
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-071
A Challenging Case Report: Recanalization of RCA With Anomalous Origin From the Left Sinus
By Jian-Kuan Yeh, Cheng-Yu Ko
Presenter
Jian-Kuan Yeh
Authors
Jian-Kuan Yeh1, Cheng-Yu Ko1
Affiliation
National Cheng Kung University Hospital, Taiwan1,
View Study Report
TCTAP C-071
Coronary - Complex PCI - CTO
A Challenging Case Report: Recanalization of RCA With Anomalous Origin From the Left Sinus
Jian-Kuan Yeh1, Cheng-Yu Ko1
National Cheng Kung University Hospital, Taiwan1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
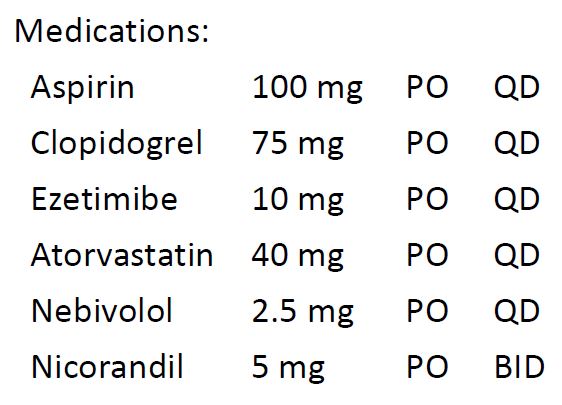
