
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-191
Precision in Ostial LAD CTO Stenting: How IVUS Technology Shapes the Future of PCI
By Faiz Mashood, David Yong, Ong Siew Hoon, Goay Swee En, Teoh Chee Kiang, Rafidah Abu Bakar, Amin Ariff Nuruddin
Presenter
Faiz Mashood
Authors
Faiz Mashood1, David Yong1, Ong Siew Hoon1, Goay Swee En1, Teoh Chee Kiang1, Rafidah Abu Bakar1, Amin Ariff Nuruddin1
Affiliation
National Heart Institute, Malaysia1,
View Study Report
TCTAP C-191
Coronary - Imaging & Physiology - Invasive Imaging (IVUS, OCT, NIRS, VH, etc)
Precision in Ostial LAD CTO Stenting: How IVUS Technology Shapes the Future of PCI
Faiz Mashood1, David Yong1, Ong Siew Hoon1, Goay Swee En1, Teoh Chee Kiang1, Rafidah Abu Bakar1, Amin Ariff Nuruddin1
National Heart Institute, Malaysia1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
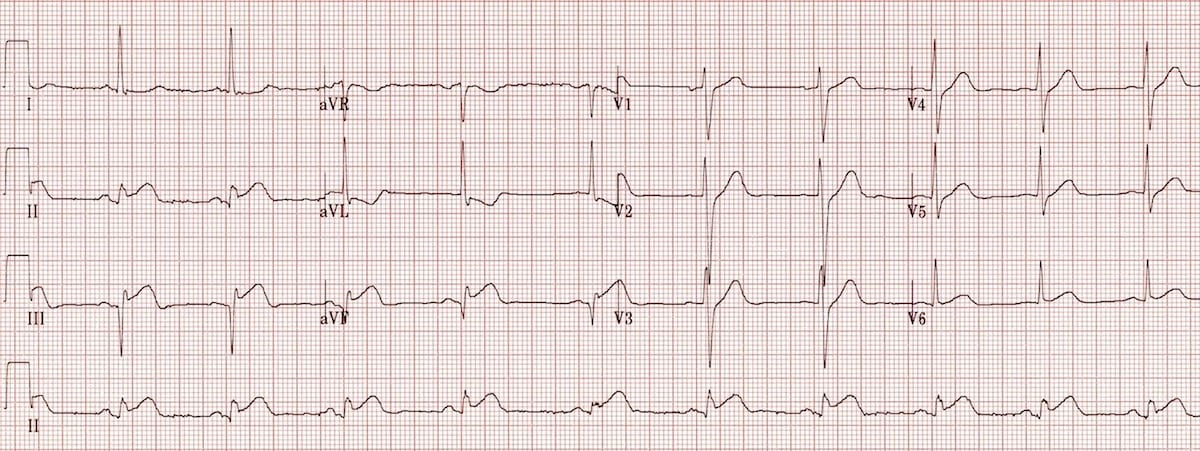
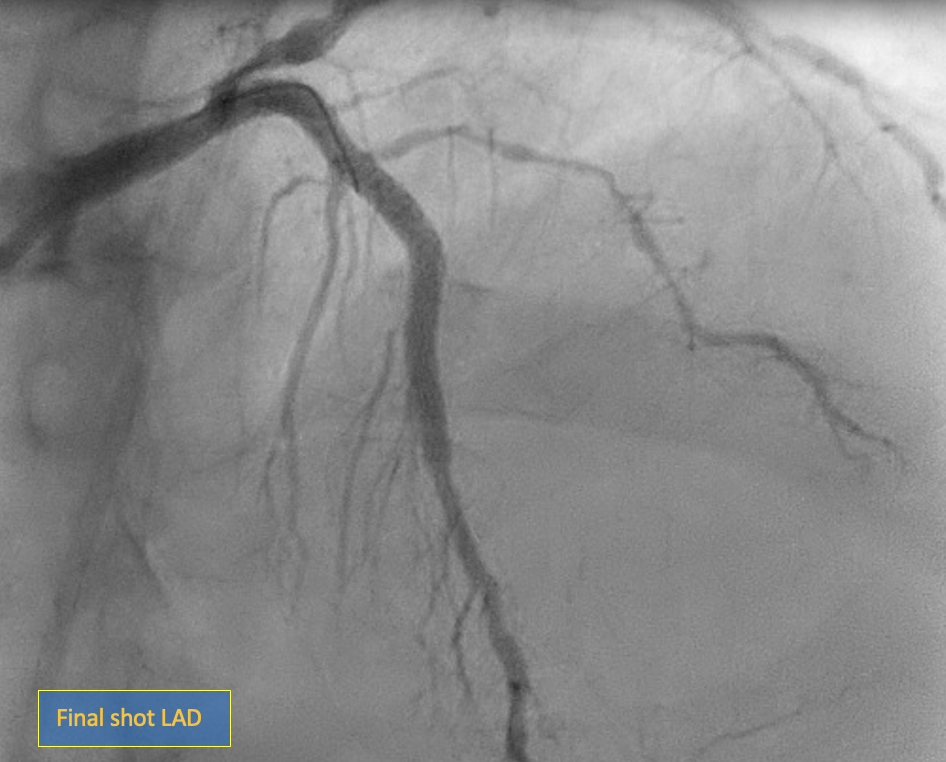
