/87, HR 80 bpm regular, clear lungs with no murmurs.

Relevant Test Results Prior to Catheterization
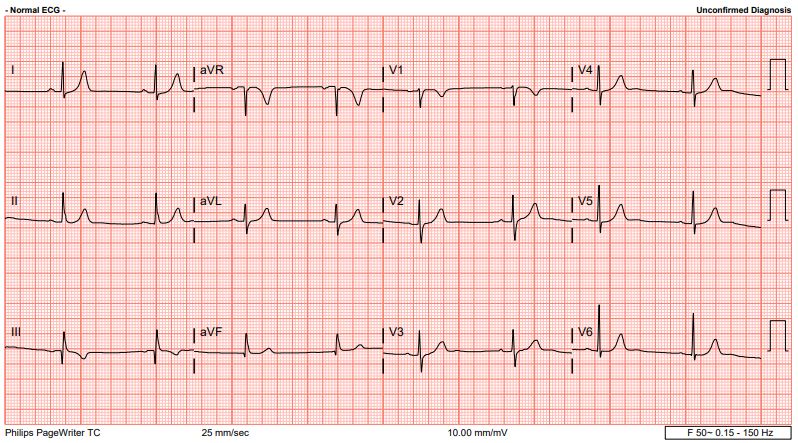
ECG: sinus rhythm, no acute ischemic changesChest X ray: clear lung fields, normal heart sizeECHO: LVEF 62%, normal LV size with septal LVH 1.3cm; TAPSE 2.0cm. Normal valves

Relevant Catheterization Findings
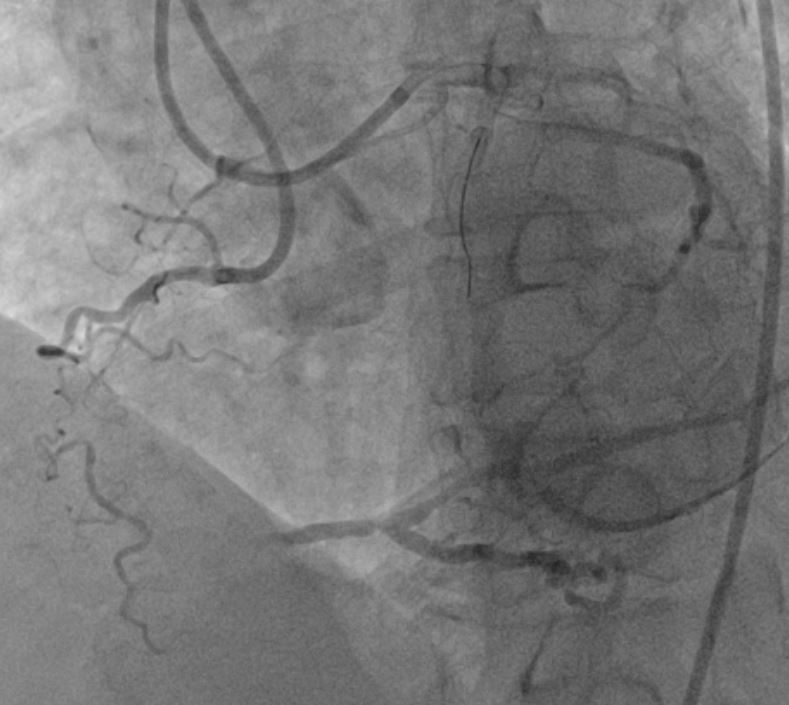
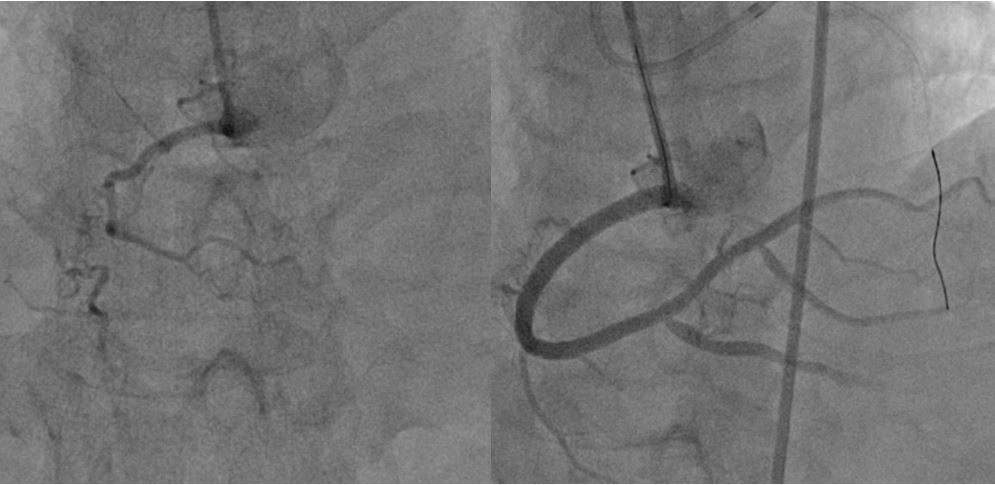
Left main: normalLeft Circumflex artery: normal, non dominantLeft Anterior Descending Artery: proximal LAD stent patent; epicardial retrograde filling to distal RCARight Coronary Artery: 2tandem CTOs at proximal and mid RCA, JCTO score 2 (calcification, lesion length > 20mm). Presence of bridging collaterals from atrial branch of RCA to mid RCA