This is a 45-year-old man with hypertension and dyslipidemia on medical therapy. He smoked 2 packs of cigarettes per day for 30 years. The patient was at his usual status until April of 2024 when progressive dyspnea on exertion and chest tightness occurred, resulting in decreased exercise tolerance. Physical exam showed clear breath sounds bilaterally and regular heart rate and rhythm without audible murmurs.
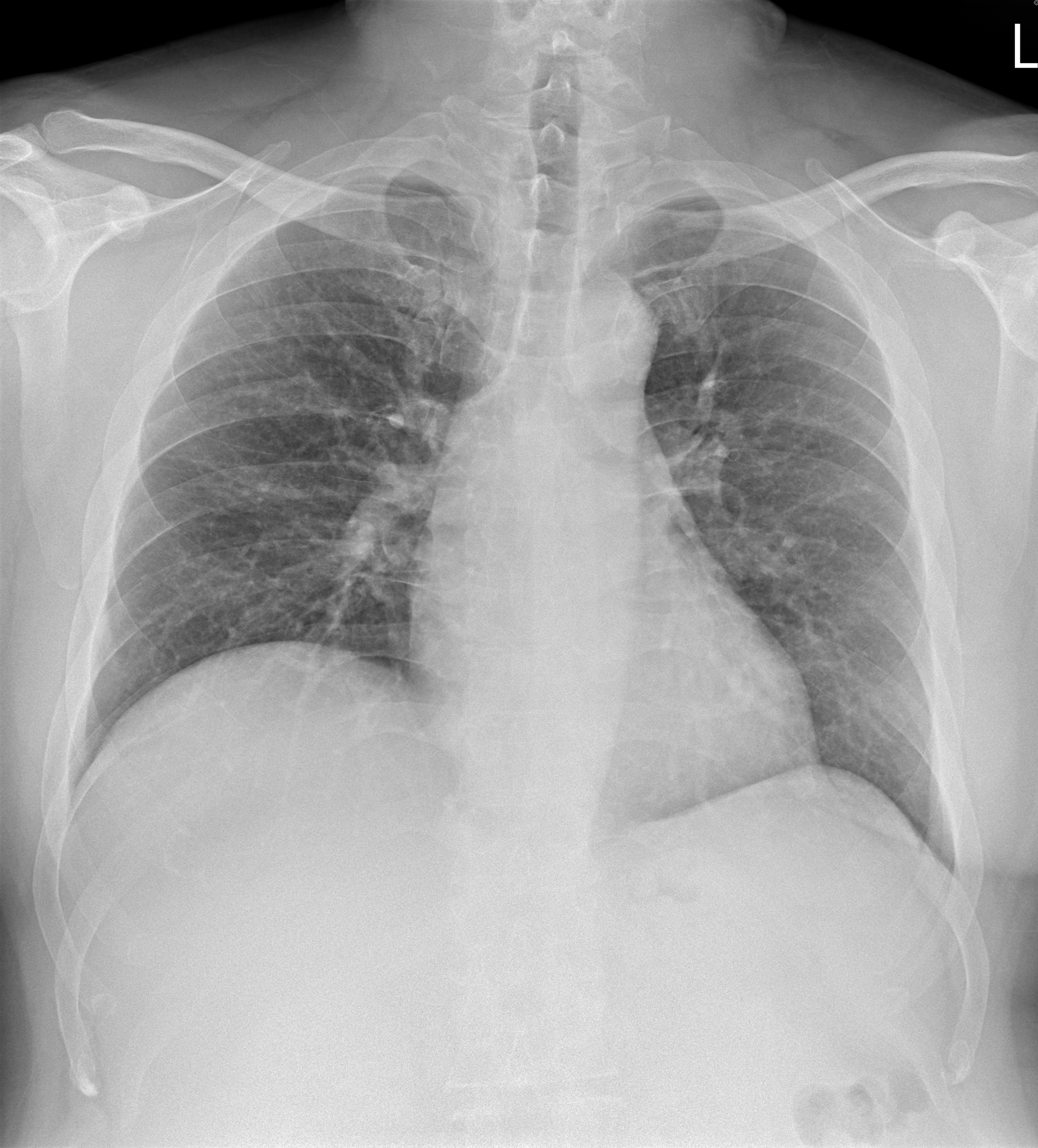
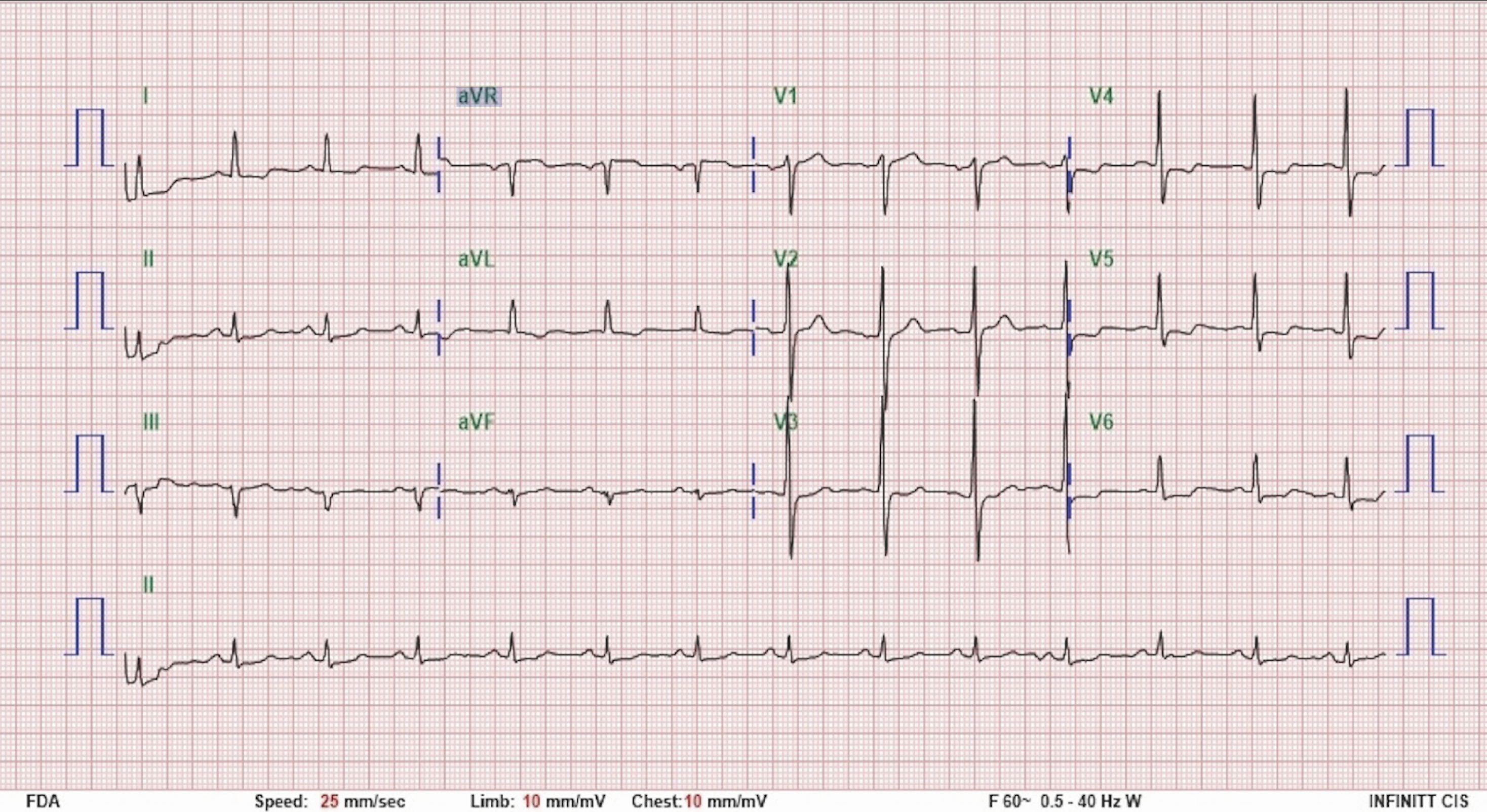
Relevant Test Results Prior to Catheterization
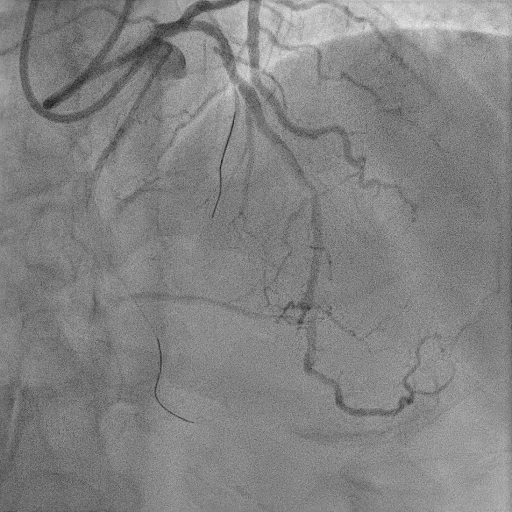