A 61-year-old man with a recent inferior myocardial infarction and a history of diabetes, hypertension, and dyslipidemia presented with 3-vessel disease, including a chronic total occlusion (CTO) of the proximal LAD. After primary PCI on the RCA, he underwent staged PCI for the LAD CTO and proximal LCx. Using IVUS guidance, PCI was successfully performed with drug-eluting stents in the LAD and a drug-coated balloon in the LCx. The final angiography showed TIMI 3 flow, excellent stent apposition.
Relevant Test Results Prior to Catheterization
-
Relevant Catheterization Findings
Left main : distal mild disease
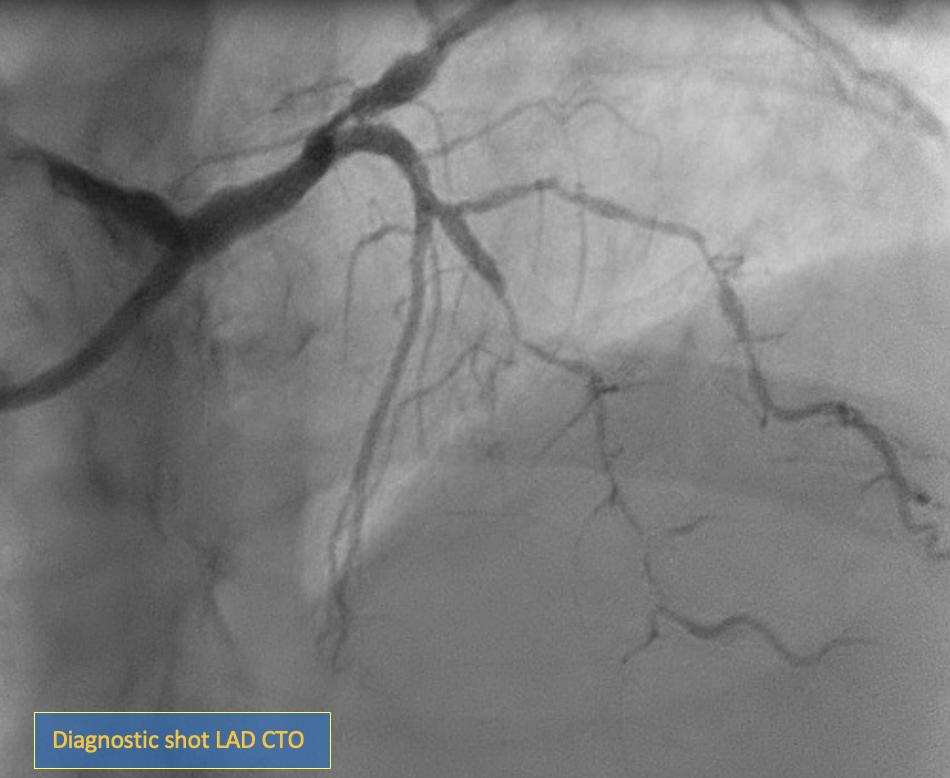
LAD : proximal LAD CTO with tapered end
LCx : ostial to proximal LCX 90% stenosis
RCA : patent stent
Interventional Management
Procedural Step
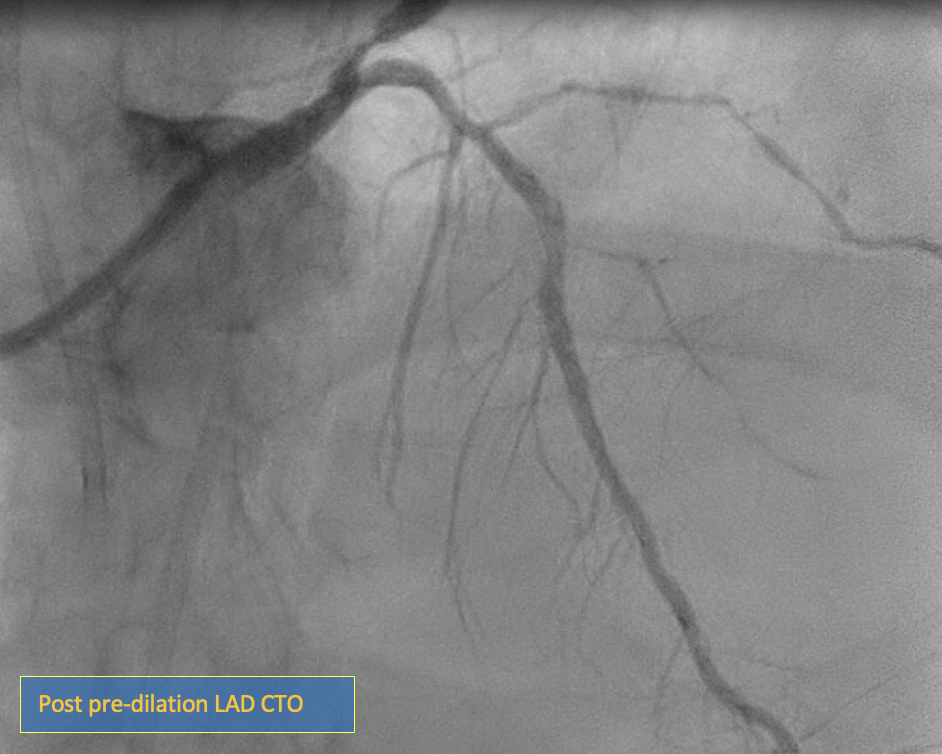
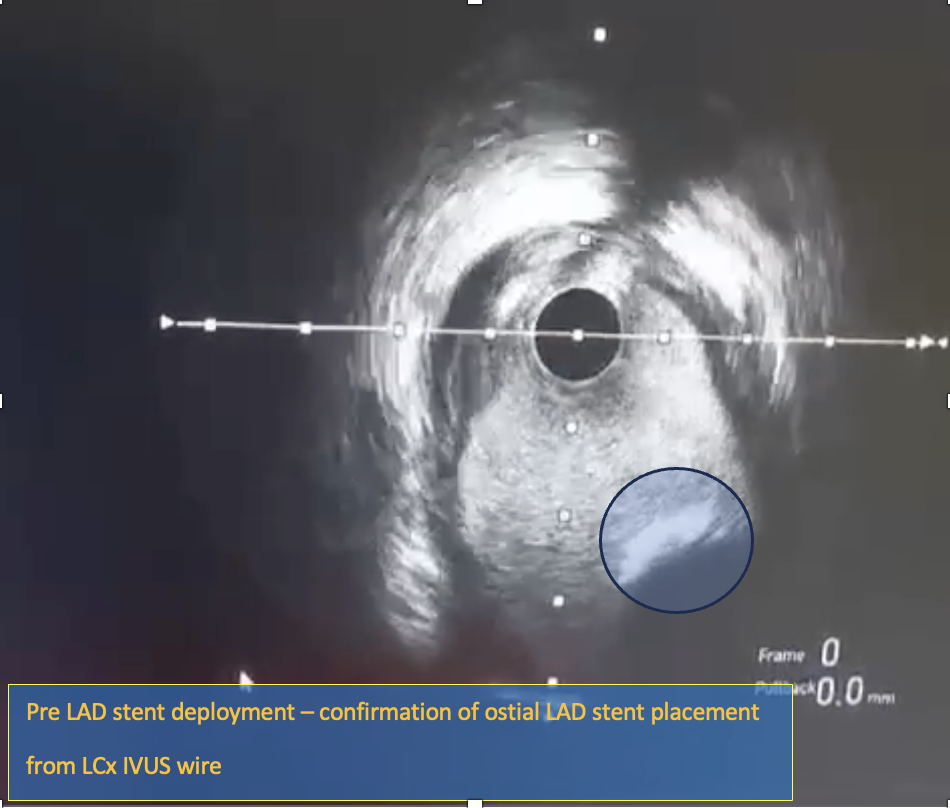