Interventional Management
Procedural Step
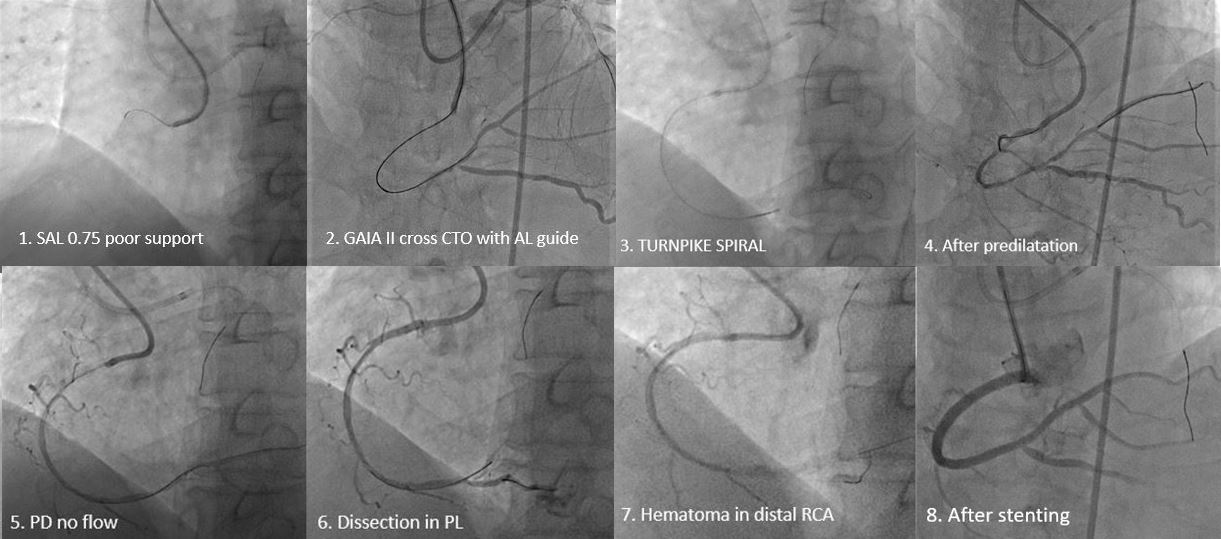
Attempt to approach proximal cap with FIELDER XT in CARAVEL microcatheter using SAL 0.75 guide was unsuccessful due to poor guide position. Changed to JR 3.5 guide, crossed first CTO up to mid RCA with FIELDER XT followed by GAIA II, however loss system due to poor guide support.
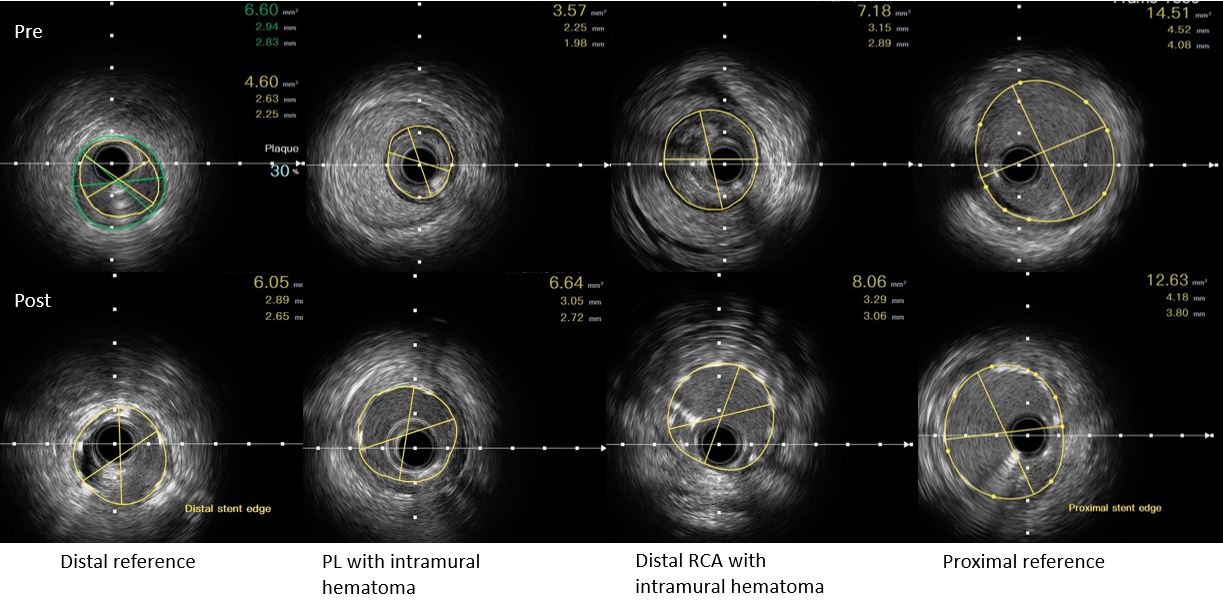
Case Summary
This case illustrates the importance of guide support while performing antegrade wire escalation for CTO PCI. In balloon uncrossable lesions where atherectomy is not an option in view of high likelihood of presence of significant dissections, a microcatheter with high flexibility, trackability and torque transmission is used to create sufficient luminal gain to allow passage of further equipment for successful lesion preparation.Intimal dissection leading to formation of intramural hematoma can lead to acute vessel occlusion. immediate stent deployment to seal the dissection flap, preventing further accumulation of hematoma and restoring vessel patency is necessary.