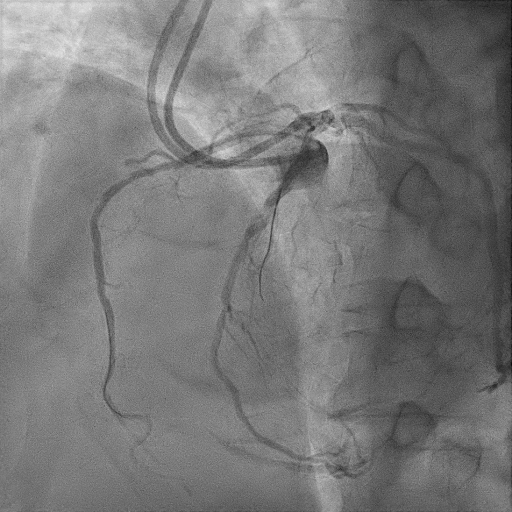
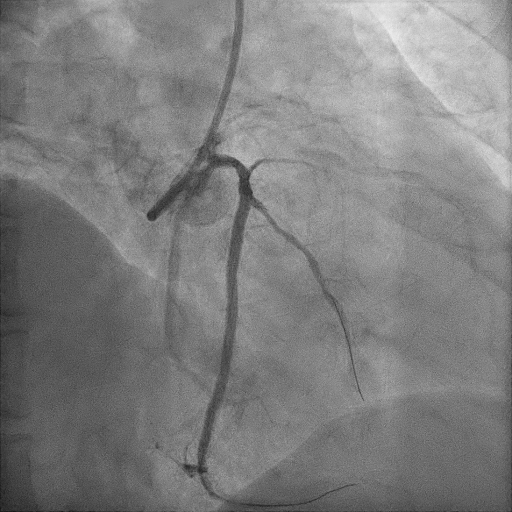
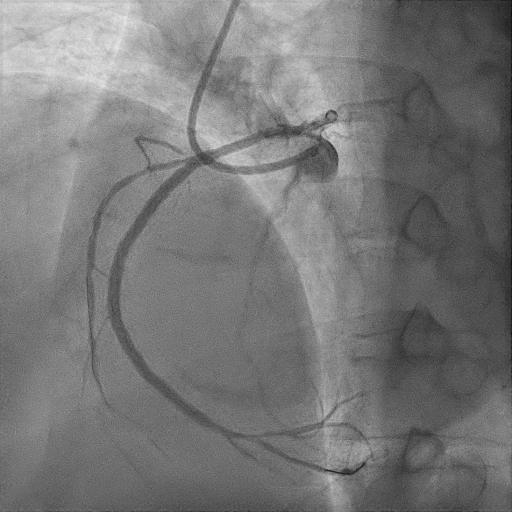
The electrocardiogram showed sinus rhythm. The echocardiography showed adequate global LV systolic function without regional wall motion abnormalities. He underwent a treadmill exercise test, which was positive for ischemia. The initial coronary angiogram showed absence of RCA from the RCC, and due to collaterals from the LAD, total occlusion of the RCA since the ostium was suspected. Due to proximal cap ambiguity, coronary CTA was arranged, and showed that the RCA originated from the LCC.