Engagement with an EBU 3.5 / 7F catheter was established in the left coronary sinus. A femoral puncture was performed using a JR 3.5 / 6F catheter to evaluate collateral circulation. Initial attempts to advance a Fielder XT wire and Corsair Pro microcatheter down to the LAD were unsuccessful, leading to a switch to a Pilot 200 wire. A retrograde angiogram from the RCA confirmed the wire was in the septal branch, prompting the use of a parallel wire technique with a Gaia II wire, which successfully navigated into the true lumen. Pre-dilation was conducted with a 1.0 x 5 mm semi-compliant balloon, followed by upsizing to a 2.0 x 15 mm balloon. Pre-IVUS was performed, resulting in the decision for sequential pre-dilation with a 2.5 x 15 mm scoring balloon. IVUS confirmed vessel size, stent length, and a minimal lumen area (MLA) of 3.37 mm. An initial 3.0 x 32 mm stent was delivered to the proximal LAD, followed by the placement of an ostial LAD stent measuring 3.5 x 28 mm, confirmed with IVUS. The IVUS images from LCx demonstrated stent strut positioning at the ostial LAD, with further verification obtained through two caudal angiographic views to ensure precise stent placement. The procedure was completed with a drug-coated balloon in the proximal LCx. The final angiographic shot revealed TIMI 3 flow with no flow-limiting dissections or perforations.
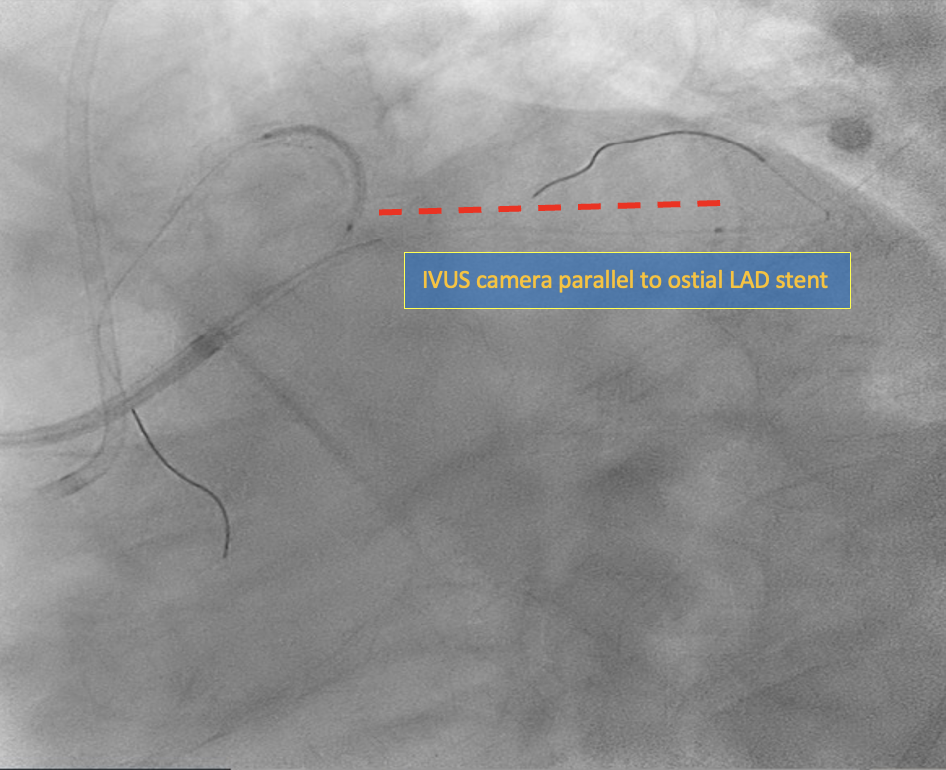
Case Summary
Achieving accurate ostial stent placement in coronary interventions remains challenging due to the difficulty in pinpointing the true anatomical ostium. Misplacement can lead to incomplete coverage or stent protrusion, increasing risks like restenosis and thrombosis. IVUS guidance offers a solution by providing real-time, high-resolution imaging to enhance stent positioning accuracy. While promising, IVUS use in this context isn’t yet standardized. Further research is needed to establish its efficacy and safety, potentially paving the way for IVUS-guided stenting to become part of clinical guidelines, improving patient outcomes.