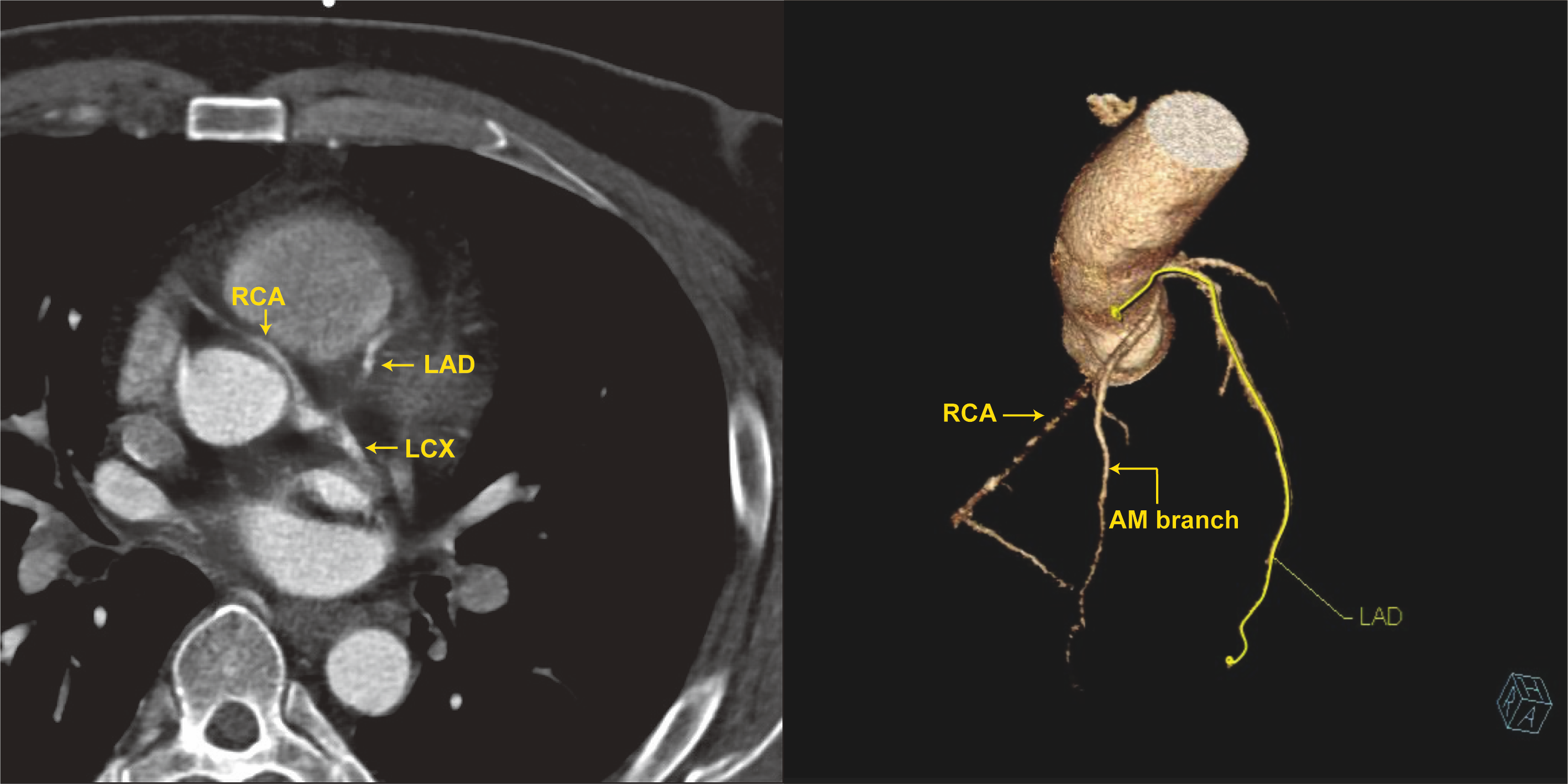
Relevant Catheterization Findings
Left main coronary artery: atherosclerosis without significant stenosisLAD: atherosclerosis, mLAD 50% stenosisLCX: atherosclerosis, post stenting without significant in-stent restenosisRCA: anomalous origin from the left coronary cusp, total occlusion since pRCACollaterals: AM branch of RCA to dRCA; septal branches of LAD to dRCA
Interventional Management
Procedural Step
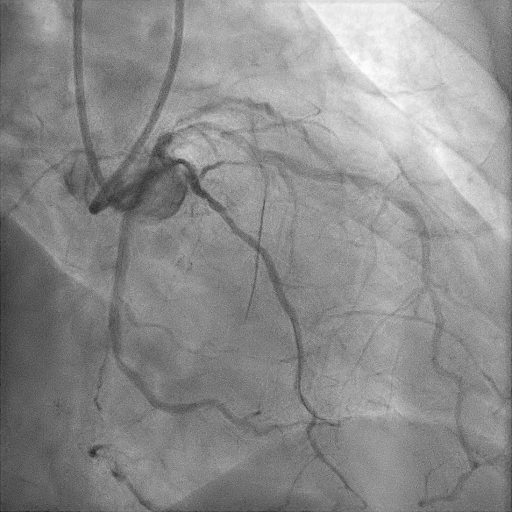
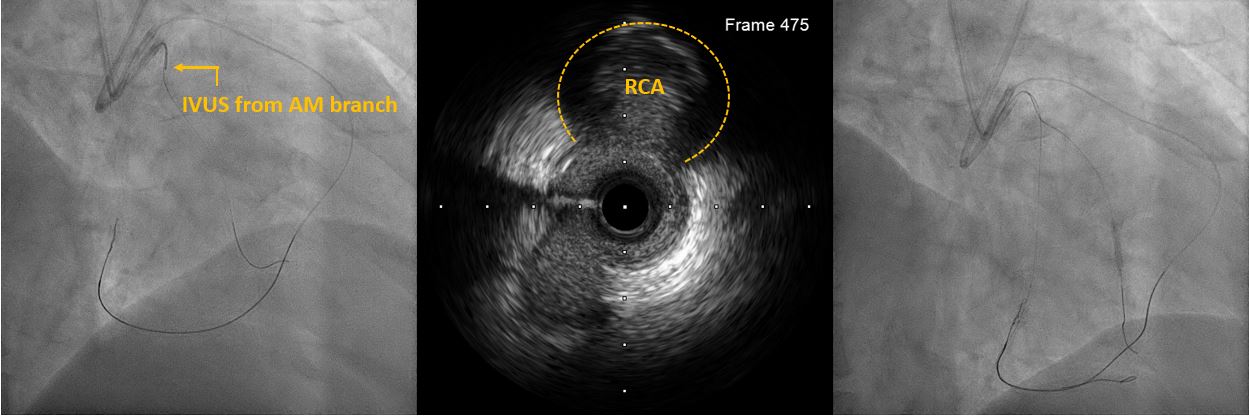
1. An EBU 3.75 SH 7 Fr. guiding catheter to engage LM orifice, an EBU 3.5 SH 7 Fr. guiding catheter with the 6 Fr. guide extension catheter to engage RCA orifice.2. The XT-A wire in the Caravel microcatheter to try antegrade wiring, but difficult to advance due to proximal cap ambiguity.3. Switched to retrograde strategy due to intervention collaterals present (CC2 septal branches from LAD to RCA). 4. The Sion wire in the Caravel microcatheter successfully reached the dRCA via septal collaterals.5. Retrograde wire escalation from Fielder XTA, Gaia 2nd, to Gaia 3rd wires, reaching mRCA. Gaia 3rd left at mRCA as landmark.6. Switched back to antegrade approach. IVUS run over RCA-AM to identify proximal CTO stump.7. Antegrade wire escalation for RCA, using Fielder XTA and then Gaia 2nd wires, along with Sasuke dual lumen microcatheter and anchoring balloon technique (2.5mm semi-compliant balloon) over AM branch. Antegrade wire entered m-dRCA successfully.8. Two DESs (3.0x48mm) were deployed over p-dRCA after adequate lesion preparation.9. A DCB (3.5x2mm) inflated at the ostial RCA, and another DCB (2.5x30mm) inflated at the dRCA.
Case Summary
1. Proximal cap ambiguity of CTO could be resolved by either coronary CT angiography, intravascular ultrasound, retrograde crossing, or a combination of the above-mentioned methods. 2. Guide-extension catheters and side branch balloon-anchoring technique may be useful in increasing the support during CTO PCI.3. Drug-coated balloons may be considered in diffuse lesions with small reference vessel size.